Pharmacology 4th Ed – Tara V Shanbhag, Smita Shenoy
Pharmacology 4th Ed – Tara V Shanbhag, Smita Shenoy



🙂
Synonyms: Crown and bridge cement, Zinc oxyphosphate
APPLICATIONS:
Luting of restoration and orthodontic bands & brackets
Thermal insulation
Root canal restoration
High strength bases
Temporary restoration
CLASSIFICATION:
| PARTICLE SIZE | FILM THICKNESS | USE | |
| TYPE 1 | Fine | 25um | Luting |
| TYPE 2 | Medium | 40um | Luting, base |

SETTING OF THE CEMENT:
Phosphoric acid in the liquid dissolves zinc oxide and reacts with aluminium phosphate to form aluminium phosphate gel on the remaining undissolved zinc oxide particles.

SETTING TIME: 2.5 to 8 minutes
MANIPULATION:
It is an exothermic process.
Zinc oxide cement is dispensed on the glass slab and divided into 6 increments(1/16, 1/16, 1/8, 1/4, 1/4, 1/4). It is followed by dispensing of the liquid.
Mixing of the cement should be initiated by the smallest increment with a thin spatula. There should be brisk spatulation with large, wide circular motions to dissipate the heat.
When the spatula is drawn away from the mixture, a strand of 12-19 mm should be produced. Such cement is suitable for cementation.
MIXING TIME:
For each increment: 15-20 sec
Total mixing time: 1.5-2 min
PROPERTIES:
MECHANICAL PROPERTIES: Compressive strength = 104 MPa, Tensile strength = 5.5 MPa, Elastic modulus = 13 GPa
SOLUBILITY: Less soluble in water (0.06%). Soluble in lactic, acetic and citric acids (in-vivo)
ADHESION TO TOOTH: Mechanical bonding ( In case of application of a cavity liner before applying zinc phosphate, it does not bond well due to less retention as it will create smoother surface with less interlocking)
BIOLOGICAL PROPERTIES: Phosphoric acid is acidic and cytotoxic. Younger patients are more susceptible to it because of more open dentinal tubules. Older patients with sclerotic dentin have a tortuous path for the entry of acid.

The biological considerations of dental materials cannot be isolated from their physical properties.
Biological requirements of Dental Materials
A dental material should:
2. Be non-irritant to the oral or other tissues.
3. Not produce allergic reactions.
4. Not be mutagenic or carcinogenic.

Examples of hazards from chemicals in Dental Materials
✔Some dental cements are acidic and may cause pulp irritation.
✔Polymer based filling materials may contain irritating chemicals such as unreacted monomers, which can irritate the pulp.
✔Phosphoric acid is used as an etchant for enamel.
✔Mercury is used in dental amalgam, mercury vapor is toxic.
✔Dust from alginate impression materials may be inhaled, some products contain lead compounds.
✔Monomer in denture base materials is a potential irritant.
✔Some people are allergic to alloys containing nickel.
✔During grinding of beryllium containing casting alloys, inhalation of beryllium dust can cause berylliosis.
✔Some dental porcelain powders contain uranium.
✔Metallic compounds (e.g. of lead and tin) are used in elastomeric impression materials.
✔Eugenol in impression pastes can cause irritation and burning in some patients.
✔Laboratory materials have their hazards, such as: cyanide solution for electroplating, vapours from low fusing metal dies, siliceous particles in investment materials, fluxes containing fluorides, and asbestos.
✔Some periodontal dressing materials have contained asbestos fibres.
REFERENCES:
1.Textbook of Dental Materials – John J Manappallil
2.Images – Google

🎯 GOALS…
⭐ BENEFITS ⭐
REFERENCE:- STURDEVANTS – CONS. DENTISTRY
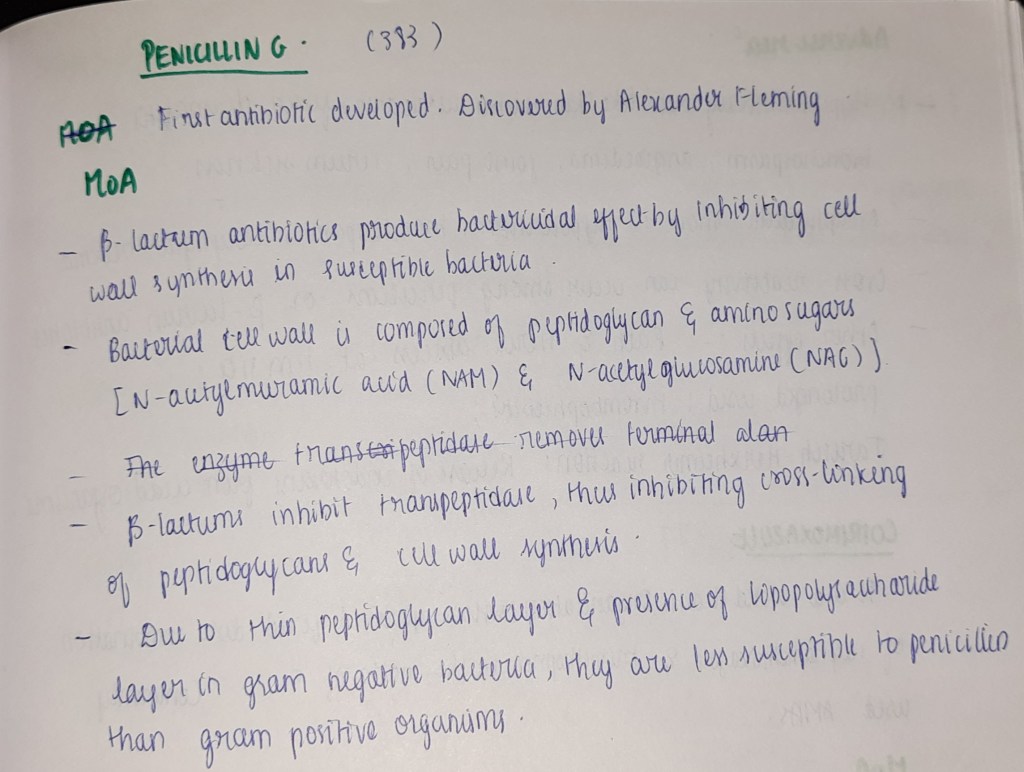
The cell wall is a tough and rigid structure surrounding the bacterium like a shell. It weighs about 20-25% of the dry weight of the cell.
FUNCTIONS:
1.Shape
2. Protection against osmotic damage
3.Rigidity
4.Cell division
5.Possesses target site for antibiotics, lysozymes and bacteriophages. Carries bacterial antigens that are important in virulence and immunity.
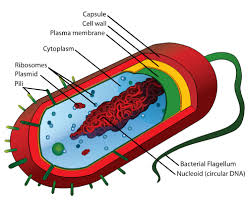
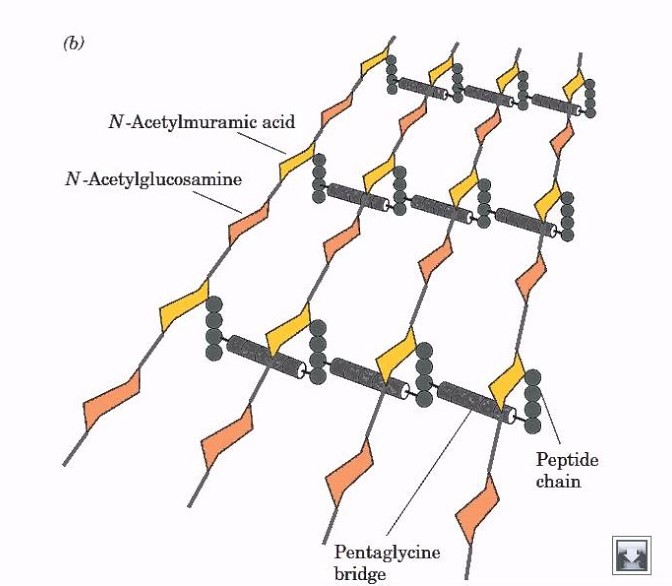
The rigid part of the cell wall is a peptidoglycan which is a mucopeptide (murein) composed of N-acetyl muramic acid and N-acetyl glucosamine molecules alternating in chains, cross-linked by peptide sub-units.
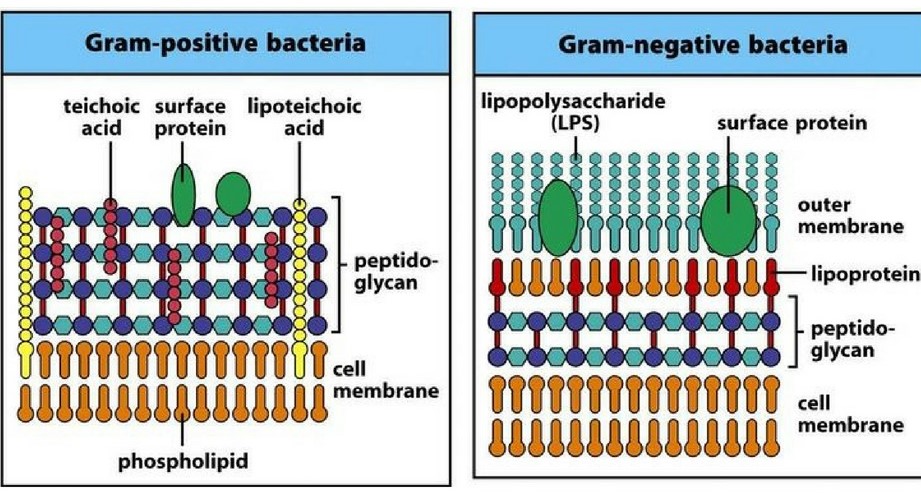
DIFFERENCES BETWEEN GRAM POSITIVE AND GRAM NEGATIVE CELL WALL
| CHARACTER | GRAM POSITIVE | GRAM NEGATIVE |
| Thickness | 20-80nm | 10nm |
| Periplasmic space | Absent | Present |
| Lipids and Glycoproteins | Few(0.3%) | Many(58%) |
| Teichoic acid | Present | Absent |
| Peptidoglycan | <15% | 10-20% |
| Gram’s reaction | Violet | Pink |
| Outer membrane | Absent | Present |
| Lipopolysaccharides | Absent | Present |
DEMONSTRATION OF CELL WALL
1.Plasmolysis
2,Microdissection
3.Differential staining
4.Reaction with specific antibody
5.Electron microscopy
BACTERIA WITH DEFECTIVE CELL WALL
PLEOMORPHISM AND INVOLUTION FORMS
Certain species of bacteria exhibit great variation in shape and size of individual cells are called pleomorphic bacteria.
Some bacteria show swollen and aberrant forms in ageing laboratory cultures and are known as involution forms.
Defective cell wall synthesis is responsible for development of these two forms 🙂
SOURCE: MICROBIOLOGY – C.P BAVEJA
