

References: Shafer’sTextbook Of Oral Pathology
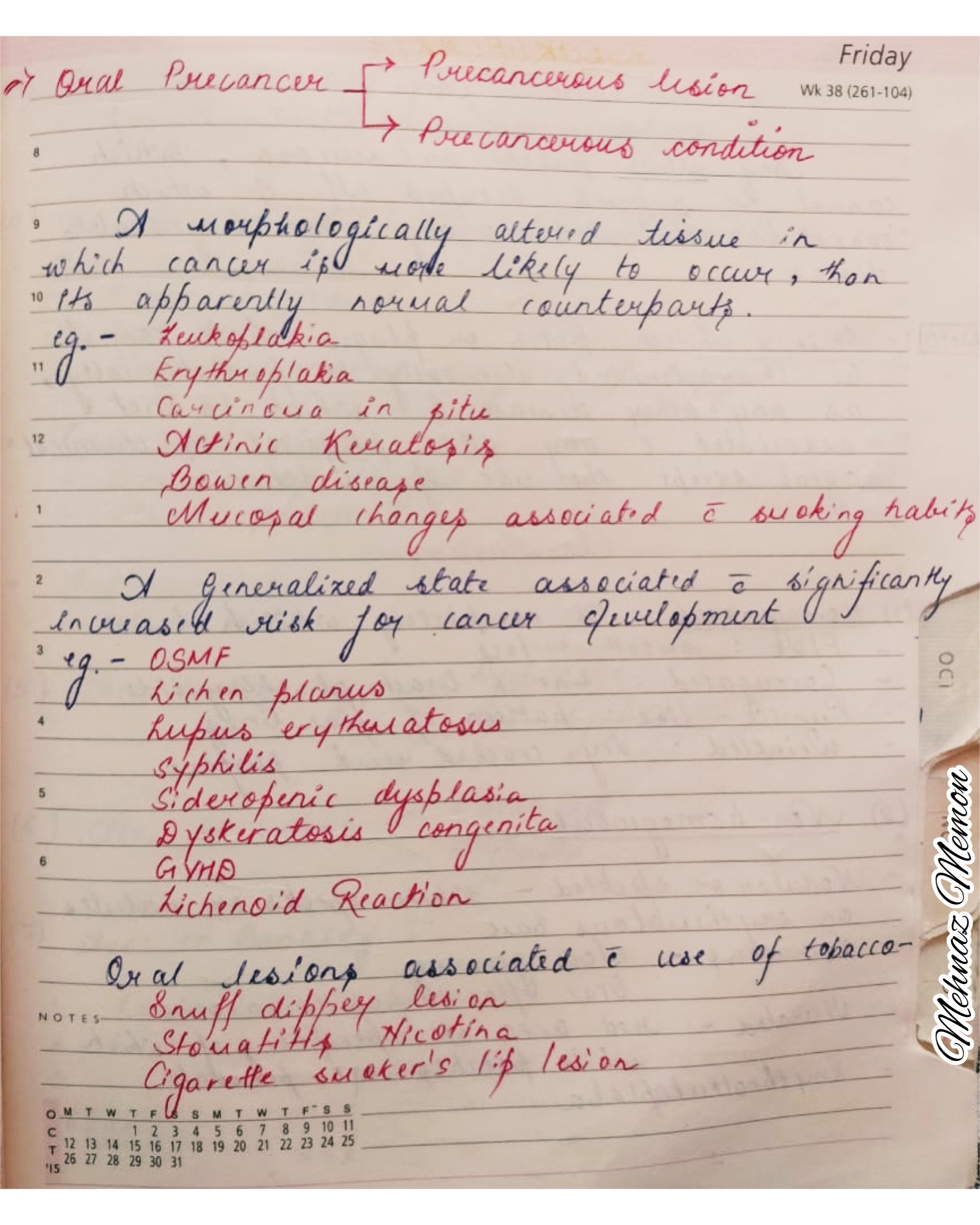
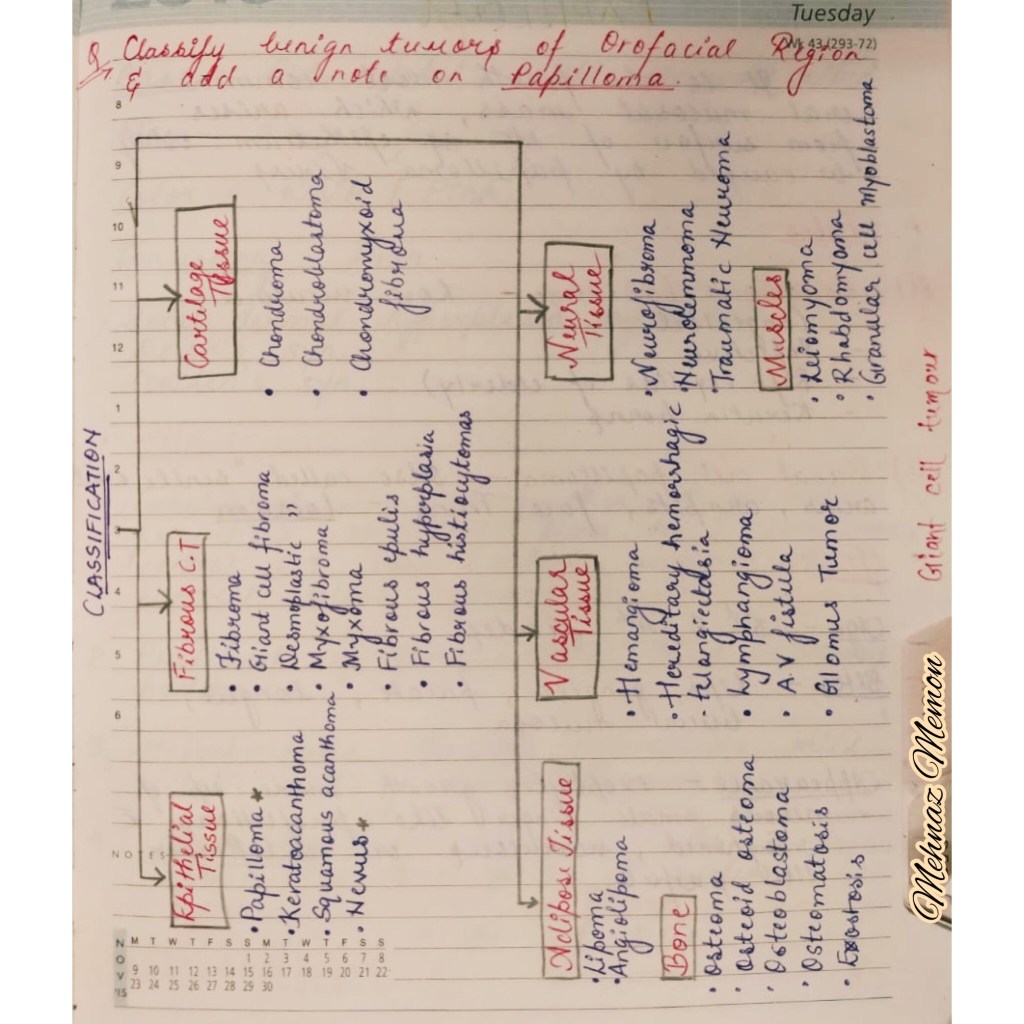
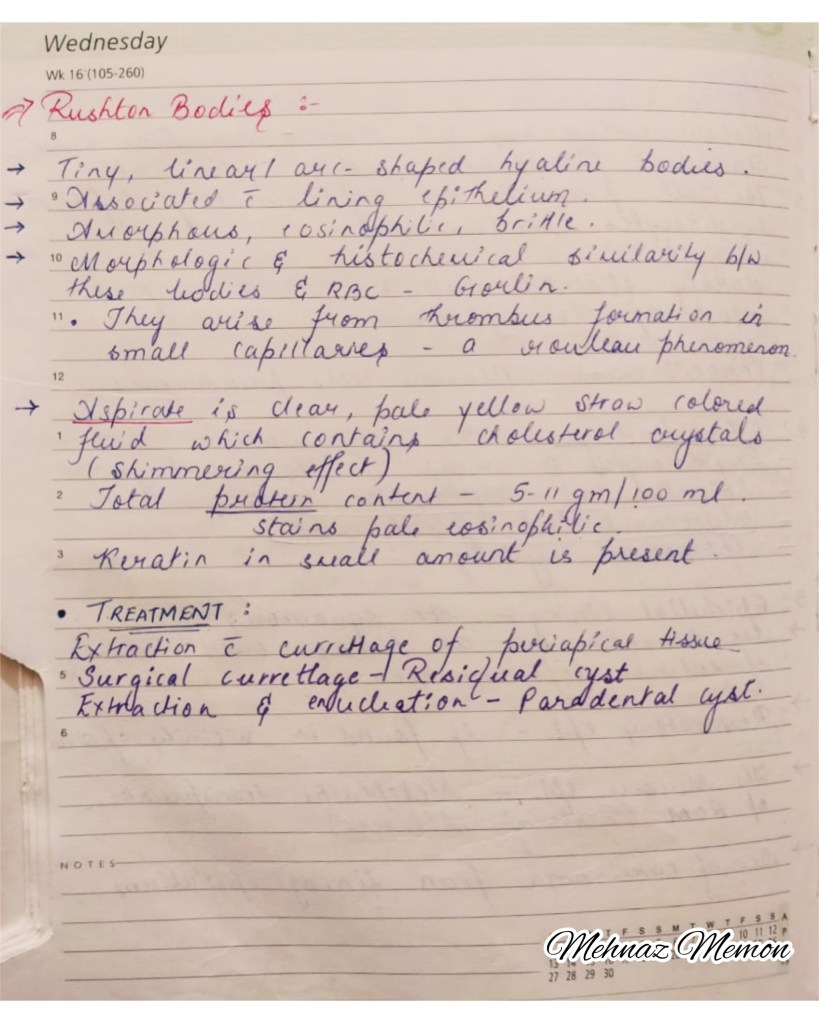
Precancerous lesions & conditions shortlisted..👆🏻
References: Shafer’sTextbook Of Oral Pathology
Source: Internet


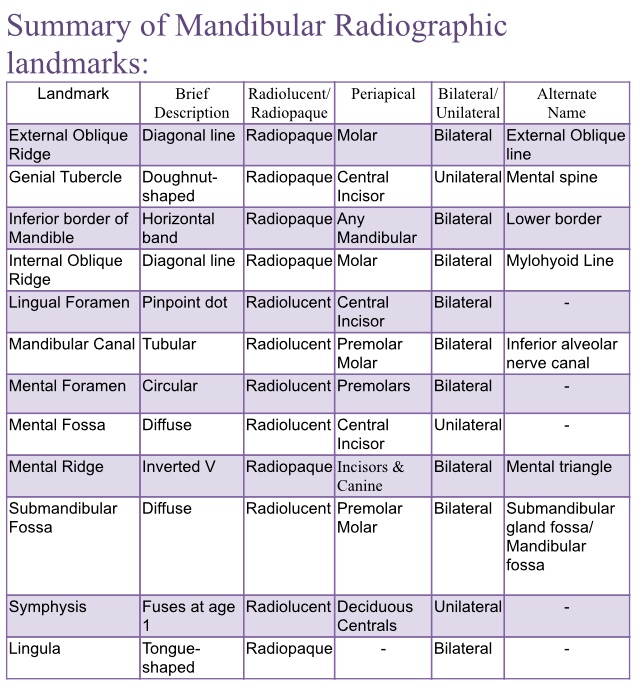
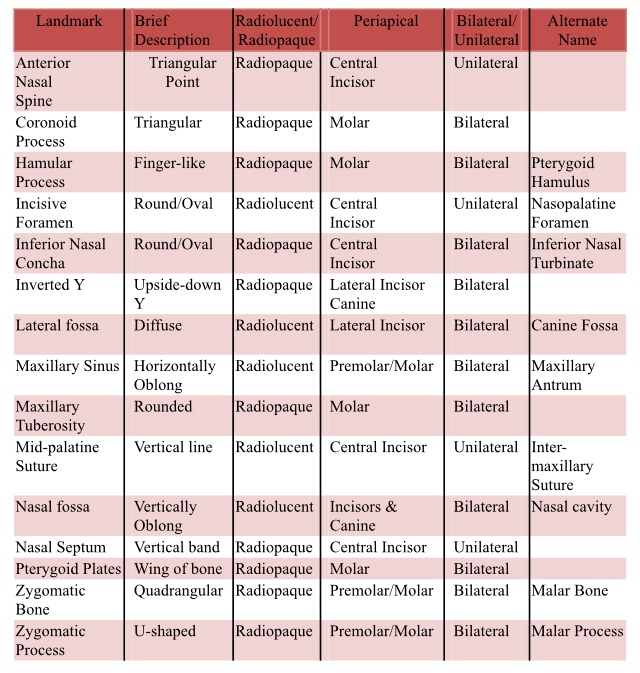
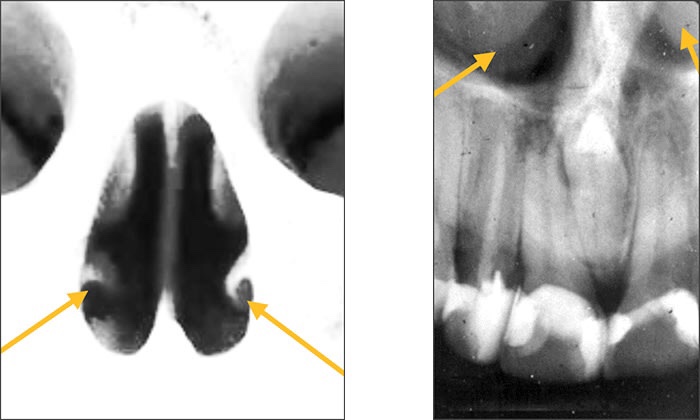
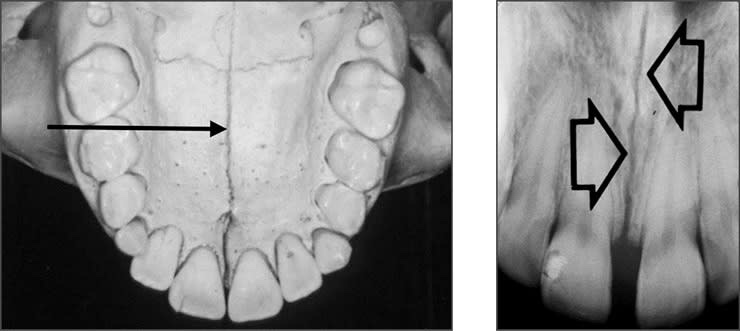
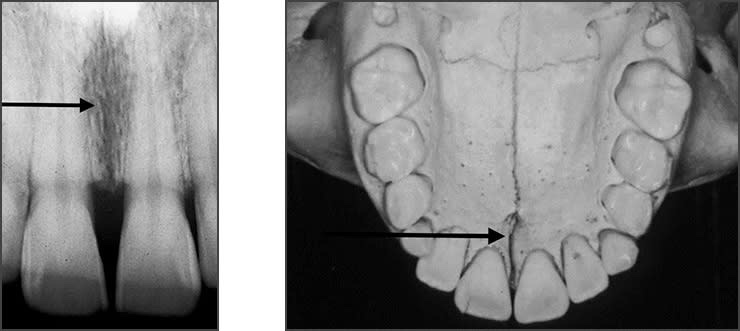
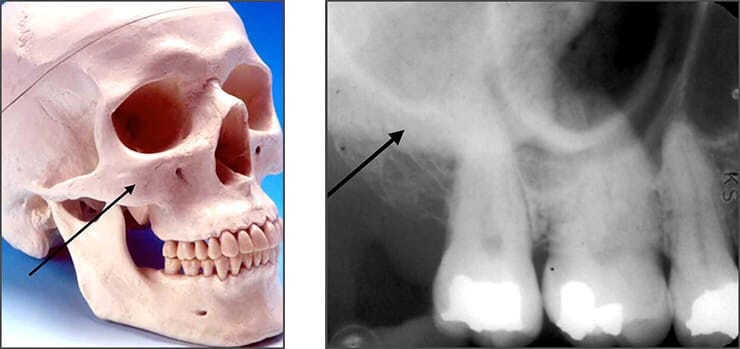
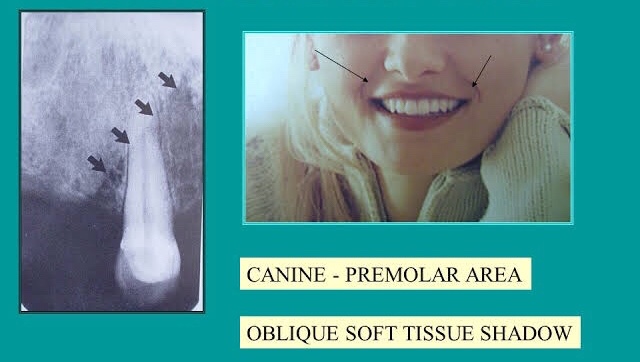
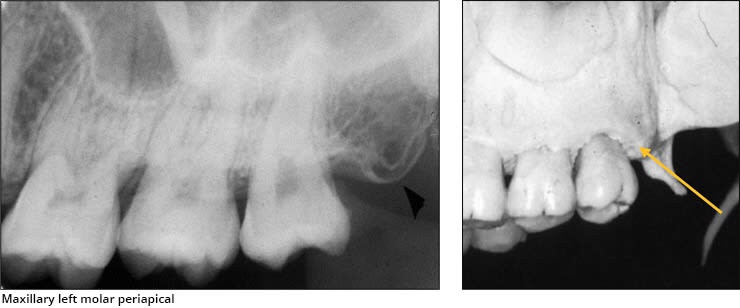
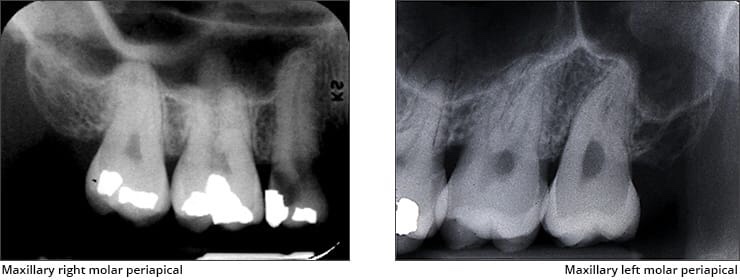
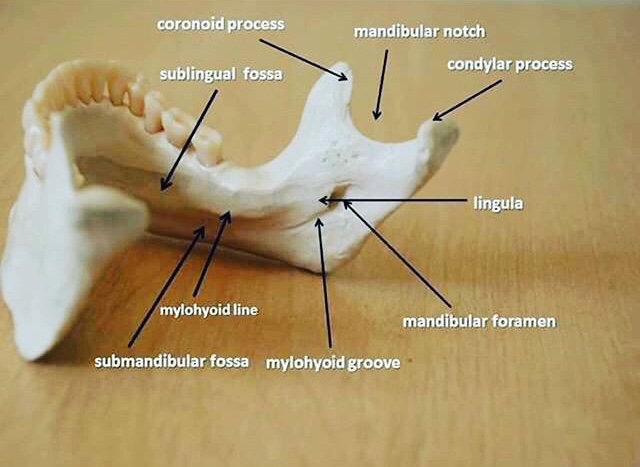
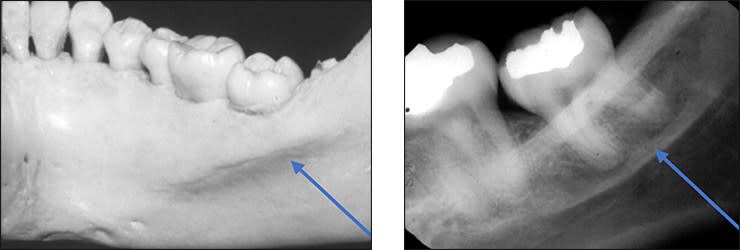
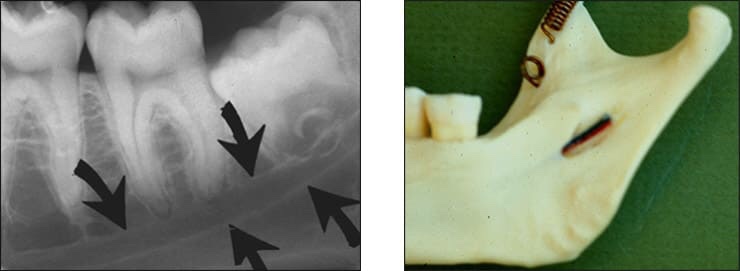
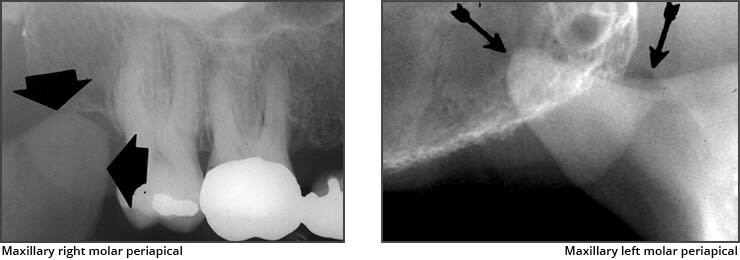
Radiolucent vs. Radiopaque
➡️ Structures that are cavities, depressions or openings in bone such as a sinus, fossa, canal or foramen will allow x-rays to penetrate through them and expose the receptor. These areas will appear radiolucent or black on radiographic images.
➡️ Structures that are bony in origin absorb or stop the penetration of the x-rays and, therefore, do not reach the receptor. These areas appear radiopaque or white on radiographic images. Some structures partially absorb radiation and are represented in varying degrees of radiopacity.





















References: https://www.dentalcare.com/en-us/professional-education/gail-f-williamson


References: Shafer’sTextbook Of Oral Pathology
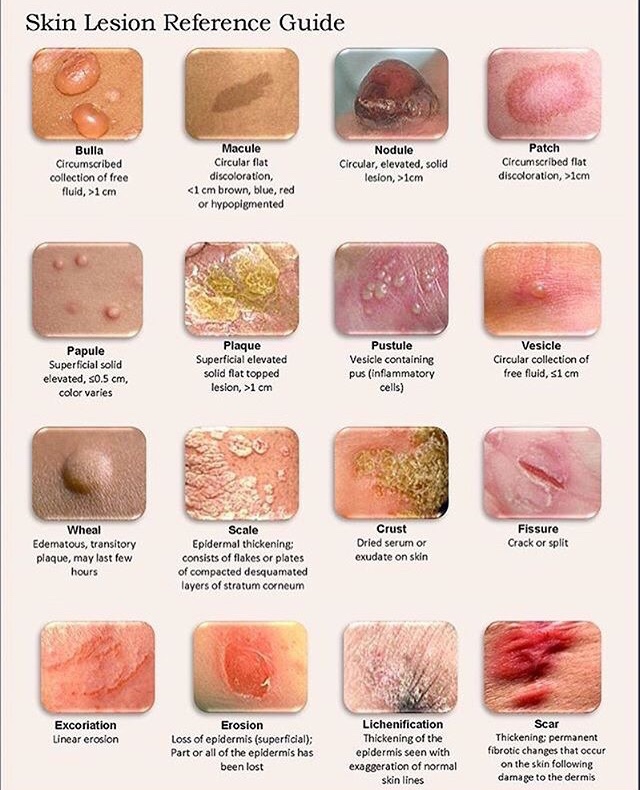
Pemphigus describes a group of chronic bulbous diseases (Wichman) of the skin, characterized by the appearance of vesicles & bullae (fluid-filled intradermal blisters) that develop in cycles.
➡️ A auto-immune blistering disease of the skin & mucous membrane. Finding of IgG antibody directed against the cell surface of keratinocytes is seen.
➡️ 3 primary subsets of pemphigus include –
➡️ Associated factors:
An acronym has been suggested from the name of the disease, PEMPHIGUS, to encompass those factors:
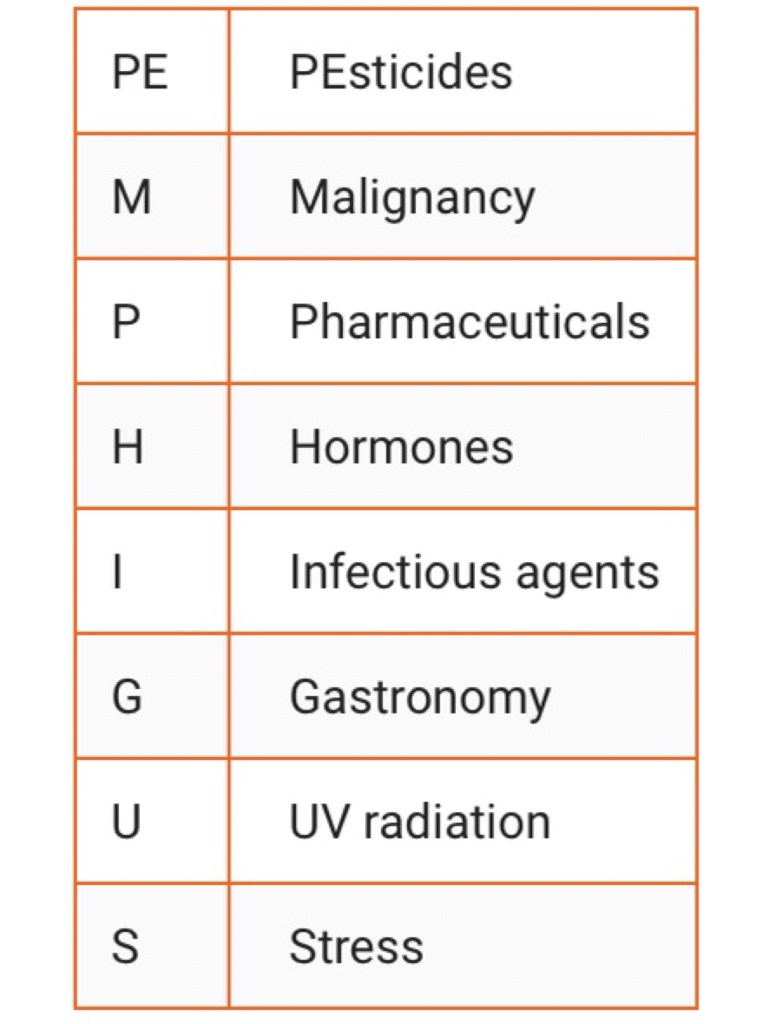
1. Drugs: The inciting medications can be classified based on their chemical structure, with the main groups being thiols drugs, phenol drugs, and non-thiol/phenol drugs. The most common offending drugs include D-penicillamine, captopril, and penicillin.
2. Diet: Once the drug-induced pemphigus has developed, besides discontinuing the drug, the nurse or physician should educate the patient on a recommended diet. Certain foods contain phenols and thiols that can exacerbate the condition. Thus a dietary consult is necessary. Foods that contain phenol and thiol like compounds include chives, garlic, onion, black pepper, cashew, and mangoes.
3. Infection: The most frequently incriminated infectious agents are the viruses of the herpetoviridae family, namely herpes simplex, EBV, CMV, and even HH8.
4. Auto-immune diseases
5. UV Radiation
6. Stress: Avoiding emotional stress may be therapeutic in pemphigus patients, hastening the healing process and reducing or stopping the use of immunosuppressive drugs.
Pathogenesis:
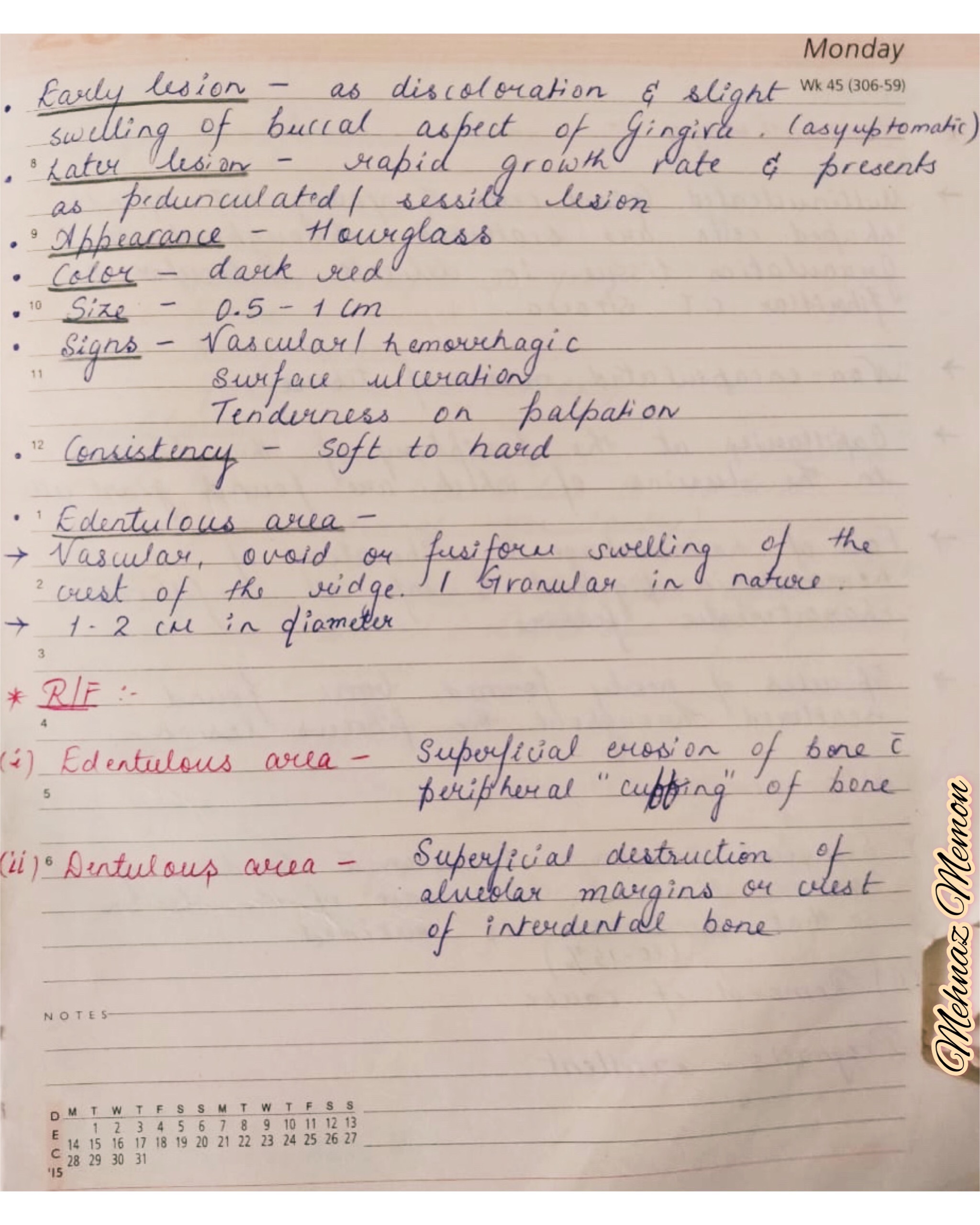
Clinical features:
➡️ Uncommon variant of Pemphigus Vulgaris – P. Vegetans
Oral Manifestations:

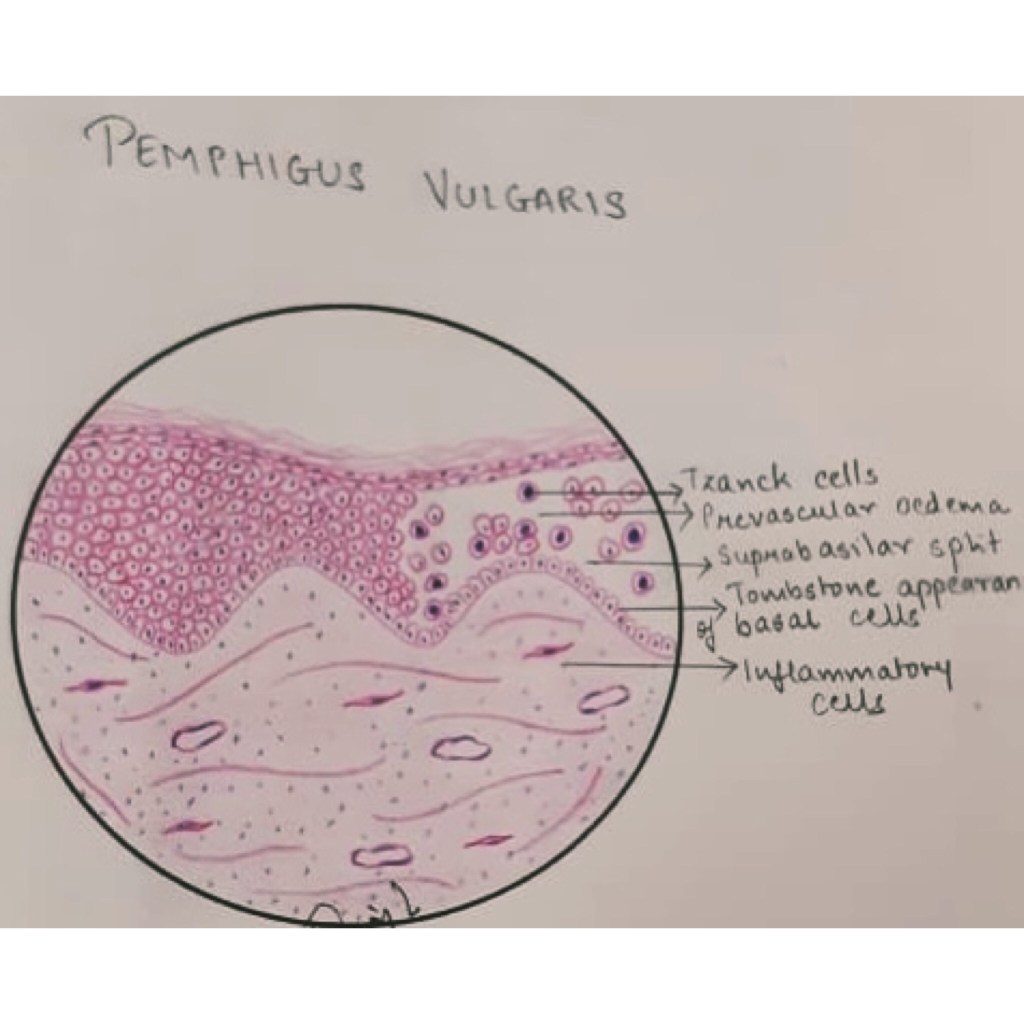
Histopathology:
Evaluation:
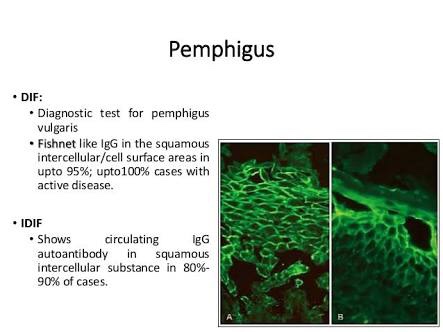
Immunofluorescent testing:
Management:
Differential Diagnosis:
References: Shafer’sTextbook Of Oral Pathology; Internet