Most Prevalent Chronic Disease.
CAVITY…???💬
Yes! A early carious lesion develops when demineralization wins over Remineralization over time.




References: Shafer’sTextbook Of Oral Pathology
CAVITY…???💬
Yes! A early carious lesion develops when demineralization wins over Remineralization over time.
References: Shafer’sTextbook Of Oral Pathology
Development of chancre at site of inoculation. Usually Solitary in nature.
Intra-orally,
➡️ The chancre is an ulcerated lesion covered by grayish white membrane, painful due to secondary infection.
➡️ Sites:

Microscopically:-
Heals: 3 weeks – 2 months


➡️ Most characteristic & important lesion of syphilis due to endarteritis obliterans.

➡️ In syphilitic glossitis, the surface of the tongue gets broken up by fissures due to atrophy.
White patches on tongue – Tertiary Syphilis
Due to vasculitis & endarteritis, there’s circulatory deficiency to the lingual papillae
⬇️
Atrophy of filiform & fungiform papillae
⬇️
Bald, smooth, lingual surface
⬇️
Leukoplakic involvement (Dysplastic type)
References: Shafer’sTextbook Of Oral Pathology, Image source: Google

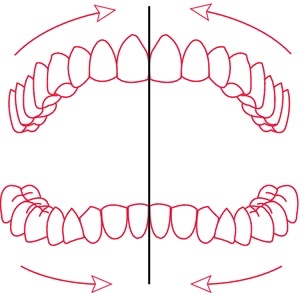
➡️ Intra-arch malocclusions that include variations in individual tooth position and malocclusions affecting a group of teeth within an arch. Intra arch malocclusions can also include condition like spacing or crowding within the dental arch.

Brief Description:







References: Textbook of Orthodontics The Art and Science 6th Edition By Bhalajhi!
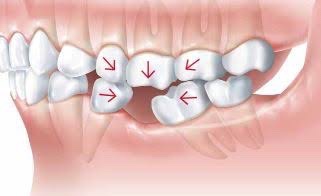
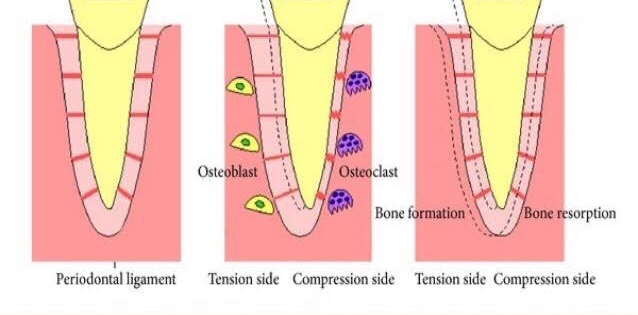
➡️ Orthodontic tooth movement is a unique process where a solid object (teeth) is made to move through a solid medium (bone).
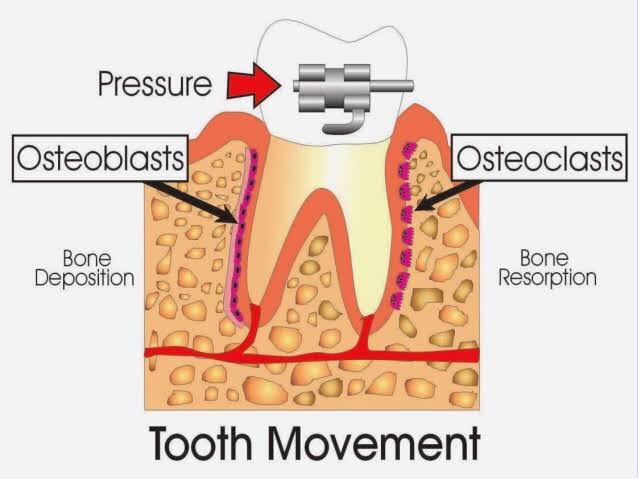
➡️ Orthodontic treatment is possible due to the fact that whenever a prolonged force is applied on a tooth, bone remodeling occurs around the tooth resulting in its movement.
➡️ Physiologic tooth movements are naturally occurring tooth movements that take place during and after tooth eruption. They include:
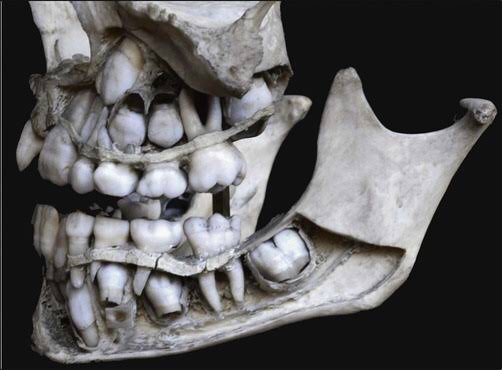
➡️ Tooth eruption is the axial movement of the tooth from its developmental position in the jaw to its final position in the oral cavity. A number of theories have been put forward to explain how the eruption process take place.
a. Blood pressure theory: According to this theory, the tissue around the developing end of the root is highly vascular. This vascular pressure is believed to cause the axial movement of the teeth.
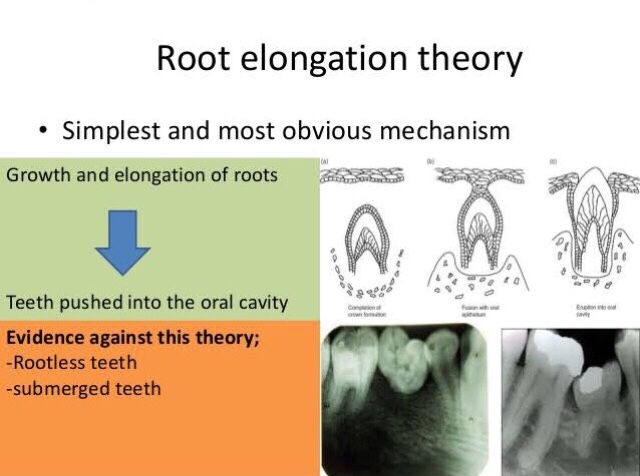
b. Root growth: According to the proponents of this theory, the apical growth of root results in an axially directed force that brings about the eruption of the teeth. This theory has not been accepted. Teeth move a greater distance during eruption than the increase in root length. In addition the onset of root growth and eruption do not seem to coincide. Teeth that are malformed and lack roots also erupt in a no. of cases.
c. Hammock ligament: According to Sicher, a band of fibrous tissue exists below the root apex spanning from one side of the alveolar wall to the other. This fibrous tissue appears to form a network below the developing root and is rich in fluid droplets. The developing root forces itself against this band of tissue, which in turn applies an occlusally directed force on the tooth.
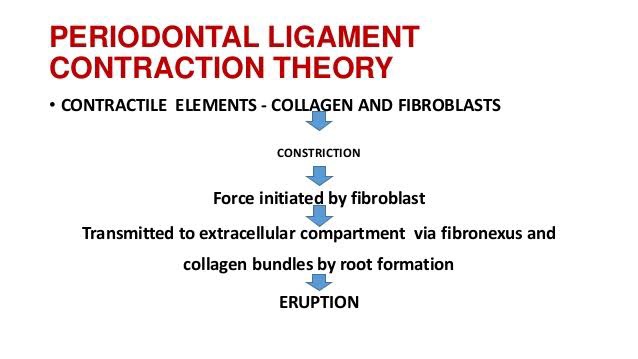
d. Periodontal ligament traction: This theory states that the periodontal ligament is rich in fibroblasts that contain contractile tissue. The contraction of these periodontal fibres result in axial movement of the tooth.
➡️ During mastication, the teeth and periodontal structures are subjected to intermittent heavy forces, which occur occur in cycles of one second or less and may range from 1-50 kg based on the type of food being masticated. A tooth subjected to these heavy forces, exhibits slight movement within its socket and subsequently returns to its original position as soon as the load is removed.
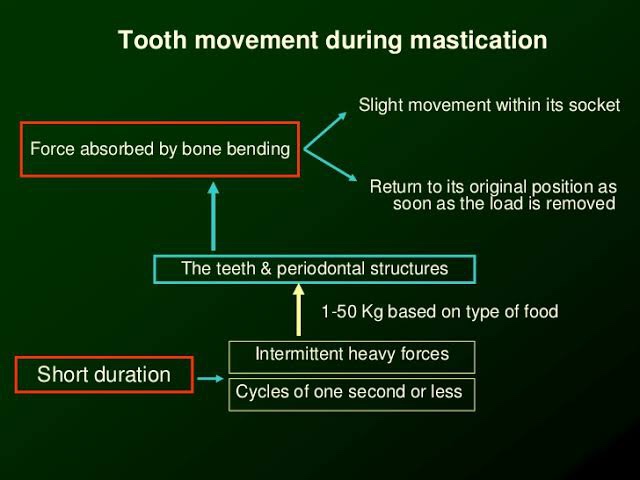
➡️ When a tooth is subjected to such heavy forces, the tissue fluid present in the periodontal space, being incompressible, prevents major displacement of the tooth within the socket. Therefore the forces are transmitted through the tissue fluids to the adjacent alveolar bone. Recent studies have shown that the alveolar bone can bend in response to heavy masticatory forces.
➡️ Whenever the forces of mastication are sustained and are more than the usual one second cycle, the periodontal fluid is squeezed out and pain is felt as the tooth is displaced into the PDL space.
References: Textbook of Orthodontics The Art and Science 6th Edition By Bhalajhi!…Image source: Google




References: Shafer’sTextbook Of Oral Pathology, Textbook of Pathology, Harsh Mohan; Random google Images
References: Textbook of Oral medicine by Ghoms