One-line takeaway: The quad-helix produces significant, stable maxillary expansion (mean +5.3 mm intermolar, +4.1 mm intercanine) with midpalatal suture opening in both deciduous and mixed dentitions — with no significant difference between the two groups.
Why Early Maxillary Expansion Matters
Functional posterior crossbite is commonly associated with a transverse maxillary deficiency. In such cases, the mandible often shifts laterally during closure to avoid occlusal interference. This functional shift can lead to several secondary problems, including:
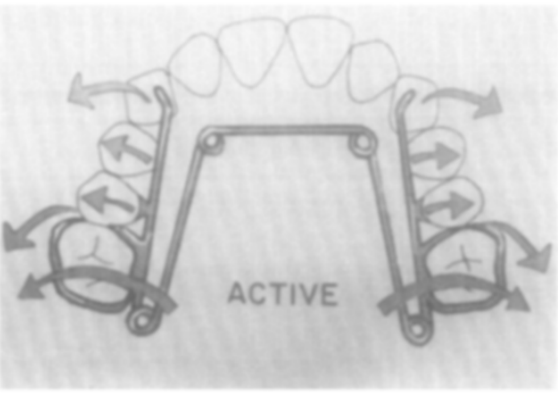
The quad-helix appliance is essentially a modification of the W-arch appliance, with the addition of four helices. These helices provide greater flexibility and allow a wider range of activation compared with traditional lingual arch expansion appliances.
Typically, the appliance is fabricated from 0.036-inch stainless steel wire and soldered to bands placed on the maxillary molars. The helices act as force modulators, delivering low, continuous expansion forces to the maxillary arch.
The quad-helix is a W-arch modification with 4 helical loops incorporated. These loops deliver four specific advantages over a standard W-arch:
Refined adjustment capability — fine-tune forces without full removal
💡 Exam Distinction: Quad-helix = slow/continuous expansion vs. jackscrew = rapid expansion. Both open the midpalatal suture, but quad-helix produces more physiologic bone remodeling with less relapse risk.
↑ Range of force application — stores energy over greater activation distances
↑ Flexibility — lighter, continuous, physiologic force
The typical treatment protocol involves an initial activation that produces a modest transverse expansion force. The patient is then monitored periodically, and adjustments are made only when expansion progress slows.
General clinical steps include:
Cementing the appliance onto molar bands.
Activating the appliance to produce expansion equivalent to approximately half the buccolingual width of the molars.
Monitoring the patient weekly or periodically during the active expansion phase.
Achieving slight overexpansion so that the lingual cusp of the maxillary molar contacts the buccal cusp slope of the mandibular molar in centric relation.
Maintaining the appliance in a passive state for a retention period.
The entire active phase of expansion typically lasts about one month, followed by a retention period of approximately six weeks.
📊 Treatment Course Data
Variable
Deciduous (x̄ 5y 3m)
Mixed (x̄ 8y 2m)
Correction time (days)
28.8 ± 4.9
31.8 ± 5.9
Retention time (days)
44.2 ± 1.8
45.2 ± 1.7
Total appliance time (days)
73.0 ± 5.9
77.0 ± 6.0
No. of adjustments
1.2 ± 0.4
1.0 ± 0.3
Midpalatal suture opening
✅ All subjects
✅ All subjects
Between-group significance
NS (p > 0.05)
← same
Memory hook: “30-45-75” — ~30 days active, ~45 days retention, ~75 days total.
📐 Transverse Dimensional Changes (The Core Data)
Measurement
Deciduous — Intercanine
Deciduous — Intermolar
Mixed — Intercanine
Mixed — Intermolar
Before treatment (mm)
27.5 ± 0.4
31.0 ± 0.4
29.3 ± 0.9
35.3 ± 2.0
Post-retention (mm)
31.4 ± 0.9
36.7 ± 0.6
33.7 ± 1.1
40.2 ± 1.2
3-month recall (mm)
29.8 ± 0.4
34.8 ± 0.4
31.5 ± 1.0
38.9 ± 1.5
Expansion increase
+3.9 ± 0.8
+5.7 ± 0.5
+4.4 ± 0.7
+4.8 ± 1.3
Relapse
−1.6 ± 0.9
−1.9 ± 0.3
−2.2 ± 0.3
−1.2 ± 0.4
Net gain
+2.3 ± 0.4
+3.9 ± 0.5
+2.2 ± 0.6
+3.6 ± 1.1
Significance (p)
< 0.01
< 0.001
< 0.01
< 0.02
Overall pooled means (both groups combined):
Intermolar expansion: +5.3 mm → net gain after relapse: ~+3.75 mm
Intercanine expansion: +4.1 mm → net gain after relapse: ~+2.25 mm
🔬 Sutural Opening — The Radiographic Finding
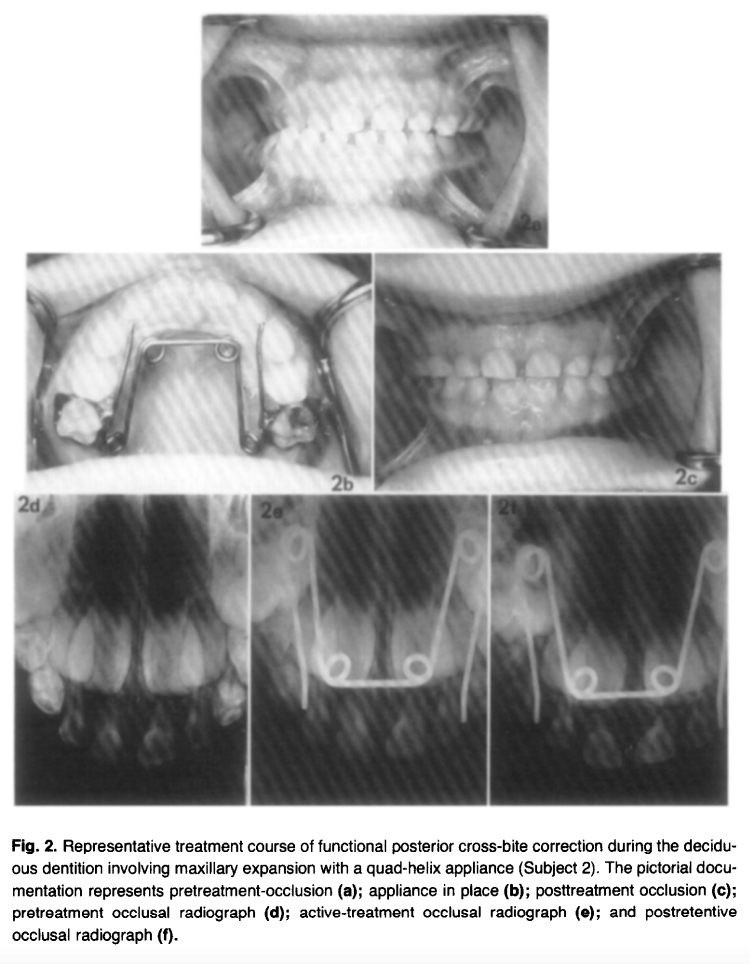
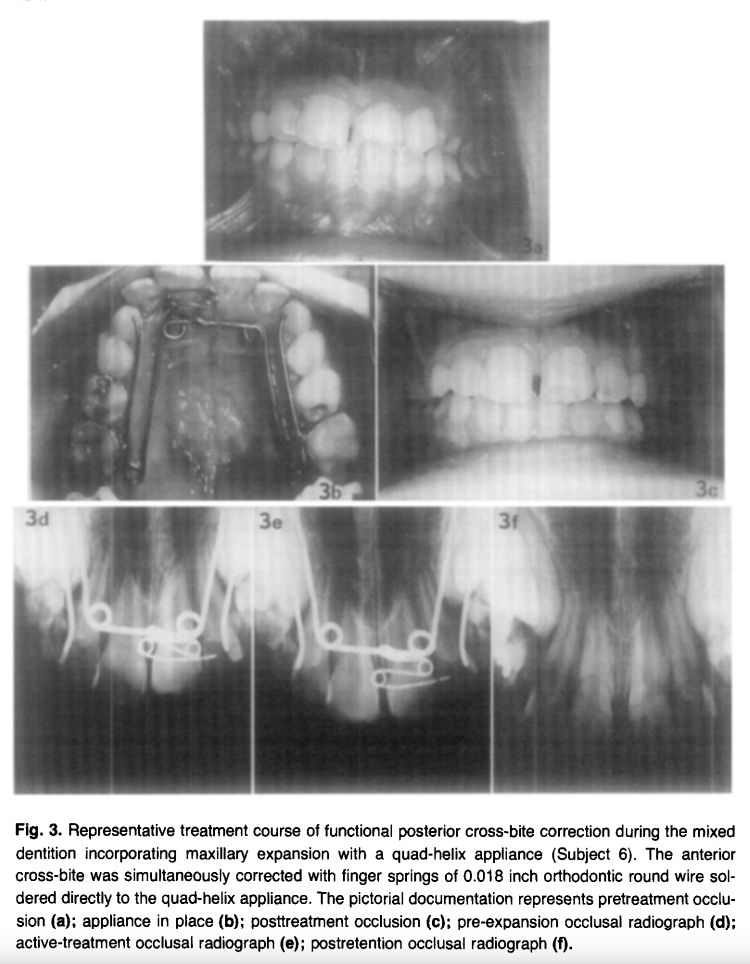
Every single subject (10/10) showed radiographic evidence of midpalatal suture opening on occlusal radiographs taken at 2 weeks of active treatment. The separation pattern was greatest anteriorly with a progressive posterior decrease — a classic sutural opening pattern. By end of retention, suture widening was no longer detectable radiographically, confirming bone fill-in.
📌 Exam alert: This finding proved the quad-helix produces orthopedic effects, not purely orthodontic tooth tipping — especially relevant in younger patients. This was the key debate this study addressed (W arch/Porter arch were thought to be purely orthodontic appliances).
↩️ Relapse & Overexpansion Protocol
Relapse averaged ~2 mm in both intercanine and intermolar dimensions after the 3-month post-retention period. The protocol to handle this:
Overexpand by 2–3 mm during active phase — lingual cusp tip contacts buccal cusp slope of mandibular molars bilaterally in centric relation
This slight overcorrection compensates for tooth uprighting relapse once appliance is removed
Slow expansion → more physiologic sutural remodeling → less relapse than rapid palatal expansion
⚡ Rapid vs. Slow Expansion
Feature
Quad-Helix (Slow)
RPE/Jackscrew (Rapid)
Force type
Low, continuous
High, intermittent
Suture opening
✅ Yes (both dentitions)
✅ Yes
Orthopedic effect
Present (especially young)
Dominant
Orthodontic effect
Present (tooth tipping)
Present
Relapse
Lower
Higher
Adjustments needed
~1.1 (minimal)
Multiple activations daily
Patient compliance
Not required
Device-dependent
Total treatment time
~75 days
3–6 months incl. retention
Berlocher et al. (RPE comparison): intermolar +4.2 mm, intercanine +3.8 mm using RPE — comparable to quad-helix results here.
❗ Key Conclusions — Write These in Your Answer
Functional posterior cross-bites are mandibular shift-related, causing midline deviation, condylar asymmetry, and arch constriction — early correction is essential
Quad-helix produces significant transverse increases in all subjects (p < 0.001 for intermolar)
No significant difference between deciduous and mixed dentition groups in expansion magnitude, rate, or relapse
Midpalatal suture opens in both dentitions — confirming orthopedic, not just orthodontic, mechanism
~2 mm overexpansion effectively compensates for expected relapse
Mandibular arch dimensions showed no significant change — no predictable expansion effect on the lower arch
Appliance had excellent patient tolerance — no pain, speech difficulty, or significant soft tissue issues