Picture this exam scenario: A 7-year-old child sits in your chair. Her mom says “her jaw looks crooked.” You notice her teeth bite on the right side but her chin shifts left. Is this dental? Skeletal? Functional? Do you treat now or wait?
Every answer in this review solves THAT case.
⚡ The “Know This Or Fail” Numbers
| Stat | Value | Why It Matters |
|---|---|---|
| Posterior crossbite prevalence | 7–23% | Most common transverse malocclusion |
| FXB = unilateral with shift | 80–97% of all PXB | Nearly all UPXBs are functional! |
| Self-correction rate | 0–9% | Never justify waiting |
| Deciduous dentition prevalence | 8.4% → 7.2% mixed | Slight spontaneous decrease |
| Spontaneous new crossbite development | 7% | Equals self-correction rate — net zero |
| Equilibration success (< 5 yrs) | 27–64% | Only in very young, limited use |
| Arch perimeter gain | 4 mm (85% stable long-term) | Bonus benefit of expansion |
🔥 EXAM TRAP: “Posterior crossbite is self-correcting” → FALSE. Only 0–9%. Never a valid clinical justification.
🧩 Etiology: The BIG Picture First
Think in 3 layers — Genetic → Environmental → Habit
NARROWED MAXILLA
↑
┌─────────────────────────────────┐
│ SKELETAL: Small Max/Mand ratio │ ← Genetic + mouth breathing
│ + Increased lower face height │
└─────────────────────────────────┘
↑
┌───────────────────────────────────────┐
│ AIRWAY: Adenoids / Tonsils / Rhinitis│ → Mouth breathing → narrow maxilla
│ + Neonatal intubation │ → Direct palatal deformation
└───────────────────────────────────────┘
↑
┌─────────────────────────────────────────────┐
│ HABIT: Pacifier / Digit sucking >4 yrs age │ → ↓ Max intercanine + ↑ Mand intercanine
└─────────────────────────────────────────────┘
🧠 Mnemonic: “GANH” (say it like “Gain” — because early treatment = gain!)
Genetics (small maxilla, wide mandible)
Airway obstruction (adenoids, tonsils, rhinitis)
Neonatal intubation
Habits (pacifier/digit sucking beyond age 4)
🔍 Differential Diagnosis — The Most Examined Section
The 3-Type Framework
| Feature | ✅ FXB (Functional) | Single Tooth XB | True Skeletal Bilateral XB |
|---|---|---|---|
| CO vs CR | Discrepancy (mandatory finding) | Coincident | Coincident |
| Mandibular midline | Deviated to crossbite side | Midline OK | Midline OK |
| Maxillary arch shape | Symmetrical (key!) | Asymmetrical | Symmetrical |
| Crowding pattern | More in maxilla (not mandible) | Localized | —- |
| Crossbite side molar | Class II (partial/full) | Varies | Bilateral Class II |
| Non-crossbite side molar | Class I | Normal | Bilateral Class II |
| Condyle position (tomogram) | Non-XB side: down & forward in fossa | Symmetric | Symmetric |
| Cause | Transverse maxillary deficiency | Overretained teeth / arch length | Severe skeletal discrepancy |
🧠 Mnemonic: “SMACK-D” (What FXB gives you clinically)
Shift of mandible → toward crossbite side
Midline mandibular deviation → toward crossbite side
Arch — maxillary is symmetrical (despite appearing unilateral!)
CO–CR discrepancy — the defining diagnostic feature
Klass II on crossbite side / Class I on non-crossbite side (K for klass 😄)
Deficiency maxillary arch → more crowding in upper than lower
🔥 EXAM TRAP: The maxillary arch in FXB is SYMMETRICAL. The unilateral appearance is caused by the mandibular shift — not by asymmetric maxillary constriction. Examiners love asking this!
⏰ Treatment Timing — The Golden Window
Think of the Midpalatal Suture as a WINDOW that closes with age:
Age: 2–5 yrs 6–8 yrs 9–11 yrs 12+ yrs Adult
Suture: Wide open [BEST WINDOW] Narrowing Almost fused Fused
Force: Minimal Small forces Moderate RME needed SURGERY
Recommend: Equilibration ✅ IDEAL ⚠️ Difficult ⚠️ RME only ❌ Ortho+Surg
- Late deciduous / early mixed dentition = IDEAL → small forces open suture, permanent incisors get space before eruption
- Late mixed dentition = DIFFICULT — exfoliating teeth compromise appliance anchorage
- Early permanent dentition (≥12 yrs) = RME preferred — faster rate, greater skeletal expansion, less dental tipping
🔥 EXAM TRAP: Sutural expansion > dental tipping expansion. Always aim for maximal sutural opening + minimal dental tipping. Suturally expanded cases relapse less.
🔧 Appliance Masterclass
Fixed vs. Removable — The War is Already Won
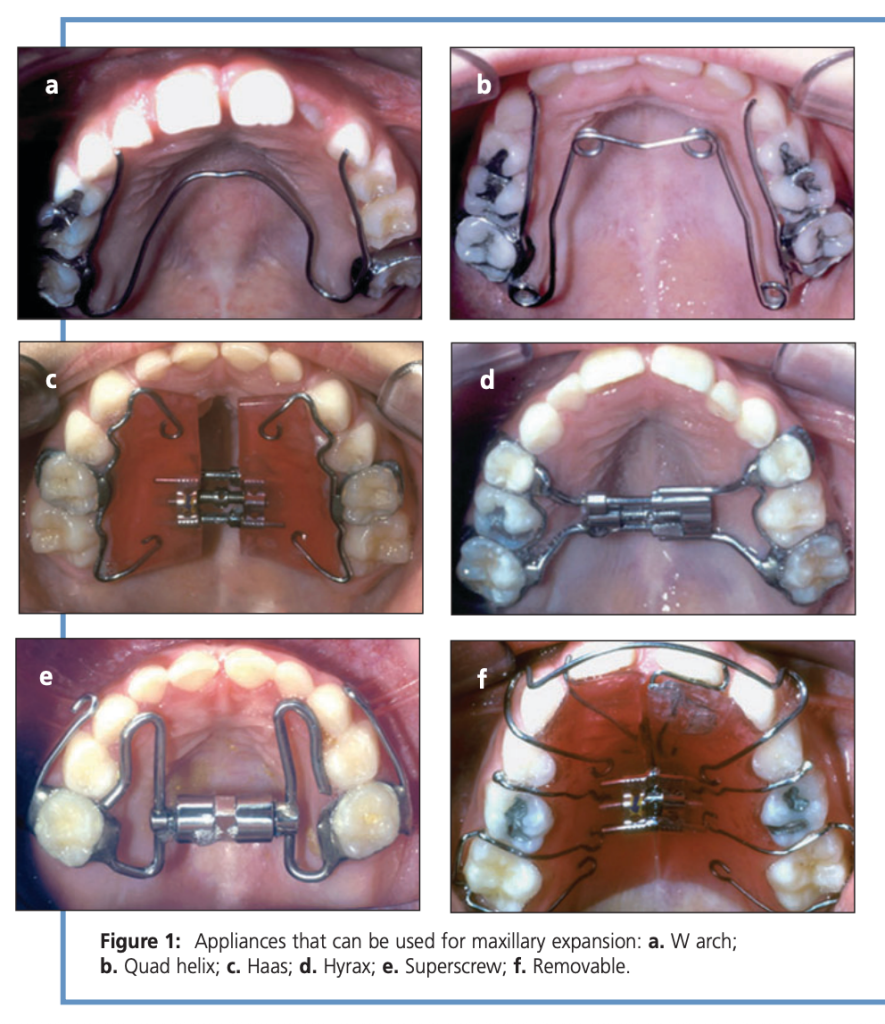
| Appliance | Speed | Rate | Time | Winner Status |
|---|---|---|---|---|
| Quad Helix | Slow | ¼ turn / 2–3 days | 6–12 wks | 🏆 Gold standard — 1/3 cost of removable, 1/5 treatment time |
| W-Arch | Slow | ¼ turn / 2–3 days | 6–12 wks | ✅ Good alternative |
| Haas | RME | 1–2 × ¼ turn/day | 2–6 wks | ✅ Tissue-borne, most skeletal effect |
| Hyrax | RME | 1–2 × ¼ turn/day | 2–6 wks | ✅ Tooth-borne, hygienic |
| Superscrew | RME | 1–2 × ¼ turn/day | 2–6 wks | ✅ Comparable to Haas/Hyrax |
| Removable plate | Slow | ¼ turn / 5–7 days | Longest | ❌ NOT recommended — compliance failure, relapse, lost appliances |
📋 Retention Protocol — “SOLAR”
Stabilize screw with ligature wire or composite
Overexpand — lingual cusps of upper contact buccal cusps of lower
Leave appliance in place for retention OR make removable retainer
At least 4–6 months retention minimum
Rule: Retention period ≥ active treatment duration
⚠️ Side Effects of RME — “DEMO”
Diastema (midline maxillary — transient! closes via transeptal fibers) → warn patient/parent
Expansion of mandibular intercanine width (spontaneous — actually a bonus in crowded cases)
Maxillary protraction (forward movement of maxilla — useful in Class III patients!)
Open bite (anterior) — especially if 2nd permanent molars present; control molar eruption carefully
🧬 The Adaptation Argument (Why You MUST Treat Early)
This is the biological rationale section — examiners love conceptual questions here.
If left untreated, 3 irreversible adaptations occur:
- Condylar asymmetry → glenoid fossa and condyle remodel asymmetrically during growth
- Mandibular rotation → mandible rotates relative to cranial base (submentovertex X-ray shows this in adults)
- Muscle adaptation → masticatory cycle becomes asymmetric (Throckmorton et al.)
After early treatment: condyle symmetry restored, mandibular rotation corrected, masticatory symmetry re-established
Adult with untreated FXB: mandible is rotated relative to cranial base but symmetric within the fossa — adaptation has already “locked in” the asymmetry
🔥 EXAM TRAP: In adults with untreated posterior crossbite, condyles ARE symmetric within the fossa (adaptation is complete) but mandible IS asymmetric relative to the cranial base. Don’t confuse this!
🧠 The TMD Controversy — Balanced Answer Template
For essay/viva: State both sides:
- FOR correlation: Crossbite → condylar asymmetry → joint loading → TMD signs (Alamoudi; Egermark-Eriksson studies)
- AGAINST causation: Sari et al., Keeling et al. found no causal link
- Safe conclusion: “Crossbite may be a cofactor in TMD identification, but its role should not be overstated”
🎯 The Selective Grinding Rule (< 5 Years Only)
- Age limit: strictly < 5 years
- Success rate: 27–64% (Lindner: 50% in 4-year-olds)
- The magic number: maxillary intercanine width must be ≥ 3.3 mm greater than mandibular for best results
- Beyond age 5 → expansion appliances required, not grinding
🏁 Master Flash Summary — “FEED-SOLAR”
(Treatment protocol in one phrase)
Functional shift eliminated by symmetric maxillary expansion
Early treatment — late deciduous / early mixed dentition
Expand symmetrically (even for unilateral presentation!)
Don’t use removable appliances
—
Stabilize screw, Overexpand, Leave appliance in, At least 4–6 months, Retention ≥ treatment time
🔥 5 Rapid-Fire Viva Questions
Q1. Why do we expand the maxilla symmetrically for a unilateral crossbite?
→ Because the maxilla is bilaterally constricted; the unilateral appearance is due to the mandibular shift
Q2. What is the single most important diagnostic feature of FXB?
→ CO–CR discrepancy (centric occlusion ≠ centric relation)
Q3. Why is the Quad Helix preferred over removable plates?
→ 1/3 cost, 1/5 treatment time, no compliance issues
Q4. What happens to the midpalatal diastema created during RME?
→ Closes spontaneously via transeptal fiber pull and dental tipping
Q5. Name two studies supporting crossbite–TMD correlation.
→ Alamoudi (2000) and Egermark-Eriksson et al. (1990)

