Understanding the growth patterns of the maxillary and mandibular lips is essential for effective orthodontic treatment planning. As orthodontic students, recognizing the interplay between facial soft tissues and the underlying hard tissues, particularly during the critical growth period from 8 to 18 years, can significantly influence treatment outcomes. This blog post delves into a lip growth and its implications for orthodontic therapy, providing data-driven insights and clinical guidelines.
Key Findings on Lip Growth
1. Maxillary Lip Length
Maxillary Lip Length Growth (mm)
Age 8
Age 18
Percentage Increase
Largest growth occurred between
Males
17.73
21.53
21.43%
Ages 10 and 16.
Females
17.73
19.88
12.11%
Ages 10 and 14.
2. Maxillary Lip Thickness
Maxillary Lip Thickness Growth (mm)
Age 8
Age 18
Percentage Increase
Males
10.77
15.76
46.33%
Growth was continuous, with the largest increase between ages 12 and 16.
Females
10.90
12.50
14.68%
Growth occurred primarily between ages 10 and 14.
3. Mandibular Lip Length
Mandibular Lip Length Growth (mm)
Age 8
Age 18
Percentage Increase
Males
19.14
26.53
38.56%
Largest increase occurred between ages 12 and 16.
Females
19.14
22.73
18.65%
Growth occurred primarily between ages 10 and 16.
4. Mandibular Lip Thickness
Males: Increased steadily from ages 8 to 16, with a plateau between ages 16 and 18.
Largest increases occurred between ages 14 and 16.
Females: Growth was less pronounced, with significant increases only between ages 10 and 14.
Clinical Implications for Orthodontic Treatment
1. Sexual Dimorphism in Lip Growth
Males experience greater increases in both lip length and thickness compared to females.
Females show more limited growth, particularly in lip thickness during puberty.
2. Extraction Therapy Considerations
Female Patients: Limited lip thickening during puberty makes the effects of extraction therapy more noticeable, especially in patients with straight or concave profiles. Treatment plans should be approached with caution to avoid adverse effects on facial esthetics.
Male Patients: Greater lip thickening provides more flexibility for extractions without significantly impacting facial profile fullness.
Maxillary Lip Thickness Growth Rates
Males:
0.5 mm/year (ages 8–12).
0.7 mm/year (ages 12–16).
Females:
0.5 mm/year (ages 10–12).
0.3 mm/year (ages 12–14).
Conclusion
Understanding the growth patterns of maxillary and mandibular lips is essential for predicting soft-tissue responses and planning effective orthodontic treatments. Sexual dimorphism plays a significant role, with males experiencing greater growth in both lip length and thickness compared to females. These differences must be factored into treatment decisions, particularly for extraction therapy, to ensure optimal esthetic and functional outcomes. As orthodontic students, incorporating these insights into clinical practice will enhance your ability to deliver patient-centered care.
Orthodontic care primarily focuses on dental esthetics and masticatory function, but its impact on sound production is often overlooked. Sound production involves a dynamic interaction with the oral cavity, requiring orthodontists to recognize how dental anomalies and treatments influence speech. Enhanced patient care can be achieved through better treatment planning and referrals to speech pathologists for patients whose malocclusions affect speech production. This is particularly relevant for adults requiring proper speech for professional purposes.
Definition of Sound and Speech Mechanism
Sound is mechanical vibration energy requiring the coordination of neural, muscular, mechanical, aerodynamic, acoustic, and visual elements. Speech production involves four processes:
Language processing in the brain.
Motor command generation to vocal organs.
Articulatory movements of the oral cavity.
Air emission from the lungs.
Speech sounds are classified into:
Vowels: Produced without obstruction to airflow.
Consonants: Produced with varying obstructions in oral or nasal cavities.
Classification
Ingram’s Classification:
Dysphonia: Disorders of vocalization.
Dysrhythmia: Respiratory coordination issues.
Dysarthria:
Due to neurological abnormalities (e.g., motor neuron lesions).
Due to local abnormalities (e.g., jaws, teeth, palate).
Non-Structural Disorders: Mental, hearing, or environmental factors.
Developmental Disorders: Abnormal or delayed speech development.
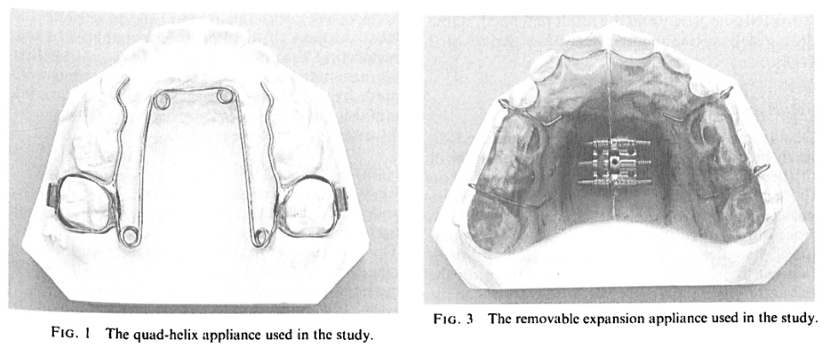
Palatal expansion has been a cornerstone of orthodontic treatment for over a century. Despite its proven efficacy, this technique has sparked debates within the orthodontic community. Is rapid expansion the best approach, or do slower methods offer greater stability? Let’s dive into the history, mechanics, and clinical applications of maxillary expansion, with a special focus on the quad-helix appliance.
The primary goal of palatal expansion is to coordinate the maxillary and mandibular denture bases, addressing narrow or collapsed arches. This can be achieved through:
Orthodontic Movement (tooth-focused)
Orthopedic Movement (bone-focused)
Combination Therapy
A variety of appliances—fixed, semi-fixed, and removable—are employed to achieve these goals.
Method
Advantages
Challenges
Rapid Palatal Expansion
Quick skeletal changes
Potential for relapse and sutural strain
Slow Expansion
Greater histologic integrity of sutures
Requires longer treatment time
HISTORY
Coffin Loop Appliance:
Incorporated in a vulcanite plate for upper arch expansion.
Produces continuous force due to the configuration of the palatal compound loop.
Martin Schwarz Appliance:
Popular in Europe.
Utilizes tissue-borne anchorage with wire components for tooth movement.
Expansion force is intermittent due to the jackscrew mechanism.
Haas and Wertz Fixed Appliance:
Designed for rapid expansion of the midpalatal suture in narrow maxillary arches.
Cemented to maxillary first premolars and first permanent molars.
Includes a palatal jackscrew and acrylic extensions.
Produces lateral orthopedic movement of the maxilla due to high force magnitude.
Load-Activation Characteristics:
Chaconas and Caputo found differences in stress transmission through craniofacial bones with various fixed expansion appliances.
Impact on craniofacial sutures varies depending on the appliance.
Rickett’s “W” Expansion Appliance:
Initially used for cleft palate conditions with collapsed dental arches.
Acts continuously over time until activation force dissipates.
What Makes the Quad-Helix Appliance Unique?
Helical Loops for Increased Flexibility:
Initially added to the posterior segment of the palatal arch
Further modification introduced four loops (two anterior and two posterior), creating the quad-helix appliance.
Construction Details:
Made of 0.038-inch (0.975 mm) wire.
Soldered to bands cemented to maxillary first permanent molars or deciduous second molars, depending on the patient’s age.
Initial Activation and Effects:
Appliance is activated before cementation.
Results in expansion of buccal segments and rotation of banded teeth
Force Magnitude:
Chaconas and Caputo reported that 8 mm of expansion before cementation generates approximately 14 ounces of force
Effectiveness in Different Age Groups:
Effective in orthopedically widening the maxilla in children, helping to establish a normal maxillomandibular relationship.
Force is sufficient for tooth movement but insufficient for orthopedic effects in adults with closed midpalatal sutures.
In children, particularly in the deciduous or early mixed dentition stages, the resistance of the patent suture is lower than the dentoalveolar area.
Clinical Case: A Pediatric Success Story
Patient History: Prolonged thumb-sucking led to a narrow maxilla due to lowered tongue position and buccinator muscle forces.
Treatment: Quad-helix appliance activated ~8 mm, sufficient for maxillary expansion.
Outcome: Successful expansion and resolution of thumb-sucking habit. The appliance’s palatal position ensured comfort and minimal impact on speech.
Maxillary Molar Width: Increased by an average of 5.88 mm, reflecting significant dental expansion.
Average Frontal Molar Relation: Improved by 2.95 mm, indicating better occlusal alignment.
Maxillary Intercanine Width: Expanded by 2.74 mm, enhancing anterior dental arch form.
Orthopedic Changes (T₁ to Tₚ)
Maxillary Width: Increased by 0.92 mm, with five cases showing expansions exceeding 2.7 mm.
Maxillomandibular Width: Increased by 0.89 mm, with notable cases surpassing 1.4 mm.
Palatal Changes: The anterior palate moved downward, increasing maxillary height.
Relapse and Stability (Tₚ to T₂)
Minimal Relapse: Dental expansions remained stable over 42 months.
Orthopedic Effects: Demonstrated high stability, contrasting with the relapse often seen in rapid palatal expansion.
Palatal Plane and Maxillary Height: Slight decreases observed, indicating no net parallel downward movement.
Slow vs. Rapid Expansion
Slow expansion using the quad-helix appliance demonstrated superior stability and less relapse compared to rapid palatal expansion. The gradual physiologic movement allowed the facial skeleton to adapt, ensuring long-term stability.
Bite Opening
Active Expansion (T₁ to Tₚ): Slight bite opening occurred due to occlusal interferences.
Post-Expansion (Tₚ to T₂): Additional bite opening was attributed to orthodontic treatment rather than the expansion appliance.
Facial Skeletal Considerations
Stability was influenced by initial nasal and maxillary widths:
Narrow Maxilla + Normal/Wide Nasal Width: High stability.
Narrow Nasal Width + Normal Maxilla: Lower stability.
Facial Type
The sample skewed toward brachyfacial types, limiting conclusions about expansion outcomes across facial types.
Promote beneficial dentoskeletal changes during growth periods (Bell, 1982).
Posterior cross-bites develop early and are not self-correcting (Moyers & Jay, 1959; Thilander et al., 1984).
Orthodontic Response to Expansion
Initial response completed within a week (Storey, 1973; Cotton, 1978; Hicks, 1978).
Subsequent movements occur as compressed buccal alveolar plate resorbs at the root-periodontal interface due to continued force (Storey, 1973).
Orthopaedic Effects of Expansion
Sufficient transverse forces can overcome bioelastic strength of sutural elements, causing:
Orthopaedic separation of maxillary segments (Storey, 1973; Chaconas & de Alba y Levy, 1977; Cotton, 1978; Hicks, 1978).
Palatal segment repositioning continues until force is reduced below sutural tensile strength.
Stabilization involves reorganization and remodeling of sutural connective and osseous tissues (Storey, 1973; Ekstrom et al., 1977).
Increased Maxillary Arch Width
Linked to orthodontic and/or orthopaedic effects of expansion (Ficarelli, 1978; Moyers, 1984).
Initial changes involve lateral tipping of posterior maxillary teeth due to compression and stretching of periodontal and palatal soft tissues.
Midpalatal Sutural Opening and Maxillary Displacement
Expansion leads to:
Downward and forward displacement of the maxilla with bite opening (Haas, 1961).
Downward and backward rotation of the mandible, increasing the vertical dimension of the lower face (Haas, 1970).
Subsequent recovery of mandibular posture noted in most cases (Wertz, 1970).
Rate of Expansion and Dental Arch Width Increase
Rapid Maxillary Expansion (Krebs, 1959, 1964):
Subjects aged 8–19 years showed an average dental arch increase of 6.0 mm (range: 0.5–10.3 mm).
Skeletal changes accounted for:
~50% of the arch width increase in 8–12-year-olds.
~33% of the increase in 13–19-year-olds.
Slow Maxillary Expansion (Hicks, 1978):
Subjects aged 10–15 years showed a dental arch width increase of 3.8–8.7 mm.
Skeletal response ranged from 16–30%, with lower skeletal response in older patients.
Buccal tipping of molars and skeletal segments contributed to arch width increase.
Asymmetrical angular changes between left and right molars and maxillary segments were observed.
Removable Plates and Sutural Growth (Skieller, 1964):
In subjects aged 6–14 years:
20% of dental arch widening was attributed to sutural growth.
Sutural growth rate during expansion was significantly greater than during follow-up, indicating stimulated growth during expansion.
Removable Plates and Sutural Growth (Skieller, 1964):
Study on 20 subjects aged 6–14 years:
20% of dental arch widening was attributed to sutural growth.
Growth rate at the mid-palatal suture was significantly higher during expansion compared to the follow-up period.
Suggests that sutural growth is stimulated during the expansion period.
Histologic Findings in Slow Expansion Procedures:
Sutural separation occurs at a controlled rate, maintaining tissue integrity during maxillary repositioning and remodeling (Storey, 1973; Ekstrom et al., 1977; Cotton, 1978).
Relapse Tendency During Post-Retention Period:
Relapse potential is reduced in slow expansion procedures due to:
Types of Anchorage Based on Maximum Anchorage Demand
Anchorage is classified into three types based on the maximum anchorage required:
Type A: Maximum Anchorage
Definition: Anchorage demand is very high.
Space Utilization: Not more than 1/4th of the extraction space should be closed by forward movement of anchor teeth.
Mechanism: The extraction space is primarily closed by maximum incisor retraction.
Type B: Moderate Anchorage
Definition: Anchorage demand is moderate.
Space Utilization: Anchor teeth are allowed to move forward by up to half the extraction space.
Mechanism: The extraction space is closed by a combination of incisor retraction and posterior tooth protraction.
Type C: Minimum Anchorage
Definition: Anchorage demand is very low.
Space Utilization: More than half of the extraction space is closed by mesial movement of the anchor teeth.
Mechanism: The extraction space is primarily closed by protraction of posterior teeth with minimal incisor retraction.
Group B Anchorage: Biomechanics of Space Closure
Key Features
Archwire: A working archwire with a minimal curve of Spee (e.g., 0.019 × 0.025-inch SS wire) is engaged into the bracket slots and molar tubes.
Couples and Forces:
The wire generates a couple at the level of the bracket/molar tube at both ends, leading to the generation of a moment of couple (M_c).
Tiebacks create a force for space closure (F), generating a moment of force (M_F).
Force and Moment Interaction:
At either end of the system, the moments of couple and force are created in opposite directions, canceling each other.
This leaves only the translatory force (F) to exist, enabling space closure.
Translational Movement
When moments are balanced correctly:
No vertical component of force is produced.
No rotational tendency occurs in the system.
Occlusal plane and overbite remain unchanged.
Diagram: Depicts the working archwire (faded blue line) and the resulting forces and moments.
Outcome: Translation of anterior and posterior segments without altering the occlusal plane or overbite.
Planned Imbalance of Moments
In some scenarios, moments are deliberately imbalanced to achieve specific vertical movements:
Posterior Teeth: Extrusion (yellow arrows).
Anterior Teeth: Intrusion (yellow arrows).
Effect: Opens the deep overbite by modifying the vertical dimension.
Diagram: Illustrates the planned imbalance (thick red curved arrow) leading to controlled vertical movements.
Outcome: Deep overbite correction through extrusion of posterior teeth and intrusion of anterior teeth.
Summary
Group B anchorage allows for controlled space closure through balanced forces and moments. By adjusting the moments, orthodontists can achieve either translational movement or vertical adjustments, making it a versatile approach in clinical orthodontics.
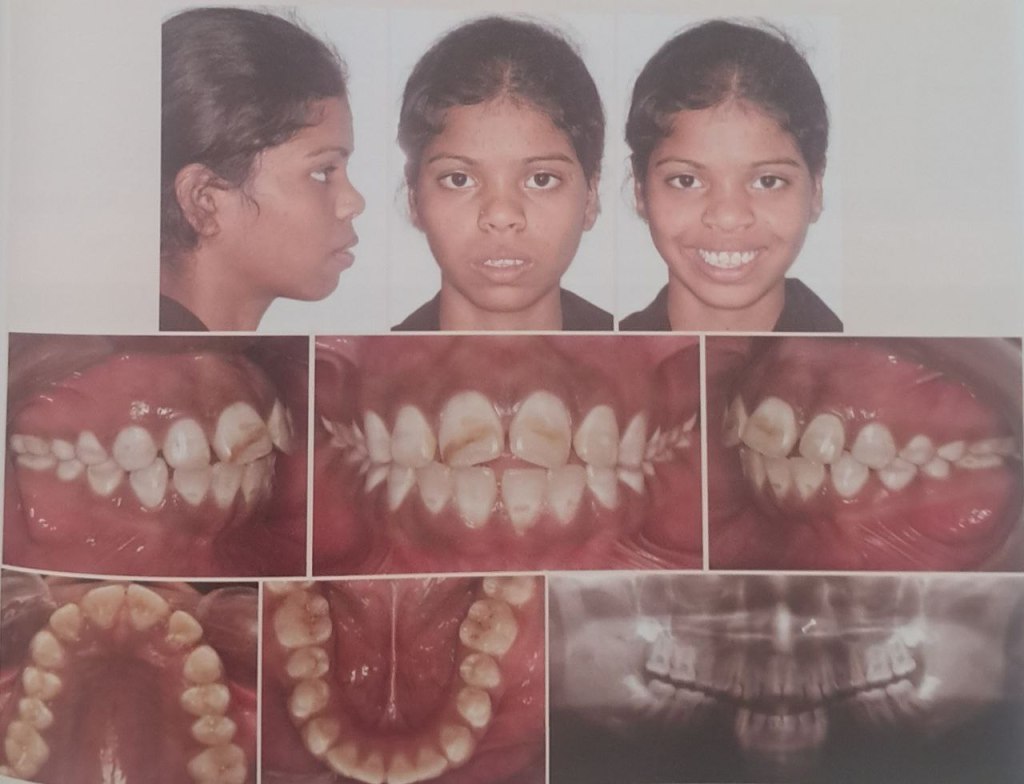
Bimaxillary protrusion is a condition characterized by protrusive and proclined upper and lower incisors with increased lip procumbency. It is commonly seen in African-American and Asian populations but can occur across all ethnic groups. Due to the negative perception of protrusive dentition and lips in many cultures, patients with bimaxillary protrusion often seek orthodontic treatment to improve their facial profiles. This guide summarizes key aspects of bimaxillary protrusion, including its etiology, pretreatment characteristics, treatment goals, and outcomes.
Etiology of Bimaxillary Protrusion
The etiology of bimaxillary protrusion is multifactorial, including:
Genetic Factors: Hereditary traits influencing facial and dental structures.
Environmental Factors:
Mouth breathing.
Tongue and lip habits.
Increased tongue volume.
Morphological Features
Keating’s study on Caucasian patients identified the following cephalometric traits:
Feature
Observation
Posterior cranial base
Shorter
Maxilla
Longer and more prognathic
Skeletal pattern
Mild Class II
Upper and posterior face height
Smaller
Facial planes
Divergent
Soft tissue profile
Procumbent with a low lip line
Pretreatment Characteristics
Cephalometric Traits
Patients with bimaxillary protrusion exhibit the following pretreatment characteristics:
Trait
Observation
Upper and lower incisor proclination
Increased (2-3 SD above mixed racial norms)
Vertical growth patterns
Increased lower anterior face height
Mandibular plane angle
Elevated
Alveolar heights
Increased
Soft Tissue Features
Lip Position:
Upper and lower lips are ahead of the E-plane.
Lower lip: 6.0 mm ahead (Keating’s Caucasian sample).
Upper lip: 1.0 mm ahead (less than Keating’s 3.4 mm).
Nasolabial Angle:
Found to be 94° (1 SD more acute than mixed racial norms).
Tan’s study on Chinese patients reported an even more acute angle (86.6°).
Lip Thickness:
Increased, likely due to a higher proportion of African-American patients in the study.
Alveolar Morphology
Alveolar Width: Reduced compared to Handelman’s norms.
Alveolar Height: Increased, consistent with vertical facial growth patterns.
Thin and elongated alveolus may limit retraction mechanics and necessitate surgical osteotomies in severe cases.
Orthodontic Treatment Goals
The primary objectives of treating bimaxillary protrusion include:
Dental Goals:
Retraction and retroclination of maxillary and mandibular incisors.
Reduction in incisor proclination and protrusion.
Soft Tissue Goals:
Decrease in lip procumbency and convexity.
Improvement in the nasolabial angle.
Mechanics Used:
Extraction of four first premolars.
Retraction using maximum anchorage mechanics.
Flowchart: Treatment Goals and Process
1. Initial Diagnosis → 2. Extraction of Four Premolars → 3. Retraction of Incisors → 4. Profile Improvement
Treatment Outcomes
Dental and Skeletal Changes
Parameter
Observation
Interincisal angle
Increased significantly
Incisor inclination
Decreased significantly
Anteroposterior incisor position
Reduced significantly (P < .001)
Soft Tissue Changes
Upper Lip Retraction:
Ratio of upper incisor retraction to upper lip retraction: 2.2:1 (similar to Chiasson and Hershey).
Lip response depends on factors like interlabial gap, lip redundancy, and musculature quality.
Vertical Dimension
No significant changes in lower anterior face height or mandibular plane angle, indicating that treatment mechanics do not affect the vertical dimension.
Introduction Malocclusion, characterized by changes in teeth positioning and skeletal growth, represents a global public health concern.
Historical Context: Correction attempts date back to at least 1000 BC.
Prevalence: Class II malocclusion affects one-third of the population and is categorized as skeletal or dental in origin.
Etiology:
Only 20% of Class II Division 1 cases are due to maxillary protrusion.
The majority stem from mandibular retrusion.
This prevalence has led to the development of functional appliances aimed at stimulating mandibular growth. These devices are divided into removable and fixed functional appliances.
Fixed Functional Appliances
Types:
Rigid: Herbst appliance, MARA (Mandibular Advancement Repositioning Appliance).
Flexible: Jasper Jumper, Scandee tubular jumpers.
Hybrid: Forsus Fatigue Resistant Device (FFRD).
Forsus Fatigue Resistant Device (FFRD):
A telescoping spring mechanism for Class II correction.
Provides moderate patient tolerance with initial discomfort that subsides over time.
PowerScope Appliance:
Latest addition, introduced by Dr. Andy Hayes in 2016 in collaboration with American Orthodontics.
Features a telescopic mechanism with a nickel-titanium (NiTi) spring delivering 260 g constant force.
Designed as a preassembled, one-size-fits-all appliance for easy chairside application.
Study Rationale While Forsus FRD is extensively studied, limited literature evaluates and compares the skeletal, dental, and soft tissue effects of PowerScope. This study bridges that gap by conducting a cephalometric evaluation and comparison of these two fixed functional appliances.
Both appliances are effective in correcting Class II discrepancies caused by retrognathic mandibles. However:
Forsus FRD is superior in achieving skeletal changes, particularly maxillary retrusion and mandibular advancement.
PowerScope shows more pronounced effects on dentoalveolar and soft tissue parameters, especially upper incisor inclination correction and facial convexity improvement.
In the world of orthodontics, Class II intermaxillary elastics have stood the test of time as a cornerstone of clinical treatment. Since their introduction by Maynard in 1843 and subsequent refinement by Henry A. Baker in the late 19th century, these small but mighty elastics have been indispensable in managing malocclusions. For orthodontic students, understanding their effects, particularly on the functional occlusal plane (FOP), is essential for mastering treatment planning and clinical decision-making.
Why Does the Functional Occlusal Plane Matter?
The occlusal plane is more than a line connecting occlusal surfaces; it’s a fundamental aspect of facial esthetics, function, and skeletal harmony. Its orientation relative to cranial and mandibular planes influences:
Maxillary and mandibular skeletal relationships
Facial forms and esthetics
Occlusal function
Alterations in the occlusal plane, whether due to growth or treatment, can significantly affect treatment outcomes and post-treatment stability. As orthodontic practitioners, it’s crucial to strike a balance between functional correction and maintaining or improving esthetic harmony.
The Role of Class II Elastics
Class II elastics have long been used to address sagittal and vertical discrepancies, including the correction of Class II malocclusions and open bites. While effective, their reciprocal forces can induce both desirable and adverse effects. Reports have suggested that Class II elastics might steepen the occlusal plane, potentially leading to instability or relapse post-treatment. However, these findings were often based on small sample sizes or non-growing patients, leaving gaps in our understanding of their effects during growth phases.
To address these gaps, a recent study analyzed the effects of Class II elastics on FOP in growing patients aged 11 to 16 years. Here’s what the researchers aimed to find out:
Does the use of Class II elastics steepen the FOP?
Are these changes more pronounced in extraction cases or patients with high-angle skeletal patterns?
Do these changes persist or relapse after treatment?
Key Findings to Remember
1. Angular Changes in the FOP
FOP-SN and FOP-FH: Decreased significantly from pretreatment (T0) to post-treatment (T1) and continued to decrease 1 year post-treatment (T2).
FOP-MP: Increased from T0 to T1, likely as a reciprocal effect of FOP-SN/FH changes.
2. Influence of Skeletal Patterns
Hyperdivergent patients showed the largest FOP angles across all time points, while hypodivergent patients had the smallest.
Despite these differences, changes in FOP were consistent across skeletal types, indicating that Class II elastics affect all growth patterns similarly.
3. Treatment Modalities: Extraction vs. Non-Extraction
Patients undergoing extraction treatment exhibited steeper initial FOP-MP angles, reflecting a preference to extract in such cases.
No significant differences were observed in FOP changes between extraction and non-extraction groups during or after treatment.
Clinical Implications for Students
Normal Growth vs. Treatment Effects: The study suggests that changes in FOP may largely reflect normal growth patterns rather than direct effects of Class II elastics. This aligns with findings from Creekmore, Schudy, and Harris, emphasizing the importance of accounting for growth dynamics.
Individualized Treatment Planning: While Class II elastics are versatile, their effects on the FOP and associated structures vary based on skeletal patterns and growth trends. Orthodontic treatment must be tailored to each patient’s unique craniofacial morphology.
Extraction Considerations: Although extraction cases may present steeper occlusal planes initially, the use of Class II elastics does not appear to exacerbate this steepness.
Takeaways for Orthodontic Students
Class II elastics remain a reliable tool for addressing Class II malocclusions, but understanding their nuanced effects on the FOP is key to optimizing outcomes.
Growth patterns play a pivotal role in how the FOP evolves during treatment. Observing these changes in clinical practice can enhance your ability to predict and manage treatment outcomes.
Finally, always consider the interplay between function, esthetics, and stability when planning orthodontic interventions.
Class II elastics may be small, but their impact on treatment is anything but. With careful planning and an understanding of growth influences, you can wield this classic tool to achieve remarkable results in your future practice.
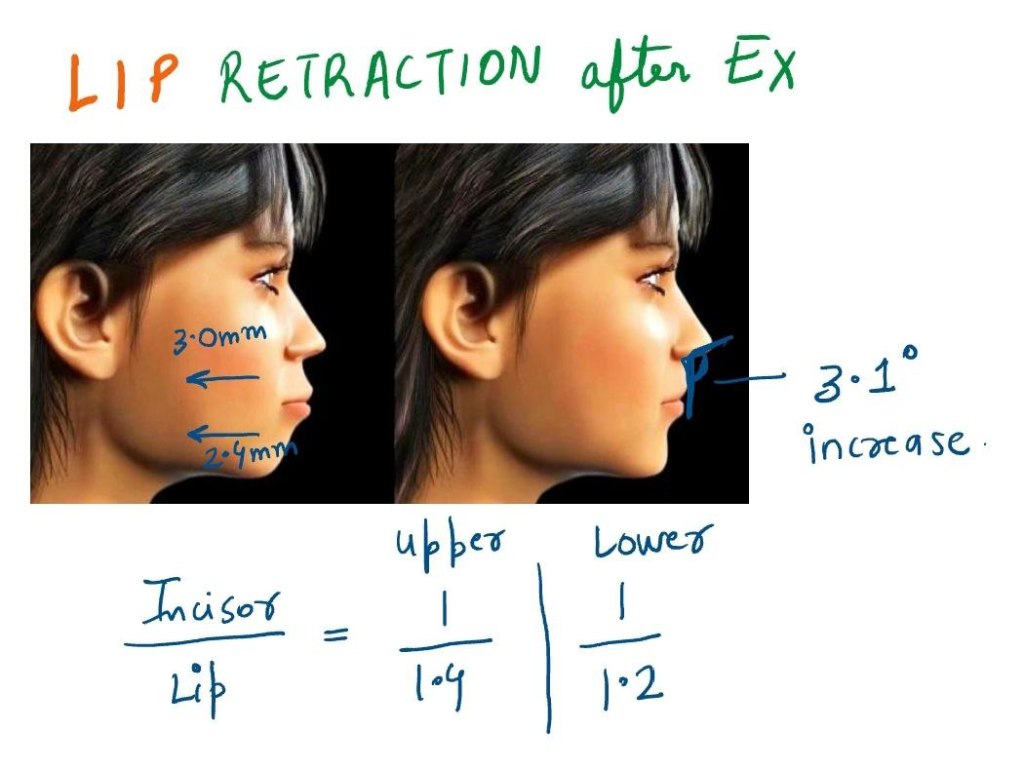
Bimaxillary protrusion is a common orthodontic condition marked by protrusive and proclined upper and lower incisors, coupled with increased lip prominence. While predominantly seen in African American and Asian populations, it is not limited to any single ethnic group. This condition often leads patients to seek orthodontic treatment due to the aesthetic concerns of protruding lips and dentition.
Soft Tissue and Hard Tissue Correlation
Orthodontic studies present two conflicting perspectives on the relationship between incisor retraction and lip position:
Strong Correlation: Some studies demonstrate a direct relationship between incisor and lip retraction.
Weak Correlation: Some studies suggest that soft tissue changes do not proportionally mirror dental movements due to variables like growth, lip tonicity, and anchorage.
Four retrospective studies on bimaxillary protrusion treatment provided valuable insights:
Study Findings
Upper Lip Retraction (mm)
Lower Lip Retraction (mm)
Nasolabial Angle Increase (°)
Caplan et al. (2009)
3.0
2.4
Not significant
Tan et al.
2.7
2.0
10.5
Lew
3.2
4.5
10.0
Bills et al.
3.0
2.4
3.1
Incisor Retraction and Lip Retraction Ratios
Study
Upper Lip to Incisor Retraction
Lower Lip to Incisor Retraction
Caplan et al.
1:1.4
1:1.2
Other Studies
1:2.2
1:1.75
Clinical Implications
Four-premolar extractions effectively reduce lip procumbency in bimaxillary protrusion.
Nasolabial angle tends to increase post-treatment.
Molar distalization is a crucial technique in orthodontics, particularly for patients with Class II malocclusion. Thanks to advancements in biomechanics, materials, and technology, orthodontists now have access to a variety of intramaxillary intraoral appliances that can apply light, continuous forces for effective molar distalization. These appliances have become a game-changer, providing us with more precise control and predictable results.
Types of Intramaxillary Appliances
The application of forces in molar distalization can come from two primary areas: the buccal or the palatal region. Depending on where the force is applied, appliances can be categorized into two broad groups:
Buccal Force Application: These appliances apply force from the outside of the dental arch.
Palatal Force Application: These appliances exert force from the roof of the mouth.
Additionally, the force mechanisms can be divided into two categories:
Friction-Free Mechanism: This type involves appliances like the pendulum, which are designed to move the molars without causing significant friction.
Sliding Mechanism: Appliances like nickel-titanium (NiTi) coil springs use a sliding mechanism to apply force, creating a more dynamic force delivery system.
Each of these appliance types has its own set of advantages and drawbacks, and comparing their efficiency in achieving molar distalization is key to making evidence-based treatment decisions. However, due to the limited number of randomized clinical trials, a meta-analysis is often not possible. That said, a comprehensive analysis of existing studies can still offer valuable insights into how these appliances work.
Treatment Outcomes: Overall Effects
When all intramaxillary appliances were considered together, some general findings emerged:
First Molar Movement: On average, first molars moved 2.9 mm distally, but this came with a 5.4° of distal tipping.
Incisor Movement: The incisors shifted mesially by 1.8 mm with 3.6° of mesial tipping.
Premolar Movement: Premolars showed a mesial shift of 1.7 mm, though tipping was less pronounced.
Vertical movements were generally extrusive for incisors and premolars, with incisors showing an average extrusion of 0.4 mm and premolars 1.1 mm. Interestingly, molar vertical movements were not statistically significant, indicating that the main effect on molars was distal movement and tipping rather than vertical displacement.
Treatment Effects: Buccal vs. Palatal Appliances
Now, let’s delve into the specific effects of buccal and palatal appliances. These results highlight the different ways these appliances move teeth:
Buccal Appliances:
Molar Movement: Molar distal movement was 2.6 mm, with a more significant tipping of 8.3°.
Incisor Movement: Incisors moved mesially by 1.9 mm with 5.0° of mesial tipping.
Premolar Movement: Premolars demonstrated a 2.0 mm mesial shift, accompanied by 7.0° of mesial tipping.
Vertical Movement: Premolars showed a slight extrusion of 0.7 mm, while incisors had a more modest extrusion of 0.2 mm.
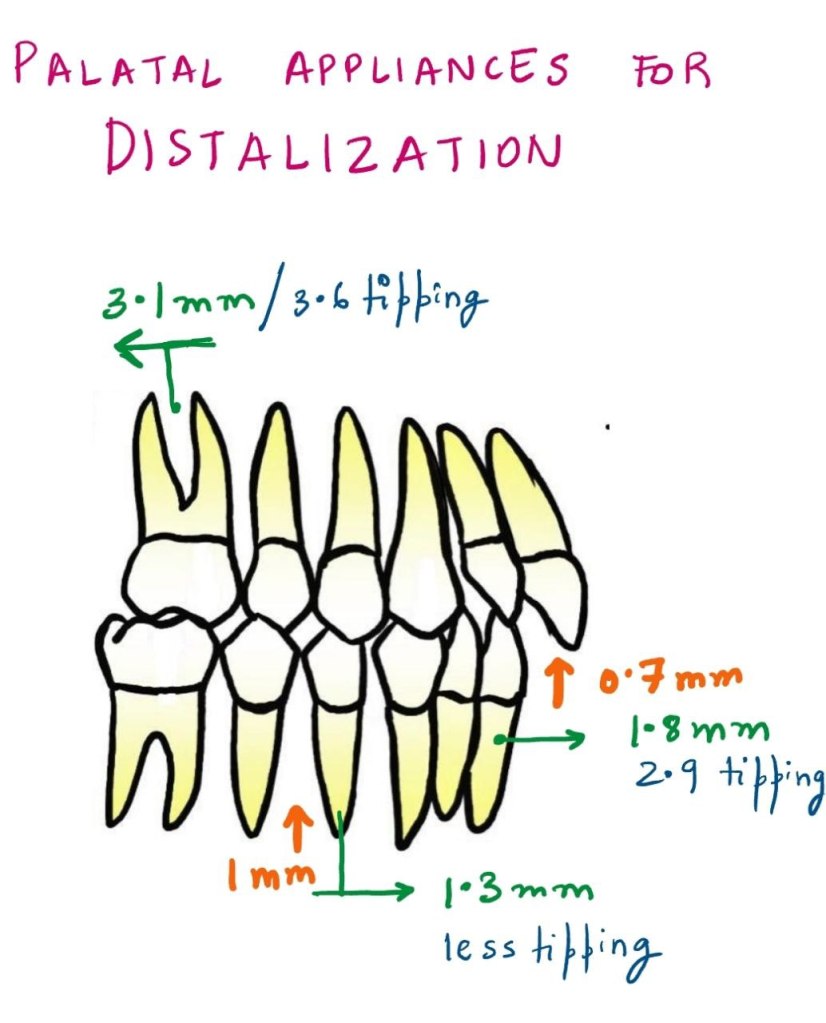
Palatal Appliances:
Molar Movement: Molar distalization was slightly more pronounced, with 3.1 mm of movement and 3.6° of tipping.
Incisor Movement: Incisors exhibited a mesial shift of 1.8 mm with 2.9° of mesial tipping.
Premolar Movement: Premolars moved mesially by 1.3 mm with less tipping than buccal appliances.
Vertical Movement: The extrusion for incisors was 0.7 mm, and premolars showed an extrusion of 1.0 mm.
Molar Distalization and Anchorage Loss
The primary effect of noncompliance intramaxillary appliances is molar distalization, which is typically achieved through a combination of crown distal movement and tipping. While distalization is the goal, a common side effect observed is loss of anchorage. This loss can be seen in the mesial movements and extrusions of incisors and premolars.
Key Findings:
Molars: Show a combination of distal crown movement and distal tipping.
Incisors: Exhibit mesial movement, tipping, and extrusion.
Premolars: Display mesial crown movement and extrusion.
As with any treatment modality, careful planning is required to manage these unintended side effects and achieve the best possible clinical outcomes.
Buccal vs. Palatal Appliances: Tipping and Force Mechanics
One interesting observation in the study was the difference in tipping effects between buccal and palatal acting appliances. Palatal appliances consistently resulted in less tipping of teeth compared to buccal appliances, as indicated by the non-overlapping confidence intervals.
Why the Difference?
The key reason for this difference lies in the moment arm of the force. In palatal appliances, the line of action of the force is closer to the center of resistance of the tooth, leading to less tipping and more controlled molar movement.
Table 1: Comparison of Tipping between Buccal and Palatal Appliances
Appliance Type
Molars Distal Movement (mm)
Molars Tipping (°)
Incisor Mesial Movement (mm)
Incisor Tipping (°)
Premolar Mesial Movement (mm)
Premolar Tipping (°)
Buccal Appliances
2.6
8.3
1.9
5.0
2.0
7.0
Palatal Appliances
3.1
3.6
1.8
2.9
1.3
3.0
This table highlights the greater tipping observed with buccal appliances compared to palatal appliances, as well as the differences in molar distalization and mesial movement of incisors and premolars.
The Nance Button: Anchorage Considerations
Another point of discussion is the use of the Nance button to reinforce anterior anchorage during molar distalization. While it can support anchorage to some extent, it does not provide absolute anchorage. This is because the Nance button, as part of the anchorage unit, cannot completely resist mesial forces during molar distalization. Clinically, this often results in an increased overjet and proclination of maxillary incisors.
Clinical Tip:
For patients already presenting with an increased overjet, orthodontists must proceed with caution when prescribing these appliances. These cases may require additional measures to control the overjet and manage incisor proclination.
The Pendulum Appliance: A Look at Tipping and Movement
The pendulum appliance, a popular friction-free appliance, was noted in the study to cause the greatest distal tipping of molars. However, this tipping was correlated with a larger amount of distal crown movement. Interestingly, this tipping can often be corrected with the use of molar uprighting bends.
Table 2: Molar Distalization and Tipping with the Pendulum Appliance
Movement Type
Molar Distal Movement (mm)
Molar Tipping (°)
Pendulum Appliance
3.4
9.0
This table shows that the pendulum appliance can achieve significant molar distalization but at the cost of increased tipping. These tipping movements can be addressed with molar uprighting bends, which can help reduce the tipping angle.
Factors Affecting Molar Distalization
Several factors can influence the effectiveness of molar distalization, including:
Teeth Used for Anchorage: Different anchorage setups can affect the extent of distal movement.
The Type of Appliance Used: Whether the appliance uses a sliding mechanism or a friction-free mechanism plays a role.
Patient Factors: Age, initial molar relationships, and the eruption of second and third molars all contribute to how effectively molars are distalized.
In studies that focus on growing patients, mean ages ranged from 11.2 to 14.9 years, which is crucial because the growth phase can significantly impact the effectiveness of treatment. For example, molar distalization is often more effective before the second molars have erupted. When second molars are erupted, more force may be required, and the treatment time may increase.
Table 3: Influence of Molar Eruption on Distalization Efficiency