👋 Hey there, fellow ortho warriors! Today, we’re diving into the mysterious world of Class II malocclusion—where the maxilla likes to boss around the mandible, and our job is to restore the balance of power! 🦷⚖️
Why Does Class II Happen? 🤔
Class II malocclusion isn’t just about an overgrown maxilla or a shy mandible. It’s a whole party of skeletal structure, growth patterns, and dentoalveolar development (McNamara, 1981). Think of it as a complex relationship—sometimes it’s the maxilla’s fault, sometimes the mandible’s, and sometimes they just don’t get along. 😅
Treatment to the Rescue! 🦸♂️
To tame this rebellious jaw situation, orthodontists use:
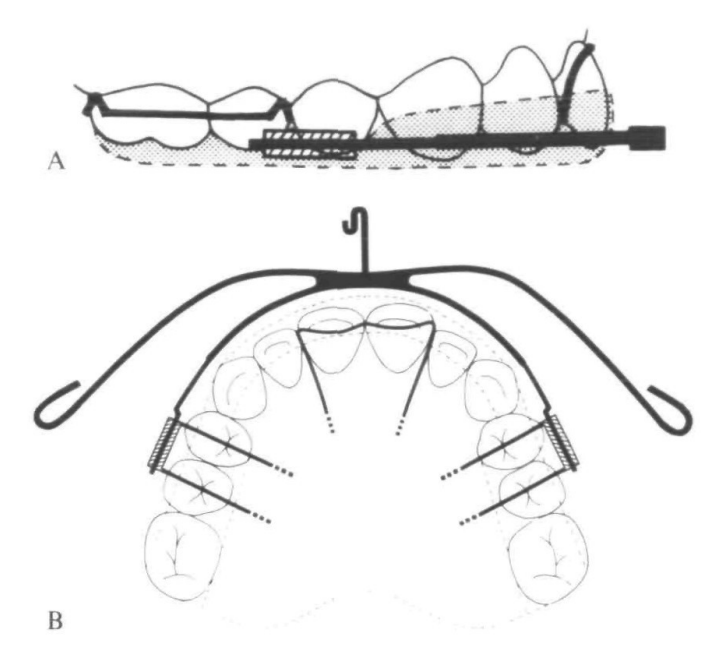
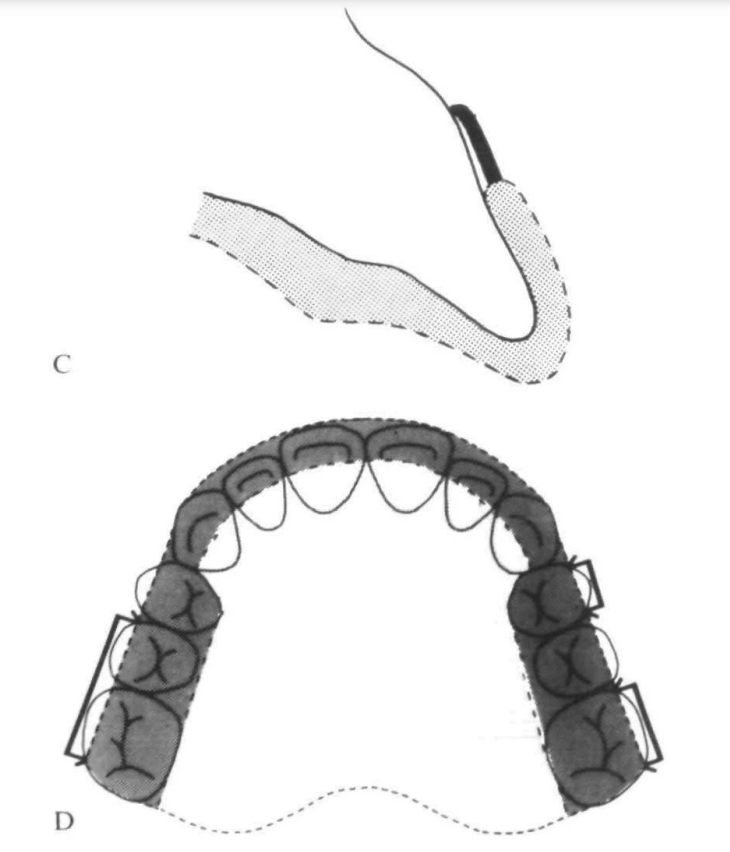
📌 Extraoral force (a.k.a. the famous headgear) to put the maxilla in its place.
📌 Functional appliances (activators, Frankels, etc.) to give the mandible a growth boost.
📌 A combo of both when we want to play it safe—like pairing Batman & Robin for maximum crime-fighting (Meach, 1966; Bass, 1982).
What Happens When We Use High-Pull Headgear + Activator?
This legendary duo doesn’t just sit there looking pretty. It:
✅ Restricts maxillary growth (no more forward expansion party! 🎉)
✅ Stops maxillary teeth from going mesial & vertical (so they stay where they belong)
✅ Encourages better posterior tooth and condylar remodeling (remodeling isn’t just for houses! 🏠)
✅ Improves muscle patterns (stronger jaws = better function 💪)
💡 Remember: High-pull headgear is like a strict teacher holding the maxilla back, while the activator is the personal trainer pushing the mandible forward. 💪🦷
The Soft Tissue Side of the Story! 😍
We focus a lot on bones, but let’s be real—patients care about their face in the mirror! 🤳
Soft tissue changes in Class II treatment can be unpredictable, but here’s the gist:
✔ Lip retrusion happens (Forsberg & Odenrick, 1981)
✔ Soft tissue pogonion moves forward (McDonagh et al., 2001)
✔ The profile can flatten out (Hansson et al., 1997, 2000)
📌 Mnemonic to Remember Soft Tissue Changes: “RPF” – Retrusion, Pogonion Forward, Flattening! 🎯
What Happens to the Maxilla? 🏠⬅️
When we use high-pull headgear + activators, the maxilla doesn’t just sit there—it gets pulled back like a stubborn kid being dragged away from a candy store. 🍬🚫
✅ Point A shifts backward
📍 −1.4 mm (N Perpendicular)
📍 −2.3 mm (OLp)
This means we’re seeing true orthopedic retraction—aka maxillary restraint in action! 🚀
Why does this matter? Because a Class II case with maxillary excess needs more than just dental changes—we need to slow down forward maxillary growth! 🏃♂️💨
Is This a Proven Effect? 📜
Oh, you bet! Studies have been backing this up for decades (Pfeiffer & Grobéty, 1982; Pancherz, 1984; Van Beek, 1984, and many more!).
🧐 Key evidence?
📌 SNA decreased in the treatment group (yay, retraction! 🎉)
📌 SNA increased in the control group (because they didn’t get the maxillary-taming treatment).
💡 Think of it like this: Without headgear, the maxilla keeps moving forward like a train with no brakes. 🚂💨 Add high-pull headgear? Boom—slowed down! 🛑
Mandibular Growth: Myth or Reality?
Mandibular Effects: The Great Debate! 🤨⚖️
Functional appliances like the Activator + High-Pull Headgear have been stirring debates for decades:
| Camp 1: “Yes, Functional Therapy Grows the Mandible!” 📈 | Camp 2: “Nope, It’s Just Natural Growth!” 📉 |
|---|---|
| Demisch (1972) 🧑⚕️ | Harvold & Vargervik (1971) 🧑⚕️ |
| Owen (1981) 📚 | Wieslander & Lagerström (1979) 📚 |
| Luder (1982) 🔬 | Jacobsson & Paulin (1990) 🔬 |
| Toth & McNamara (1999) 🦷 | Forsberg & Odenrick (1981) 🦷 |
🤯 So, who’s right? Our study says… both have a point!
What Happened in Our Study? 🧐📊
Mandibular Advancement Findings
| Parameter | Treated Group (Activator + Headgear) | Control Group (No Treatment) | Significance |
|---|---|---|---|
| Mandibular advancement(mm) | ~3 mm forward 🚀 | Minimal change | ✅ |
| SNB increase (°) | +2.6° 📈 | +0.4° 📉 | ✅ Significant |
| Mandibular length (Go–Me) | Increased significantly 🦷📏 | Mild increase | ✅ Significant |
💡 What does this mean?
✔️ The mandible didn’t just sit back and relax—it advanced!
✔️ The SNB angle increased, meaning the lower jaw moved forward more than in untreated cases.
✔️ Mandibular length (Go-Me) increased significantly—suggesting real skeletal adaptation!
But WHY Did This Happen? 🔍
This isn’t just some mandibular magic trick—science explains it! 🧪✨
🔹 Condylar remodeling & Glenoid Fossa Relocation 🏗️
- The condyle remodels and moves forward in the fossa.
- This explains why the NSCo angle decreased & OLp-Co moved forward (Woodside et al., 1987; Ruf et al., 2001).
- Basically, the TMJ adapts to the new jaw position! 🦷
💡 Think of it as shifting a chair forward—if the condyle moves, so does the whole mandible! 🪑➡️
Quick Mnemonic to Remember Mandibular Changes! 🧠
🦷 “SNB = See the New Bite!”
(Because a Class II turns into a Class I as the jaw moves forward!)
🔹 Mandible advances (~3mm forward)
🔹 SNB increases (+2.6° 📈)
🔹 Go-Me increases (Mandibular growth 📏)
🔹 Condylar adaptation helps in Class II correction
Ortho Takeaway: What Should You Remember?
✅ Functional appliances help the mandible move forward, even if they don’t “grow” it like a plant. 🌱
✅ SNB increases, Go-Me increases, and the glenoid fossa adapts. 🦷
✅ The jaw doesn’t just grow—it adapts! It’s teamwork between remodeling & growth! 🛠️
🤔 What’s YOUR take? Do you think functional appliances really grow the mandible, or do they just help reposition it? Drop a comment below! 💬
What Happens to the Dentition?
Activator + headgear therapy isn’t just a bone game—it’s also a tooth tamer! 🦷🔧 Here’s the real MVP effect:
| Parameter | Treated Group 📊 | Control Group 💤 |
|---|---|---|
| Maxillary Incisor Retroclination 🦷⬅️ | 🔽 5.3° | No sig. change |
| Overjet Reduction 😁 | 🔽 5.4 mm | No sig. change |
| Mandibular Incisor Proclination 🦷➡️ | 🔼 2.0° | No sig. change |
| Overbite Decrease 📉 | 🔽 2.2 mm | No sig. change |
💡 Big takeaway?
👉 Overjet correction is a team effort—maxilla moves back, mandible moves forward, and incisors get into formation! 🎯
Upper Incisors: Pulling Back Like a Retreating Army 🚶♂️⬅️
📌 Activator + headgear retroclined the upper incisors by 5.3°
📌 Overjet reduced by 5.4 mm (thanks to a combo of skeletal & dental effects!)
📌 Even though the incisors were capped, lingual movement still happened! 🦷✨
🧐 Think of it like this: The upper incisors are stubborn party crashers who get forcibly escorted out by the headgear. 🚔👮♂️
Lower Incisors: The Sneaky Forward Movers 😏
📌 Mandibular incisors proclined by 2° despite being capped!
📌 Studies show this is unavoidable in functional therapy (Ahlgren & Laurin, 1976; Pancherz, 1984)
💡 Mnemonic to remember?
🔹 IMPA = Incisors Might Procline Anyway! 😂
Overbite: Bye-Bye Deep Bite! 👋
📌 Overbite reduced by 2.2 mm in the treated group!
📌 Why? More vertical face height = less deep bite!
📌 Studies agree! (Ahlgren & Laurin, 1976; Pancherz, 1984; Nelson et al., 1993)
🦷 Deep bite patients be like: “Wait, where did my overbite go?!” 😱
Ortho Takeaways 📝
✔️ Overjet correction = upper incisors move back + mandible moves forward
✔️ Upper incisors retrocline significantly (5.3°)
✔️ Lower incisors procline slightly (2°), despite capping
✔️ Overbite decreases by 2.2 mm = more open bite tendency
💬 What’s the most interesting dentoalveolar change you’ve noticed in your cases? Let’s discuss in the comment section! 🤓👇
Vertical Growth: The Mandibular Elevator Effect! 🚀⬆️
When we use an Activator + High-Pull Headgear, the mandible tends to grow vertically, thanks to a backward rotation effect. 📐 But why? Let’s see what the research says! 👀
| Who Said What? 📚 | Findings on Vertical Growth 📈 |
|---|---|
| Williams & Melsen (1982) 🧑⚕️📖 | Mandible grows more vertically due to backward rotation |
| Ruf et al. (2001) 🔬 | Backward rotation leads to increased face height |
| Cozza et al. (2004a,b) 📊 | Controlling vertical dimension is key for optimal forward jaw correction |
What Did Our Study Find? 🔍📊
| Parameter | Treated Group (Activator + Headgear) | Control Group (No Treatment) | Significance |
|---|---|---|---|
| Face height in molar region | Increased 📈 | No change | ✅ Significant |
| SN–PP Angle | Slight increase 🔄 | No change | ❌ Not significant |
| FH–OL Angle | Slight increase 🔄 | No change | ❌ Not significant |
| FMA Angle (Mandibular plane angle) | No major change 🤷♂️ | No change | ❌ Not significant |
| Overbite Correction | Significant ✂️ | Stable (No correction) | ✅ Significant |
🤔 What does this mean?
✔️ Mandibular vertical growth happens, but rotation balance is key! ⚖️
✔️ Face height increased, but overall vertical relationship remained stable.
✔️ Overbite correction was significant—thank you, double capping! 🙌
Why Does This Matter? 🤔
🔹 Overbite & Vertical Growth = Besties? 🦷💕
- Overbite correction was significant because the incisors were passively prevented from erupting (thanks to double capping), allowing molars to erupt instead.
- This controlled vertical development, preventing unwanted open bites.
🔹 Watch Out for Backward Rotation! ⏪
- If the face height increases too much, the mandible rotates backward, worsening Class II instead of fixing it. 😵
- Moral of the story: Control vertical growth, or you’ll have a long face. Literally. 😆
Mnemonic to Remember Vertical Growth Effects! 🎯
🦷 “Class II? Keep It FLAT! 😎”
(Because controlling vertical dimension = better forward jaw correction!)
🔹 FMA = Flat Mandibular Angle = No significant change
🔹 Overbite correction was significant (Double capping = good prognosis!)
🔹 Vertical Growth needs control, or pogonion moves BACK! 😵
Ortho Takeaway: What Should You Remember?
✅ Mandible grows more vertically with activator therapy, but watch for backward rotation.
✅ Overbite correction was significant thanks to molar eruption.
✅ FMA remained stable, showing that vertical control was maintained.
✅ Class II correction isn’t just about moving forward—it’s about balancing vertical growth too!
Facial Profile: What Changed? 🧐
When we talk about Class II treatment, we often focus on bones and teeth—but what about the soft tissue? 🤔 Your patients don’t walk around showing off their cephs, right? It’s the face they care about! 😆
Here’s what happened when we used an Activator + Headgear Combo:
| Soft Tissue Parameter | Treated Group (Activator + Headgear) | Control Group (No Treatment) | Significance✅❌ |
|---|---|---|---|
| Facial convexity angle 🏔️ | Increased (More balanced profile) | Reduced (Got worse) | ✅ Significant |
| Upper lip–x-axis distance 👄 | Increased (Lip moved slightly forward) | No major change | ✅ Significant |
| Mlf–y-axis & Pg′–y-axis (Pogonion & Labiomental fold) 🧐 | Increased (Chin moved forward, fold depth reduced) | Slight increase | ✅ Significant |
| Sls–x-axis distance (Soft tissue sulcus) 📏 | Increased (More balanced sulcus) | Slight increase | ✅ Significant |
| Horizontal soft tissue menton (Me′–x-axis) 🧔 | Increased (Chin grew forward!) | Slight decrease | ✅ Significant |
| Labiomental fold depth (Mlf–E line distance) ✂️ | Decreased (Less deep fold = smoother profile) | Slight increase (Got worse) | ✅ Significant |
What Does This Mean? 🤓
✔️ Chin & pogonion moved forward → Say goodbye to recessive chins! 👋
✔️ Labiomental fold became shallower → No more deep, exaggerated folds! 🔄
✔️ Upper lip projection slightly increased → But without making patients look “duck-lipped” 🦆😂
✔️ Soft tissue sulcus balance improved → A more harmonious lower face
Translation? 📢 Activator + Headgear = More balanced, attractive profiles! 💁♂️💁♀️
But Why Does This Happen? 🤔
🟢 High-pull headgear = Restrains maxilla → So it doesn’t grow too far forward
🟢 Activator = Encourages mandibular forward growth → Bye-bye, retrognathic chin!
🟢 Labiomental fold = Naturally flattens as the chin moves forward
Think of it as sculpting a masterpiece 🖌️—you’re not just fixing teeth; you’re enhancing the whole face! 😎
Mnemonic to Remember: “CHIN UP!” ✨
💡 C = Convexity Angle Increases (Balanced profile)
💡 H = Horizontal Menton Growth (Chin moves forward)
💡 I = Improved Sulcus Balance
💡 N = No More Deep Labiomental Fold
💡 U = Upper Lip Projection Slightly Increased
💡 P = Pogonion Moves Forward
So next time you see a Class II patient, tell them:
“Don’t worry—after treatment, you’ll have a ‘CHIN UP’ moment!” 😆
Final Ortho Takeaway 📌
✅ Functional appliances + headgear improve soft tissue harmony 🏆
✅ Patients get better chin projection & smoother profiles 💁♀️
✅ The labiomental fold decreases, so no more harsh chin lines 🚫⏳
✅ This treatment doesn’t just fix bones—it enhances faces! 🤩
💬 What’s your favorite soft tissue change in ortho treatment? Drop a comment below! 🗣️👇