The Kennedy classification would be difficult to apply to every situation without certain rules for application. Applegate has provided the following eight rules governing the application of the Kennedy method.
RULE 1: Classification should follow rather than precede any extractions of teeth that might alter the original classification.
RULE 2: If a third molar is missing and not to be replaced, it is not considered in the classification.
RULE 3: If a third molar is present and is to be used as an abutment, it is considered in the classification.
RULE 4: If a second molar is missing and is not to be replaced, it is not considered in the classification (for example, if the opposing second molar is likewise missing and is not to be replaced).
RULE 5: The most posterior edentulous area (or areas) always determines the classification.
RULE 6: Edentulous areas other than those determining the classification are referred to as modifications and are designated by their number.
RULE 7: The extent of the modification is not considered, only the number of additional edentulous areas.
RULE 8: There can be no modification areas in Class IV arches. (Another edentulous area lying posterior to the “single bilateral area crossing the midline” would instead determine the classification).
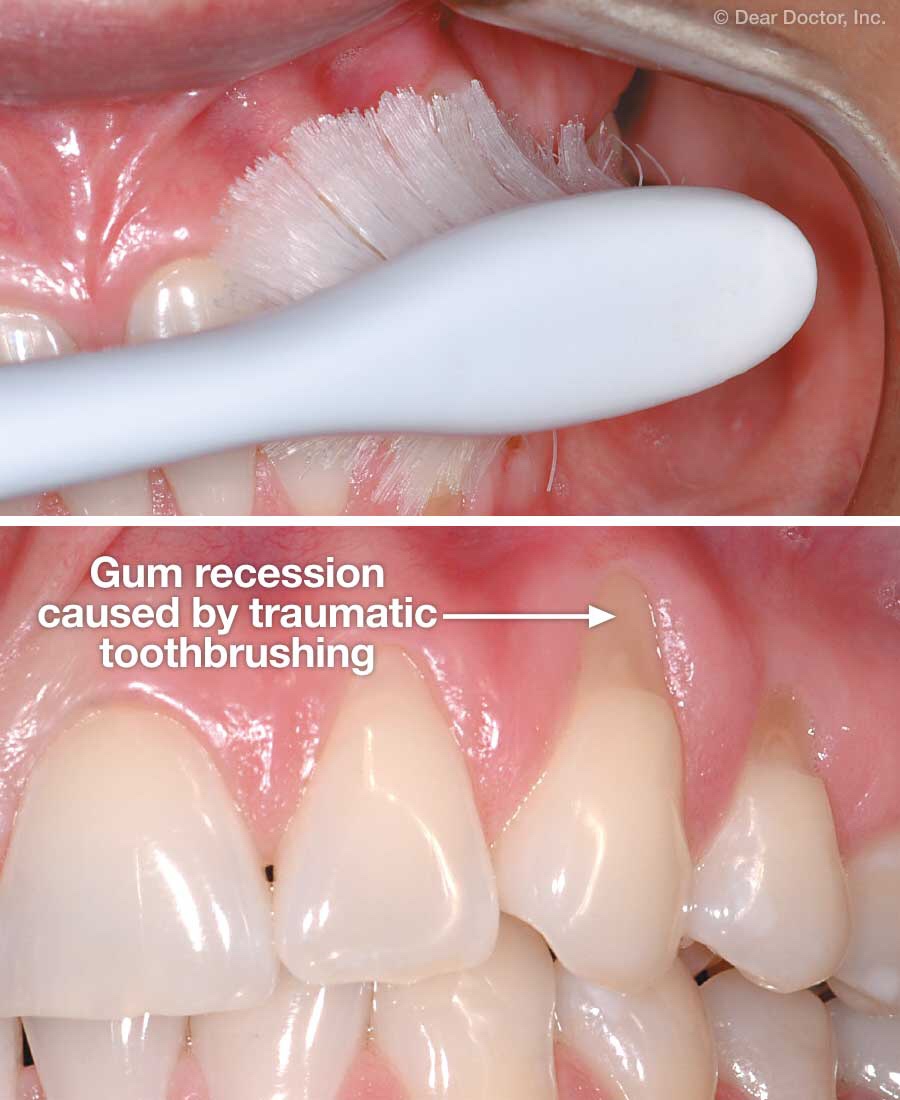
In simple words, Abrasion is loss of tooth structure due to foreign substances , like heavy brushing, hard bristels. Abrasion occours in the cervical region of tooth
Etiology
Faulty oral hygiene practice
Horizontal brushing
Excessive forces
Quality of toothbrush
pH and amount of dentifrice used
Ill-fitting clasps of partial dentures cause localised abrasion lesions
Fiction from toothpicks and interproximal brushes
Tobacco Chewing
Treatment
We need to take careful consideration of aetiology and progression of the condition. That means, correct diagnosis is the prerequisite for the management of the lesion.
If the lesion is localized and not interfering with the physiological function of the stomatognathic system = It may be restored
If the abrasion is generalized and substantial = the habit should be discontinued and controlled
If teeth are sensitive = use Flouride application
If it’s class V lesion = Restoration with GIC
If lesion involves a none conscious area in the posterior teeth = use metallic restorationon
It involves all supporting structures which is composed of:
gingiva
alveolar mucosa
cementum
periodontal ligament
alveolar bone
Slowly progressive disease
It occurs in response to plaque and calculus.
It progresses aggressively in patients with
diabetes: type I
Smoking habits: more attachment loss and bone loss, more furcation involved, and deeper pockets.
Thyroid condition
It can occur in childhood and adolescence also
What is pocket?
It is pathological deepened cervical gingiva. We can observe that junctional epithelium (attachment of gingival structure) is broken down or detached from coral end. This causes deepened sulcus. Hence, Plaque and calculus are deposited.
Clinical Features
Gingival Inflammation is present
We can see pocket formation
Slight: 1-2mm
Moderate: 3-4 mm
Severe: 5 mm or more
Loss of attachment (recession)
Presence of inflammatory swelling
Colour ranges from pale red to magenta
Loss of stippling
Blunted or rolled gingival margin
Blunt or flattened interdental papilla
All the signs of inflammatory may not always be present
May bleed on probing the pocket
Increased gingival fluid exudation
Purulent exudate may be present
Signs of inflammatory may be masked because of fibrotic changes
Horizontal and Vertical bone loss
Progressive increase in the mobility of teeth involved due to bone loss
How do you differentiate periodontitis and gingivitis?
It’s simple, in giginvitis, you can observe no bone loss and mobility whereas, in periodontitis, you can observe mobility, deep pockets and recession.
Differential Diagnosis
Age of patient
Rate of disease progression
Familial nature of the aggressive disease
Can be correlated with the amount of plaque and calculus present
How to calculate whether chronic periodontitis is generalised or localised based on number of teeth?
Rules:
Generalised – when >30% of teeth show attachment loss
Localised- when <30% of teeth show attachment loss
Let’s consider two type of patents.
In patient A, the number of teeth is 32.
We calculate 30% of total teeth, which means 10 teeth are affected by periodontitis. This denotes patient has the generalized condition.
If 7 teeth have recession and pockets, that’s is less than 10. The patient had localized condition.
In patient B, the total number of teeth is 28
We calculate 30% of 28 teeth, which means 8 teeth are affected. This denotes patient has a generalized condition.
If 6 teeth have recession and pockets, that’s is less than 8. The patient had localized condition.
Symptoms
Usually painless due to absence of receptors
Sometimes, localised dull pain radiating deep into the jaw during brushing
Sensitivity to hot and cold or both due to exposure of root dentin. The sensation will be tingling
Food lodgement in the areas of bone loss cause discomfort
Due to food accumulation, patients feel itchness in the gingiva. They try to remove it using a toothpick.
Disease Progression
Slow rate- depends on the post immunity but ageing or disease factors or diabetes play a role in the rate.
Onset can occur at any time in the presence of calculus and plaque at site-specific surfaces.
It is more evident in the mid-30s due to accumulative effect.
Some areas progress at a faster rate or slower rate.
Faster Rate- due to more accumulation of plaque and short conical roots such as anteriors