Category: Uncategorized
DENTIN HYPERSENSIVITY
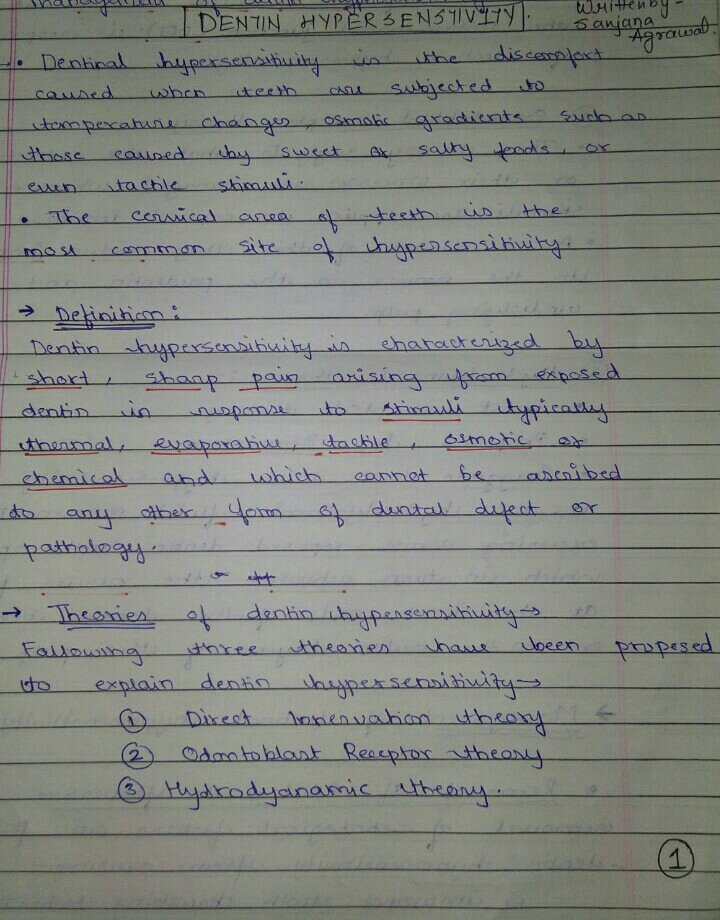
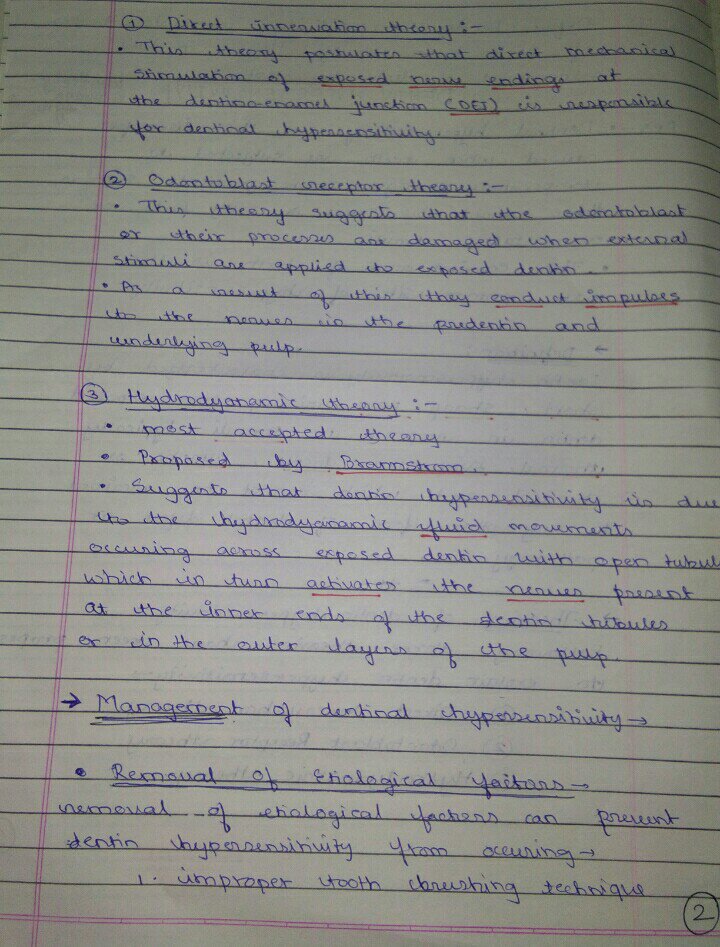
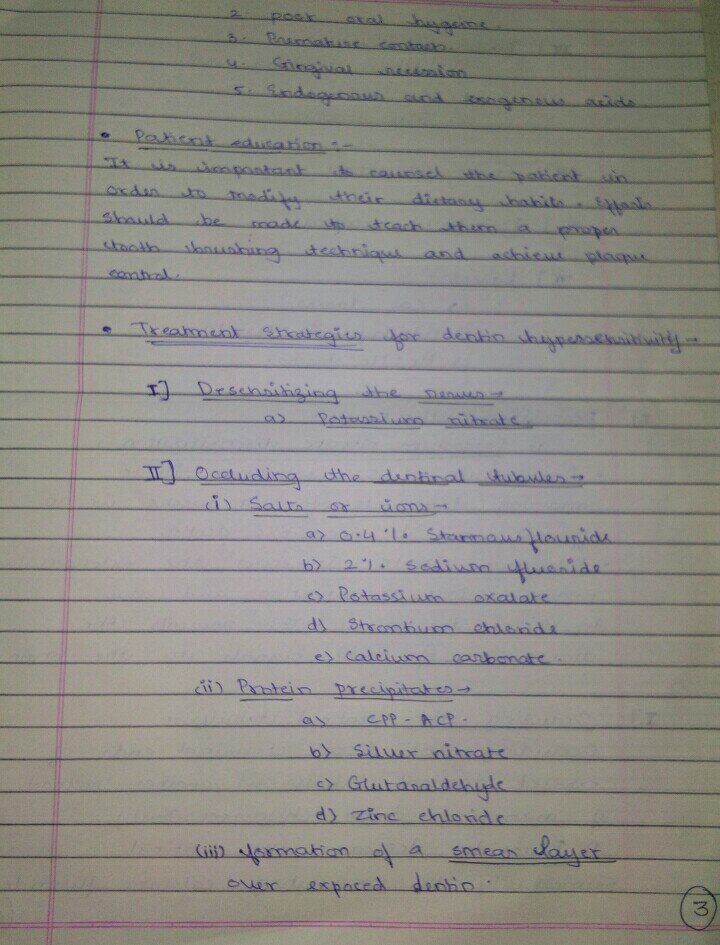

SOURCE – RAMYA RAGHU TEXTBOOK
PEDODONTIC TRIANGLE
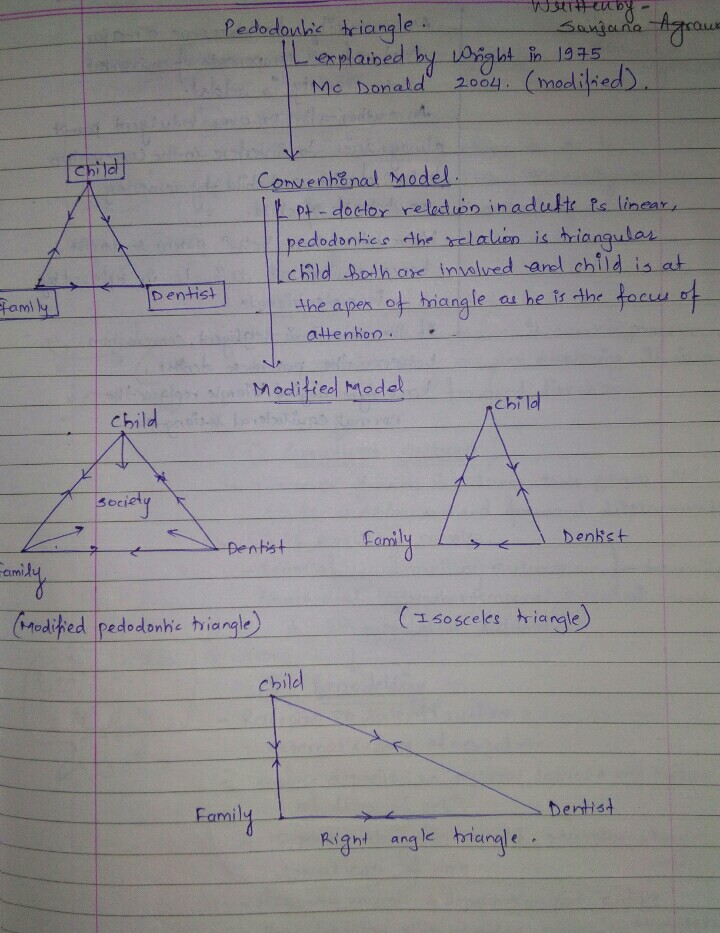
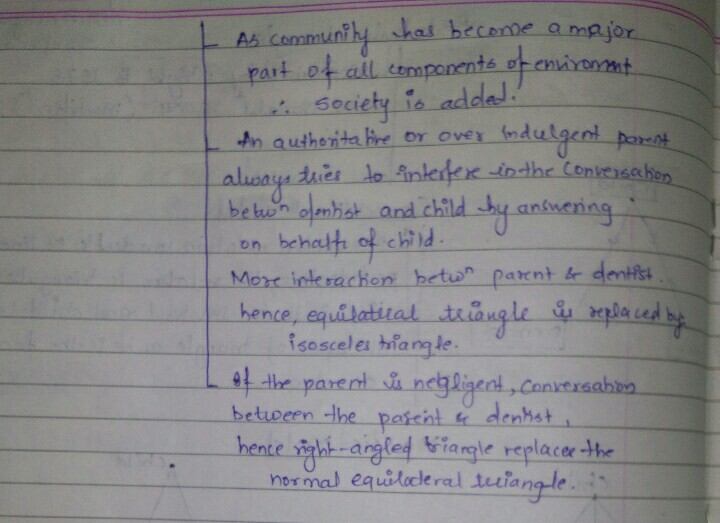
SOURCE – NIKHIL MARVA TEXTBOOK
Thyrotoxicosis
A good way to help you remember is to think of this hormone system like a house’s heating system. In this example, the thyroid gland is the furnace, the pituitary gland is the thermostat, and the hypothalamus is the person living in the house. When the house is cold, the person sets the thermostat to signal the furnace to make heat. When the house grows warmer, the system shuts off.
In hyperthyroidism, the system never shuts off, causing the release of too many thyroid hormones. For this lesson, we’ll focus on two of them: T3 (tri-iodothyronine) and T4 (thyroxine).
The thyroid needs iodine to make T3 and T4. Thyroid cells absorb iodine and combine it with the amino acid tyrosine to make these hormones. About 80% is T4, and 20% is T3.
Too much of T3 and T4 results in thyrotoxicosis. There is a subtle difference between hyperthyroidism and thyrotoxicosis – hyperthyroidism means having an overactive thyroid gland, while thyrotoxicosis is the condition of having increased levels of T3 and T4 in the blood. Thyrotoxicosis can be caused by taking too much thyroid medication, for example, or having thyroiditis (an inflamed thyroid).
Causes of thyroid hormone excess include
- Primary hyperthyroidism (Graves’ disease, toxic multinodular goiter [MNG], toxic adenoma, iodine excess)
- Thyroid destruction (subacute thyroiditis, silent thyroiditis, amiodarone, radiation)
- Extrathyroidal sources of thyroid hormone (thyrotoxicosis factitia, struma ovarii, functioning follicular carcinoma)
- Secondary hyperthyroidism (TSH-secreting pituitary adenoma, thyroid hormone resistance syndrome, human chorionic gonad- otropin [hCG]-secreting tumors, gestational thyrotoxicosis).
- Graves’ disease, caused by activating TSH-receptor antibodies, is the most common cause of thyrotoxicosis and accounts for 60–80% of cases.
- Its prevalence in women is 10-fold higher than in men; its peak occurrence is at age 20–50 years.
Clinical Features
- Anxiety, restless, and fidgety.
- weight loss with increased appetite
- frequent bowel movements
- heat intolerance
- excessive sweating
- oligomenorrhea
- Skin is warm and moist
- Cardiovascular findings include tachycardia, systolic hypertension, systolic murmur, and atrial fibrillation.
- Fingernails may separate from the nail bed (Plummer’s nails).
- Eyelid retraction and lid lag may be present.
- A fine tremor, hyperreflexia, and proximal muscle weakness also may be present.
- Long-standing thyrotoxicosis may lead to osteopenia.
- In the elderly, the classic signs of thyrotoxicosis may not be apparent, the main manifestations being weight loss and fatigue (“apathetic thyrotoxicosis”).
In Graves’ disease,
- the thyroid is usually diffusely enlarged to two to three times its normal size
- a bruit or thrill may be present.
- Infiltrative ophthalmopathy (with variable degrees of proptosis, periorbital swelling, and ophthalmoplegia)
- dermopathy (pretibial myxedema) also may be found;
- these are extrathyroidal manifestations of the autoimmune process.
In subacute thyroiditis,
- the thyroid is exquisitely tender and enlarged with referred pain to the jaw or ear
- Sometimes accompanied by fever and preceded by an upper respiratory tract infection.
- Solitary or multiple nodules may be present in toxic adenoma or toxic MNG.
Thyrotoxic crisis, or thyroid storm, is rare, presents as a life-threatening exacerbation of hyperthyroidism, and can be accompanied by fever, delirium, seizures, arrhythmias, coma, vomiting, diarrhea, and jaundice.

- Serum TSH is a sensitive marker of thyrotoxicosis caused by Graves’ disease, autonomous thyroid nodules, thyroiditis, and exogenous levothyroxine treatment.
- Elevation of bilirubin, liver enzymes, and ferritin.
- Thyroid radioiodine uptake may be required to distinguish the various etiologies: high uptake in Graves’ disease and nodular disease versus low uptake in thyroid destruction, iodine excess, and extrathyroidal sources of thyroid hormone.
Hypothyroidism
The thyroid gland is found at the base of your neck and lies just below your Adam’s apple. This gland produces hormones that are important to your metabolism, known as T3 and T4.
- Some T3 is secreted by the thyroid, but most is produced by deiodination of T4 in peripheral tissues.
- Both T4 and T3 are bound to carrier proteins (thyroid-binding globulin [TBG], transthyretin [binds T4], and albumin) in the circulation.
- Increased levels of total T4 and T3 with normal free levels are seen in states of increased carrier proteins (pregnancy, estrogens, cirrhosis, hepatitis, and inherited disorders).
- Conversely, decreased total T4 and T3 levels with normal free levels are seen in severe systemic illness, chronic liver disease, and nephrosis.
Since we know that the thyroid hormones play an important role in regulating your body’s metabolism, it makes sense that a decrease in these hormones would lead to symptoms such as a loss of energy, an increased need for sleep, an intolerance to cold, a slow pulse, constipation, weight gain, and depression
causes
- Autoimmune hypothyroidism: Hashimoto’s thyroiditis, atrophic thyroiditis
- Subtotal or total thyroidectomy
- Neck radiation in cancer patients suffering with Hodgkins lymphoma and laryngeal cancer
- Drugs: iodine excess, lithium and antithyroid drugs
- Congenital hypothyroidism
- Iodine deficiency
- Infiltrative disorders: amyloidosis and sarcoidosis
- Transient – Postpartum thyroiditis and Subacute thyroiditis
- Withdrawal of thyroxine treatment
- Secondary- Hypopituitarism and Hypothalamic disease, tumors, trauma, infiltrative disorders, idiopathic
Clinical Features
- lethargy/ fatigue
- mild weight gain with poor appetite
- constipation
- cold intolerance
- cool peripheral extremities.
- menorrhagia
- dry skin and hair loss,
- difficulty concentrating and poor memory
- Cardinal features on examination include
– bradycardia,
– mild diastolic hypertension - prolongation of the relaxation phase of deep tendon reflexes
- Goiter may be palpated, or the thyroid may be atrophic and nonpalpable.
EVALUATION OF HYPOTHYROIDISM
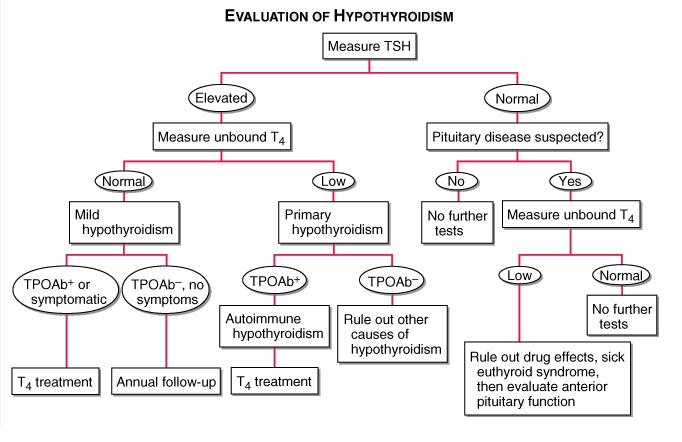
- TPOAb+, thyroid peroxidase antibodies present; TPOAb–, thyroid peroxidase antibodies not present;
- Decreased serum free T4 is common to all varieties of hypothyroidism.
- An elevated serum TSH is a sensitive marker of primary hypothyroidism but is not found in secondary hypothyroidism.
- Elevated cholesterol
- Increased creatine phosphokinase
- Anemia may be present
- Bradycardia, low-amplitude QRS complexes, and flattened or inverted T waves may be present on ECG.
Treatment
- Adult pts <60 years without evidence of heart disease may be started on 50–100 μg of levothyroxine (T4) daily.
- In the elderly or in pts with known coronary artery disease, the starting dose of levothyroxine is 12.5–25 μg/d.
- In secondary hypothyroidism, TSH levels cannot be used, and therapy needs to be guided by free T4 measurement.
- Women on levothyroxine replacement should have a TSH level checked as soon as pregnancy is diagnosed, as the replacement dose typically increases by 30–50% during pregnancy. Failure to recognize and treat maternal hypothyroidism may adversely affect fetal neural development.
- Therapy for myxedema coma should include levothyroxine (500 μg) as a single IV bolus followed by daily treatment with levothyroxine (50–100 μg/d), along with hydrocortisone (50 mg every 6 h) for impaired adrenal reserve, ventilatory support, space blankets, and treat- ment of precipitating factors.
Acromegaly
Gigantism Versus Acromegaly
It is all about increase production of growth hormone and when the long bone in the leg, called the epiphysis plate, fuses. If the epiphysis plate has not fused before puberty and there is a large amount of growth hormone being released from the pituitary gland, the person is considered to have gigantism. If the epiphysis plate has fused after puberty and there is a large amount of growth hormone being released from the pituitary gland, the person is considered to have acromegaly.
 |
Causes
- PituitarySources: Somatotrope adenomas and mammosomatotrophe adenomas
- Extra Pituitary Sources: Pancreatic adenoma (islet cell tumour) and excessive GnRh production by carcinoid tumor
Clinical Features
The peak occurrence of acromegaly is at age 40–45. Now that we understand how someone is diagnosed with acromegaly, let’s take a look at what a person would look like with this condition. Because the epiphysis bone has fused, they will not get taller, but bones and organs will enlarge.
They will have big hands, feet, and forehead:
- ring tightening
- increased shoe or glove size
- frontal bossing
Their organs and glands will enlarge and cause associated diseases:
- cardiomyopathy
- left ventricular hypertrophy
- diastolic dysfunction
- colon polyps, and colonic malignancy.
- an enlarged thyroid
- Increase in sebum = oily skin
- Peripheral resistance will increase = hypertension
Also, they could have an increase in blood glucose because the increase of growth hormone stops insulin from carrying the glucose out of the blood in to the tissues. So the glucose (sugar) hangs out in the blood.
- glucose intolerance
- diabetes mellitus
Other unique features:
- Thick heel pads
- Deep voice
- Hyperhidrosis
- Skin tags
- Osteoarthritis: bilateral limbs and weight gain
- Spade like hand
- Obstructive sleep apnea
- Visual deficit
- Carpal tunnel syndrome.
Oral Manifestations
- Widened teeth spacing
- mandibular enlargement with prognathism,
- macroglossia
Overall mortality is increased approximately threefold.
Diagnosis
- Insulin-like growth factor type I (IGF-I) levels are a useful screening measure with elevation suggesting acromegaly.
- Investigation of choice: Due to the pulsatility of GH, measurement of a single random GH level is not useful for screening. The diagnosis of acromegaly is confirmed by demonstrating the failure of GH suppression to <0.4 μg/L within 1–2 h of a 75-g oral glucose load.
- MRI of the pituitary usually reveals a macroadenoma.
- Serum prolactin levels are increased in acromegaly
- X-ray of Foot
Treatment
- The primary treatment modality for acromegaly is transsphenoidal surgery.
- GH levels are not normalized by surgery alone in many pts with macro-adenomas; in those, somatostatin analogues provide adjunctive medical therapy that suppresses GH secretion with modest to no effect on tumour size.
Drugs: Octreotide, Lanreotide and Pasireotide - The GH receptor antagonist pegvisomant can be added in pts who do not respond to somatostatin analogues. Pegvisomant is highly effective in lowering IGF-I levels but does not lower GH levels or decrease tumor size.
- Pituitary irradiation may also be required as adjuvant therapy but has a slow therapeutic onset and a high rate of late hypopituitarism.
Jaundice
Liver produces important proteins, such as albumin, which ensures you don’t look swollen, and allows for the transport of important drugs. It helps to detoxify things that may be dangerous to your health. It also helps to give you energy by generating glucose, and so much more!
What Is Bile and Bilirubin?

Other than all of the things that I just mentioned the liver is important for, it’s also important for the production of something known as bile. This is a greenish liquid produced in the liver and stored in the gallbladder, which facilitates the digestion of fat.
Bile, among other things, contains something known as bilirubin. Bilirubin is an orange-yellow pigment formed from the breakdown of red blood cells. Bilirubin is converted into other substances that eventually give urine its yellow color and feces its yellow-brown color. Who knew physiology could be so colorful and yet so disgusting?
When red blood cells break down due to age or destruction, then something known as unconjugated or indirect or water-insoluble bilirubin is released into the bloodstream. Once this unconjugated bilirubin enters the liver, the liver converts it into conjugated or direct or water-soluble bilirubin by tacking on a compound known as glucuronic acid; this is what makes bilirubin water soluble.
This newly water-soluble bilirubin is then secreted into the watery bile and, from there, into the intestines.
If all of this is making your head spin, don’t worry; we can simplify it even more. Your liver is like a giant factory. Through one end, raw ingredients come in by the truckload. In our case, that’s crates and crates of raw, hard, and unprocessed indirect bilirubin. Once inside the factory, the workers take a piece of unconjugated bilirubin and stick another ingredient right onto it, thereby making an entirely new concoction, called conjugated bilirubin. This conjugated bilirubin isn’t hard like unconjugated bilirubin; it’s slushy and can dissolve easily in water instead.
If the levels of either the conjugated or unconjugated bilirubin increase in the body, they can cause icterus, which is the more technical term for jaundice. If you are not sure of what jaundice is, then let me explain. Jaundice is the yellowing of the whites of the eyes, mucous membranes, and a person’s skin as a result of abnormally increased levels of bilirubin in the blood, aka hyperbilirubinemia.
What Causes Unconjugated Hyperbilirubinemia?
Based on what I’ve said thus far, you should be aware that the ways by which levels of unconjugated bilirubin can increase are:
- if something causes indirect bilirubin levels to rise before they reach the liver
- if unconjugated bilirubin isn’t being delivered properly to the liver (both of which are also known as pre-hepatic causes)
- if there’s something wrong with the liver that disables the conversion mechanism to conjugated bilirubin (also known as hepatic causes)
Types of Jaundice
Pre-Hepatic
- In pre-hepatic jaundice, there is excessive red cell breakdown which overwhelms the liver’s ability to conjugate bilirubin. This causes an unconjugated hyperbilirubinaemia.
- Any bilirubin that manages to become conjugated will be excreted normally, yet it is the unconjugated bilirubin that remains in the blood stream to cause the jaundice.
Hepatocellular
- In hepatocellular (or intrahepatic) jaundice, there is dysfunction of the hepatic cells. The liver loses the ability to conjugate bilirubin, but in cases where it also may become cirrhotic, it compresses the intra-hepatic portions of the biliary tree to cause a degree of obstruction.
- This leads to both unconjugated and conjugated bilirubin in the blood, termed a ‘mixed picture’.
Post-Hepatic: Post-hepatic jaundice refers to obstruction of biliary drainage. The bilirubin that is not excreted will have been conjugated by the liver, hence the result is a conjugated hyperbilirubinaemia.
Laboratory Tests
Any patient presenting with jaundice should have the following bloods taken:
- Liver function tests (LFTs), as summarised in Table 2
- Coagulation studies (PT can be used as a marker of liver synthesis function)
- FBC (anaemia, raised MCV, and thrombocytopenia all seen in liver disease) and U&Es
- Specialist blood tests, as summarised below as part of a liver screen
| Blood Marker | Significance |
| Bilirubin | Quantify degree of any suspected jaundice |
| Albumin | Marker of liver synthesising function |
| AST and ALT | Markers of hepatocellular injury* |
| Alkaline Phosphatase | Raised in biliary obstruction (as well as bone disease, during pregnancy, and certain malignancies) |
| Gamma-GT | More specific for biliary obstruction than ALP (however not routinely performed) |
Table 2 – LFT serum markers. *as an estimate, if the AST:ALT ratio >2, this is likely alcoholic liver disease, whilst if AST:ALT is around 1, then likely viral hepatitis as the cause
Liver Screen
A liver screen can be performed for patients whereby there is no initial cause for liver dysfunction, tailored to whether acute or chronic liver failure
| Viral Serology | Non-Infective Markers | |
| Acute Liver Injury | Hepatitis A, Hepatitis B, Hepatitis C, and Hepatitis ECMV and EBV | Paracetamol levelCaeruloplasminAntinuclear antibody and IgG subtypes |
| Chronic Liver Injury | Hepatitis BHepatitis C | CaeruloplasminFerritin and transferrin saturationTissue Transglutaminase antibodyAlpha-1 antitrypsinAutoantibodies* |
Table 3 – Acute and Chronic Liver Screens *Autoantibodies include anti-mitochondrial antibody (AMA), anti-smooth-muscle antibody (Anti-SMA), and anti-nuclear antibody (ANA), used to identify a variety of autoimmune liver conditions, such as primary sclerosing cholangitis (PSC)
Imaging
The imaging used will depend on the presumed aetiology. An ultrasound abdomen is usually first line, identifying any obstructive pathology present or gross liver pathology (albeit often user dependent).
Magnetic Resonance Cholangiopancreatography (MRCP) is used to visual the biliary tree, typically performed if the jaundice is obstructive, but US abdomen was inconclusive or limited, or as further work-up for surgical intervention.
A liver biopsy can be performed when the diagnosis has not been made despite the above investigations.
Management
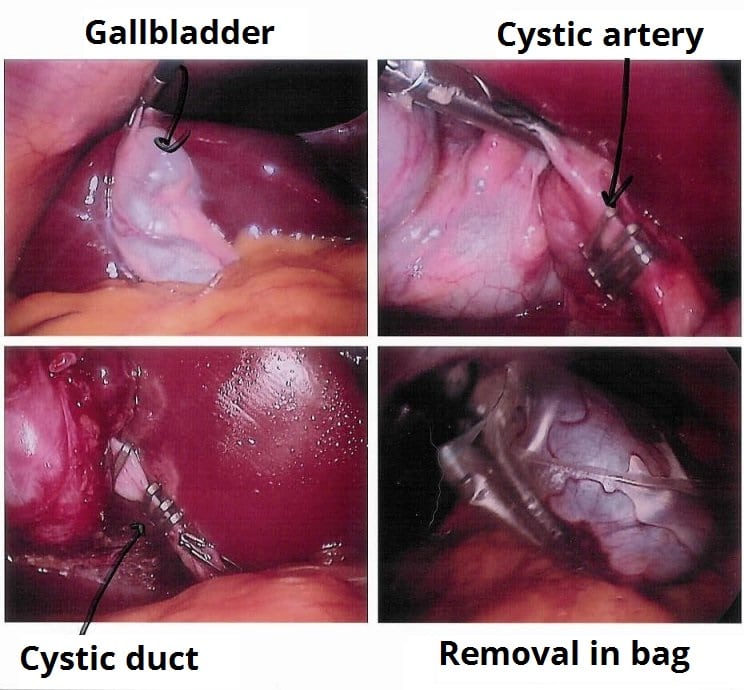
The definitive treatment of jaundice will be dependent on the underlying cause. Obstructive causes may require removal of a gallstone through Endoscopic Retrograde CholangioPancreatography (ERCP) or stenting of the common bile duct.
Symptomatic treatment is often needed for the itching caused by hyperbilirubinaemia. An obstructive cause may warrant cholestyramine (acting to increase biliary drainage), whilst other causes may respond to simple anti-histamines.
Identify and manage any complications where possible. Monitor for coagulopathy, treating promptly (either vitamin K or fresh frozen plasma (FFP) is needed) if any evidence of bleeding or rapid coagulopathy, and treat hypoglycaemia orally if possible (otherwise 5% dextrose is needed).
Where patients become confused from decompensating chronic liver disease (‘hepatic encephalopathy’), laxatives (lactulose or senna) +/- neomycin or rifaximin may be used, in attempt to reduce the number of ammonia-producing bacteria in the bowel.By User:Pschemp [CC-BY-SA-3.0], via Wikimedia Commons
PREMALIGNANT LESIONS AND CONDITIONS

source – don’t remember, had written it long back , textbook – Shafers
Hepatitis C
Two Different Cases Of Hepatitis C Virus
Hepatitis is a term that means inflammation of the liver. It can be caused by many different things, one of which can be from a virus. Let’s take a retrospective look at two people who unknowingly had a Hepatitis C virus.
Jacob was in his twenties when he was seriously injured in a car accident. Through his long recovery, he became addicted to his pain medication. It became quite severe and when the doctor stopped prescribing his pain medication, he turned to heroine. That’s how he met Anna. They both struggled with heroine addiction, injecting the drug at least once daily.
As their lives spiraled out of control, they resorted to riskier practices of drug use and were sharing needles with people they didn’t even know. Several weeks after this began, Anna became ill with flu-like symptoms and Jacob did not. It was a common illness and not too much thought was given to it.
Thankfully after a series of events, both Jacob and Anna successfully completed rehab and led a successful life. Now, Jacob was in his forties and he became ill. His skin was yellow in color and his abdomen was distended.
Both Jacob and Anna had the Hepatitis C virus. Anna’s illness was acute meaning that it lasted less than six months. Although she never knew she had Hepatitis C, she was part of the small percentage that fully recover without treatment. Jacob had a chronicinfection meaning that it lasted more than six months, in fact it lasted twenty years for him. Even though he had the infection all of this time, he was unaware of it until he developed symptoms from his advanced liver damage.

It is bloodborne, meaning it is spread from one person to another in the blood. The majority of cases are due to injected drug use in which needles are shared.
Since 1992, donated blood has been tested for Hepatitis C but prior to this people could contract a Hepatitis C virus through receiving blood transfusions. Inadequate medical equipment sterilization can also spread Hepatitis C from one person to another. It can be passed from mother to baby during childbirth but it is not passed through breast milk. It can be passed from one to another through sexual intercourse.
Unique Features
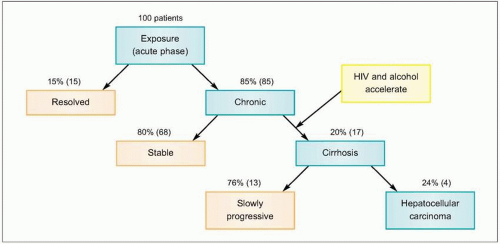
- most common cause of cirrhosis is HCV
- most common cause of acute viral hepatitis leading to chronic hepatitis ( Risk of conversion)
- Hallmark feature = pauci inflammatory reaction in acute phase
- Virus that comes in acute phase causes chronicity
- HCV inhibit insulin function leading to post receptor signalling of insulin resistance
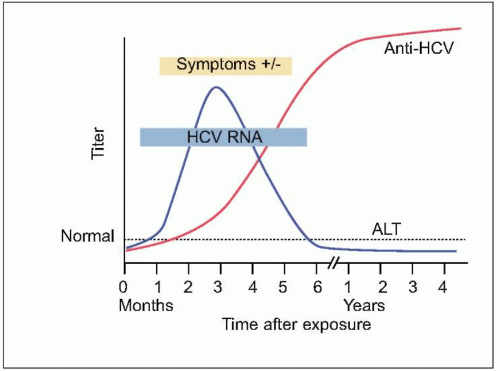
The majority of Hepatitis C infections do not have any symptoms present. As we saw with Jacob, he didn’t show any symptoms and was unaware that he had Hepatitis C. With chronic Hepatitis C, a person can remain asymptomatic for decades. They are usually only diagnosed after they start having symptoms from advanced liver disease as a result of the Hepatitis C virus.
Serology
- HCV RNA = Gold standard marker for diagnosis of HCV
- Anti HCV = Screening test of choice (IgG)
Hepatitis B
Hepatitis B is a virus that occurs in the liver. It can be acute or chronic.
Stacey is a 36-year-old woman. She has not been feeling well lately. Her symptoms are general, and she thinks she is just run down or getting the flu. She is tired, has no appetite, has abdominal pain, and has a headache. However, today Stacey noticed that her urine is a little dark. She decides to go see her doctor.
Hepatitis B is a virus of the liver. It can be acute, meaning that a person will have hepatitis B for a short period of time and then get better. Hepatitis B can also be chronic, meaning that it can cause a long-term infection and will eventually cause damage to the liver. Sometimes there are no symptoms associated with hepatitis B, but it is still contagious to others as long as it is present in the body.
Symptoms of Hepatitis B
- Liver damage is by sensitised T lymphocytes (most common)
- Virus has direct cytopathic effect, damaging the liver directly by virus
- HBV causes immune complex disease due to HBsAg + Anti HBs participation
- This complex immune disease manifests as serum sickness like illness ( Rash, Arthralgia, High grade fever) It is Type III Hypersensitive Reaction
Associated with unrelated diseases because these disease MOT is different
- leprosy
- down syndrome
- hodgkin lymphoma- Paul Ebstein like fever, after taking alcohol, pain occurs in lymph node.
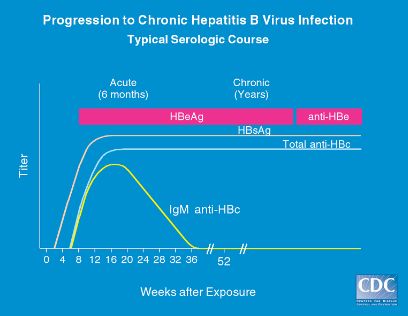
Interpreting Hepatitis B Serology in 5 Easy steps
A unique feature contributing to its virulence, is its ability to trick the host’s immune system by producing decoy antibodies. These decoy antibodies confuse the immune system and make the virus more difficult to fight.
Upon exposure to a virus, the body will produce antibodies against it. These antibodies are detectable in the blood. Hepatitis B surface antibodies, HBsAB provide immunity because the body can now recognize the virus and fight it. Presence of HBsAB can be the result of passive or active immunity immunity. Passive immunity occurs as a result of receiving the hepatitis B vaccine. Active immunity occurs after a previous hepatitis B infection.
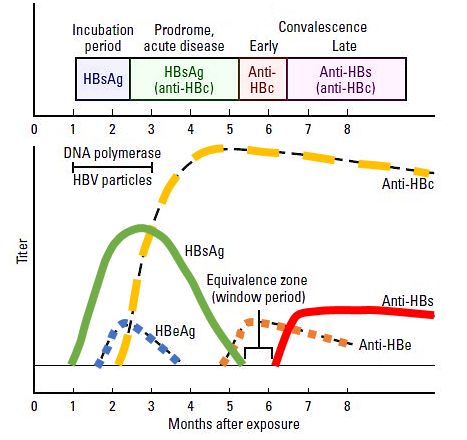
Hepatitis B surface antigen (HBsAg)
- Appears during incubation period (1-6 months), 2-7 weeks prior to symptoms.
- Peaks when the patient is most ill.
- Becomes undetectable in 3-6 months.
- Indicates infection – recent or chronic.
Hepatitis B surface antibody (anti-HBs or HBsAb)
- Arises once the acute disease has resolved.
- Sometimes, not detectable unless until weeks or months after HBsAg has disappeared. This gap is called “window” period.
- Indicates, immunity (by vaccination or infection).
Hepatitis B core antibody (anti-HBc or HBcAb)
- Anti-HBc IgM and elevated serum transaminases also appear shortly before the symptom onset.
- Over the next few months, anti-HBc IgM is replaced with an IgG component.
- IgM = Recent (Acute) infection
- IgG = Chronic infection
Hepatitis B e-antigen (HBeAg)
- Shortly after HBsAg appears, HBeAg and HBV DNA can be detected in the serum and are markers of the acute viral replication.
- Predictor of infectivity
Hepatitis B e-antibody (anti-HBe or HBeAb)
- Anti-HBe appears shortly after HBeAg vanishes and indicates subsiding viral activity.
- Predictor of low infectivity.
Causes of Hepatitis B
Hepatitis B is transmitted by body fluids including blood, saliva, semen, and vaginal secretions. It moves through mucous membranes and breaks in the skin. It can also be transmitted from mother to baby during birth. Specific actions and populations that increase the risk of contracting hepatitis B are:
- Unprotected sex with someone infected with hepatitis B
- Getting a tattoo or piercing with an unsterilized needle
- Sharing drug needles with an infected person
- Sharing razors or toothbrushes with someone infected with hepatitis B
- People who are frequently exposed to blood, blood products, or other body fluids
- Health care workers
- Travelers who go to areas with uncertain sanitary conditions
- People with a history of sexually transmitted diseases
- Those who have received blood or blood products
Stacey has had several sexual partners and does not always practice safe sex. She has had four sexual partners in the last six months. Stacey makes sure to let her doctor know this information. The blood work has resulted, and Stacey is positive for hepatitis B. It seems that Stacey contracted it through having unprotected sex with a partner with hepatitis B.
Treatment for hepatitis B depends on how long a person has had the virus, if there are symptoms, and if it is a chronic infection. Acute hepatitis B with minimal or no symptoms is treated at home with eating a balanced diet, drinking fluids, resting, and avoiding drugs and alcohol. If a person is experiencing severe symptoms, an antiviral medication may be prescribed, but it is uncommon. Hepatitis B is considered acute if it lasts less than six months.

{kind=link}