Category: Uncategorized


Mediastinum
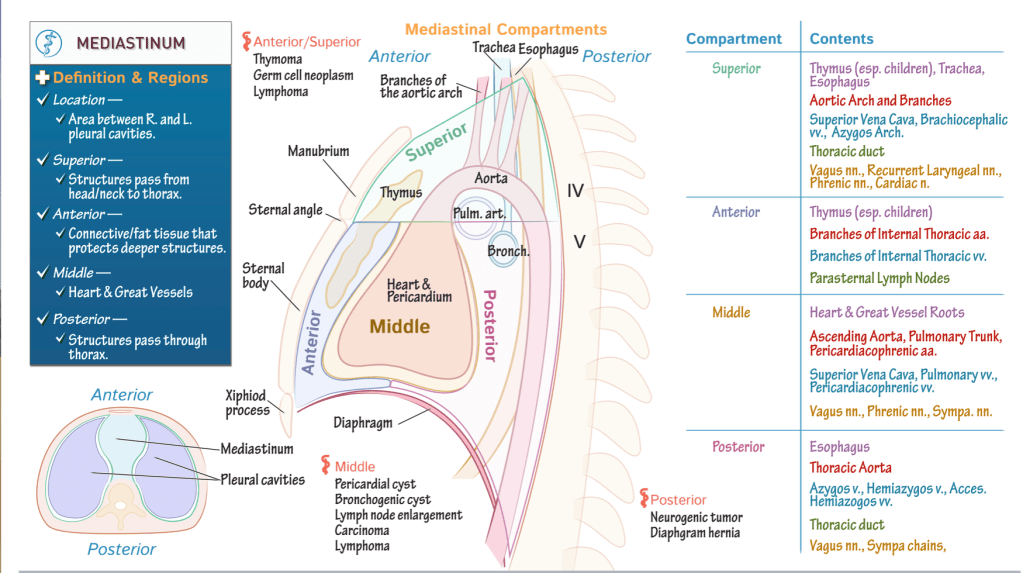
Middle compartment has a sac-like shape; it houses the pericardium, heart, and roots of the great vessels.
Anterior compartment lies anterior to this, and extends from the sternal angle, superiorly, to the diaphragm, inferiorly.
Posterior compartment lies posterior to the middle mediastinum, and, like the anterior mediastinum, extends from the sternal angle to the diaphragm.
Superior mediastinum fills the space between the superior thoracic opening to the sternal angle.
Key anatomical structures
- The thymus lies within the superior and anterior regions; recall that this structure regresses after childhood.
- Then, return to where the root and ascending portion of the aorta arise in the middle mediastinum, and show that the aorta continues through the superior and posterior compartments. We’ve also shown the branches of the aortic arch as they extend through the superior mediastinum.
- Next, posterior to the heart, show the opening of the left pulmonary artery as it passes to the left lung;
- The opening of the left bronchus; indicate that the trachea extends through the superior and posterior compartments of the mediastinum.
- The esophagus also passes through these compartments.
Pathology
- Let’s indicate some key masses that can develop in the mediastinum; we’ll broadly categorize these by region of the mediastinum, but beware of overlap.
- Anterior/superior mediastinum: thymoma, germ cell neoplasm, and lymphoma.
- Middle mediastinum: pericardial cysts, bronchogenic cysts, lymph node enlargement, carcinoma, and lymphoma.
- Posterior compartment: watch for neurogenic tumors and diaphragmatic hernias.
Summary Table
Superior compartment:
- Thymus, esophagus, and trachea.
- The aortic arch and its branches.
- The superior vena cava, brachiocephalic veins, and the arch of the azygos vein.
- The thoracic duct.
- The vagus nerves, recurrent laryngeal nerves, phrenic nerves, and cardiac nerve.
Anterior mediastinum:
- Thymus.
- Branches of the internal thoracic arteries and veins, and, the parasternal lymph nodes.
Middle mediastinum:
- The heart and the roots of the great vessels.
- The ascending aorta, pulmonary trunk, and pericardiacophrenic arteries.
- The superior vena cava, pulmonary veins, and pericardiacophrenic veins.
- And, the vagus nerves, phrenic nerves, and sympathetic nerves.
Posterior mediastinum:
- The esophagus.
- Thoracic aorta.
- Azygos, hemiazygos, and accessory hemiazygos veins.
- The thoracic duct.
- The vagus nerves and sympathetic nerves.
Larynx
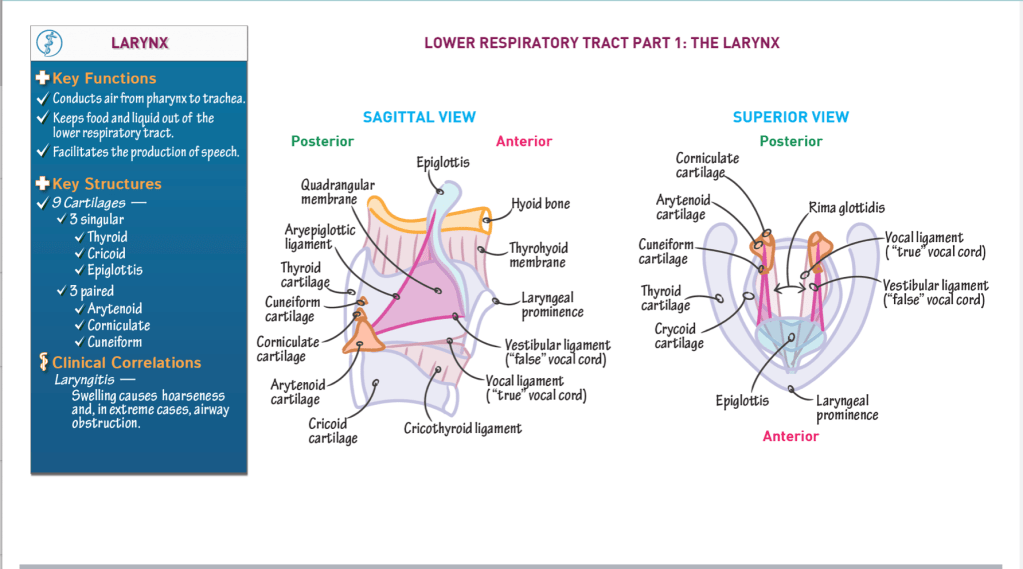
- The larynx is the start of the lower respiratory tract.
- Superiorly, the larynx is attached to the hyoid bone via connective tissues.
- Three key functions of the larynx:
- It conducts air from the pharynx to the trachea.
- It prevents food and liquid from entering the lower respiratory tract.
- It facilitates the production of speech.
Key anatomical structures:
Three larger, singular cartilages:
- Thyroid cartilage – forms anterior and lateral walls; features the laryngeal prominence.
- Cricoid cartilage – circular, forms base of larynx.
- Epiglottis – “flap” that attaches to the internal surface of the thyroid cartilage, anteriorly, and projects posteriorly and superiorly over the opening of the larynx.
- Upon swallowing, the flap closes off the entryway to the larynx, which prevents foods and liquids from entering the lower respiratory tract.
Three paired sets of smaller cartilages:
- Arytenoid cartilage – articulates with cricoid cartilage posteriorly.
- Corniculate cartilage – sits on arytenoid cartilages.
- Cuneiform cartilage – sits anterior to corniculate cartilages; very small, wedge-shaped.
Membranes and connective tissues:
- Thyrohyoid membrane – connects the thyroid cartilage and hyoid bone.
- Cricothyroid ligament – extends superiorly from the cricoid cartilage to the thyroid and arytenoid cartilages.
- Vocal ligament – thickened superior edge of the cricothyroid ligament comprises the vocal ligament; known as the “true” vocal cord because it facilitates sound production.
- Rima glottides – opening between the vocal cords. During sound production, laryngeal muscles contract to rotate the arytenoid cartilages and alter the opening between the true vocal cords.
- Quadrangular membrane – connects the lateral sides of the epiglottis to the arytenoid cartilages.
- Free edges of the quadrangular membrane thicken to form the:
Aryepiglottic ligament, superiorly
The vestibular ligament, inferiorly
- Free edges of the quadrangular membrane thicken to form the:
The vestibular ligament and its mucosal covering are often referred to as the “false vocal cord”; it does not participate in sound production.
Clinical correlations:
Laryngitis is inflammation of the vocal cords, which can stem from infectious or non-infectious causes (such as over-use). It typically results in hoarseness but severe swelling can block the airways.
Lungs and Pleural Membranes
LUNGS
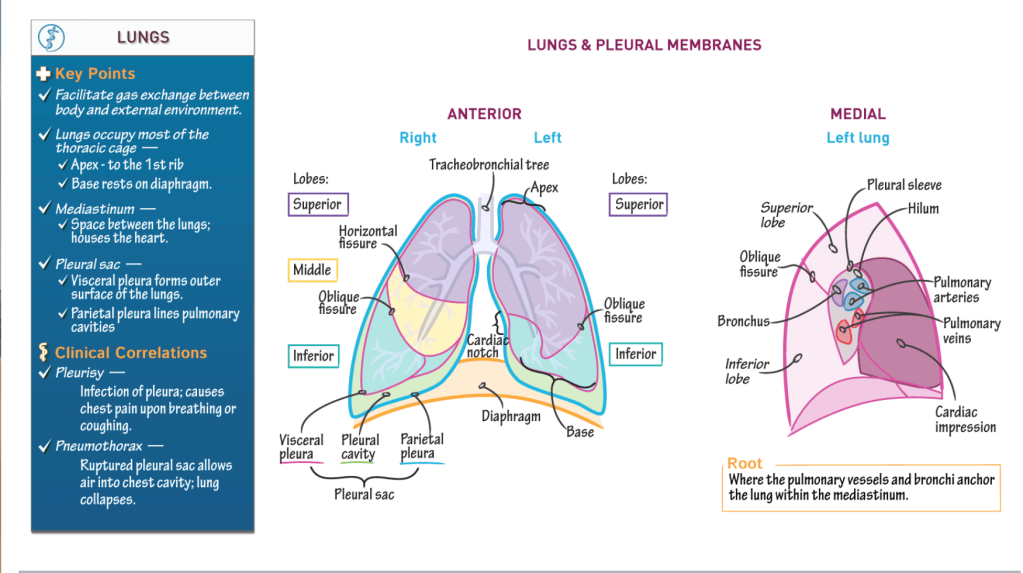
- The primary function of the lungs is to facilitate gas exchange between the body and the external environment.
- The lungs occupy most of the thoracic cage:
* The apex of the lung, its most superior portion, reaches the first rib. - The base of the lung, its inferior concavity, rests on the diaphragm.
- The mediastinum, which is the space between the lungs, houses the heart.
Right lung:
- 3 lobes (superior, middle, inferior)
- 2 fissures:
- HORIZONTAL fissure separates the superior and middle lobes.
- OBLIQUE fissure separates the middle and inferior lobes.
Left lung:
- 2 lobes (superior, inferior)
- 1 fissure:
- OBLIQUE fissure separates the middle and inferior lobes.
The left lung is smaller than the right because the heart lies slightly to the left within the thoracic cage.
Specifically, the heart nestles within the cardiac impression of the left lung, which is visible as the cardiac notch in anterior view.
Membranes:
The lungs are enclosed by the double-layered pleural sac:
- Visceral pleura forms the outermost layer of the lungs
- Parietal pleura lines the pulmonary cavities.
- Pleural cavity lies between the visceral and parietal pleura; it contains a small film of serous fluid that reduces friction between the layers.
Root of lung:
Pulmonary vessels and the bronchi anchor the lung within the mediastinum.
- Medial aspects of lungs.
- Hilum is obliquely shaped area, is lined by the pleural sleeve (aka, mesopneumonium).
Clinical Correlations:
- Pleurisy is infection of the pleura and causes chest pain upon breathing or coughing.
- Pneumothorax occurs when a ruptured pleural sac allows air to enter the thoracic cavity; the lungs collapse due to pressure changes.
Tracheobronchial tree
Key structures:
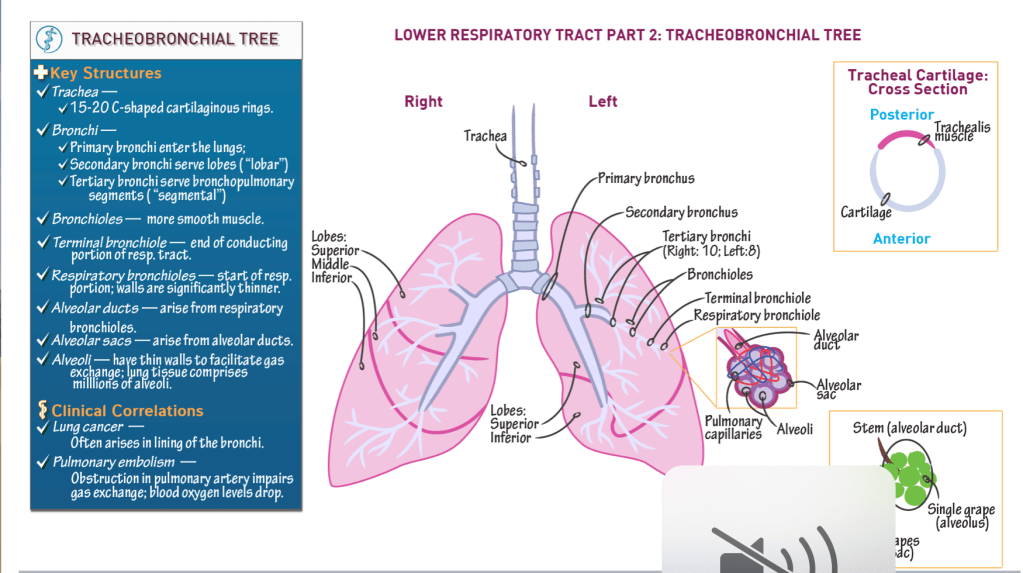
Trachea:
- Cartilaginous “trunk” of the tree.
- Comprises 15 – 20 C-shaped cartilaginous rings, are stacked vertically and connected via anular rings.
- Trachealis posterior forms posterior wall of trachea; moves to accommodate foods passing posteriorly through the esophagus.
Bronchi:
- Primary bronchi enter the lungs.
- Secondary bronchi serve lobes of lung (“lobar” bronchi).
- Tertiary bronchi serve bronchopulmonary segments (“segmental” bronchi); 10 on the right, 8-10 on the left.
Bronchioles:
- Numerous, and narrow as they branch.
- Have more smooth muscles in their walls, but still have cartilage in their walls.
- Terminal bronchiole is the final passageway of the conduction portion of the respiratory system.
Respiratory bronchioles:
- Demarcate the respiratory portion of the respiratory tract.
- Thin walls allow some gas exchange.
Alveolar ducts:
- Arise from respiratory bronchioles.
Alveolar sacs:
- Terminal ends of the alveolar ducts.
Alveoli:
- Thin-walled out-pockets of the alveolar sacs.
- Surrounded by pulmonary capillaries.
- Facilitate gas exchange between the respiratory and cardiovascular systems.
Lungs:
- Hundreds of millions of alveoli.
- Left lung = superior and inferior lobes; heart nestles into medial left lobe.
- Right lung = superior, middle, and inferior lobes.
Clinical Correlations:
Lung cancer often originates in the bronchi.
Pulmonary embolism (aka PE) obstructs arterial supply. In a PE, gas exchange is reduced, and blood oxygen levels drop.
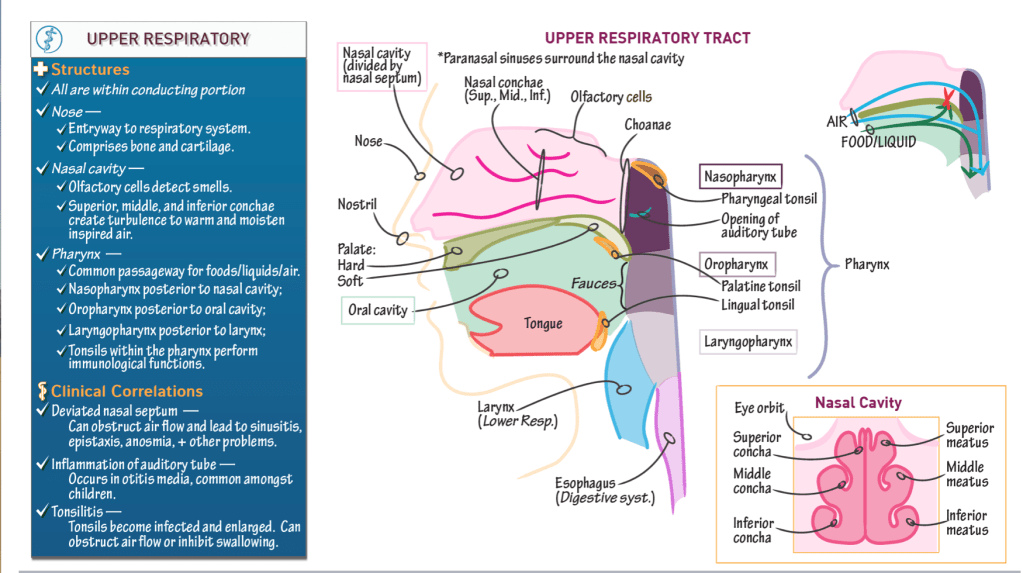
Upper Respiratory Tract
- Begins at the nose and ends with the pharynx.
Anatomical Structures
Nose:
- Opens the respiratory system to the external environment via the nostrils (aka, nares).
- Comprises bone and cartilage.
Nasal cavity:
- Posterior to the nose.
- Separated from the oral cavity by the hard and soft palates:
- The hard palate comprises the maxillary and palatine bones.
- The soft palate comprises soft tissues.
- Olfactory cells line the superior part of the nasal cavity
- The nasal septum divides the cavity into right and left sides.
- It comprises two vertical bony structures: the perpendicular plate of the ethmoid bone superiorly and the vomer, inferiorly.
- A deviated nasal septum can obstruct airflow and cause sinusitis (sinus infection), epistaxis (nose bleeds), anosmia (inability to smell), and other health problems.
- 3 nasal conchae: superior, middle, and inferior.
- Bony projections that arise on the lateral walls of the nasal cavity.
- The nasal conchae create meatuses (superior, middle, and inferior), which are small tunnels.
- Movement of air around the conchae and through the meatuses creates turbulence, which helps to warm and humidify the air. Hence, the conchae are sometimes referred to as the “turbinate” bones.
Paranasal sinuses
- Spaces within the bones surrounding the nasal cavity.
Pharynx:
- Descends posterior to the nasal cavity, oral cavity, and larynx, and is open to each of these structures.
- Common passageway foods/liquid and air: it serves both the respiratory and digestive systems.
- 3 subdivisions:
- Nasopharynx: posterior to the nasal cavity (and receives air from the nasal cavity).
The choanae are the openings between the nasal cavity and the nasopharynx.
Oropharynx: posterior to the oral cavity (and receives foods and liquids from the oral cavity).
The fauces is the opening between the oral cavity and the oropharynx. - Laryngopharynx: posterior to the larynx (it is the final common passageway for air and food/liquid).
- Nasopharynx: posterior to the nasal cavity (and receives air from the nasal cavity).
- The auditory tube (aka, Eustachian or pharyngotympanic tubes) opens into the nasopharynx
- Connects the ears and throat, which allows infection to pass between them.
- Auditory tube inflammation occurs in otitis media (aka, ear infection), which is common amongst children.
Tonsils
- Collections of lymphoid tissues that participate in immunological defense against bacterial and viral infections.
- 3 pairs of extrinsic tonsils:
- Pharyngeal tonsils reside in the superior wall of the nasopharynx.
- Palatine tonsils are near the palate (hence, their name).
- Lingual tonsils are at the back of the tongue (“lingual” refers to the tongue).
- As part of an aggressive immune response, the tonsils can swell and block airflow through the nose or inhibit swallowing.
- Chronic infection may necessitate tonsillectomy.

RAMSAY HUNT SYNDROME



Regards,
KRITI NAJA JAIN
Reference:-
- Medscape article:- https://emedicine.medscape.com/article/1166804-clinical
2. Shafers 8th e
3. Neville 3rd e
CENTRAL GIANT CELL GRANULOMA
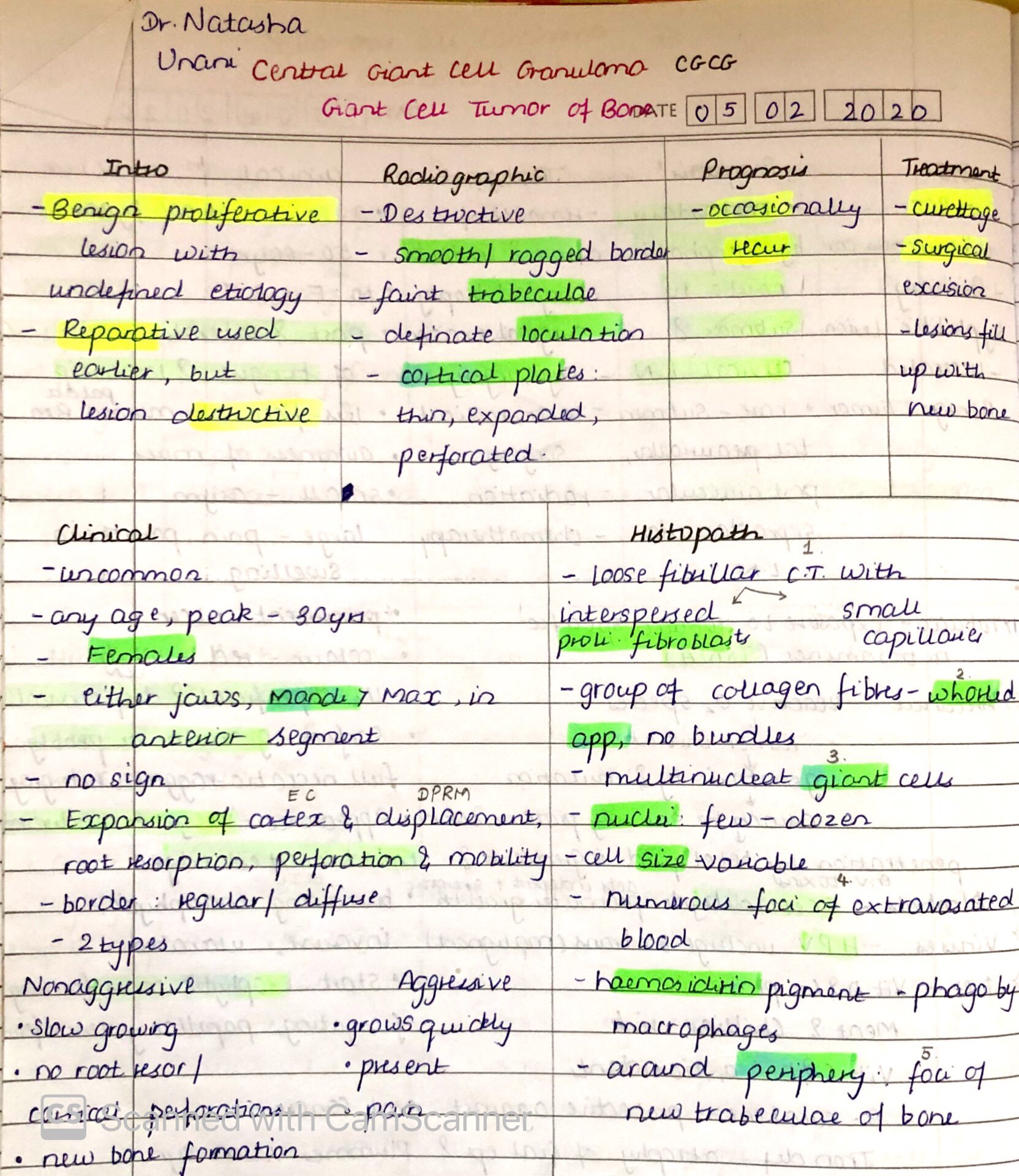
source – don’t remember, had written it long back. , textbook – Shafers
Addison’s disease
Steroids may have a less than perfect reputation in the media, but some steroids naturally occur in the body and function as a vital part of our endocrine system. For example, estrogens and testosterone serve important roles in human reproduction, while cortisol and aldosterone are integral in helping the body maintain equilibrium, especially in times of stress.
Addison’s disease is defined as the condition in which the steroid hormones produced by the adrenal cortex are either low or absent. It’s known by other names, too: chronic adrenal insufficiency, hypocortisolism, and hypoadrenalism, to name just a few.
Cortisol has many functions, including maintaining a consistent blood glucose level, reducing inflammation, and regulating water balance. Aldosterone primarily maintains sodium and water balance, which are necessary for keeping a consistent blood volume and pressure.
Both cortisol and aldosterone are produced by the adrenal glands, small endocrine glands that rest on top of both kidneys. The adrenal glands have two layers: the medulla, or inner, layer, and the cortex, the outer layer. In most cases of Addison’s disease, the cells that make up the adrenal cortex are destroyed. The destruction of these cells results in primary adrenal insufficiency, because cortisol and aldosterone are simply not produced. This is different from secondary insufficiency, in which either one or both hormones are made, but the body is unable to use them properly.
So, how does this fit into those other names for Addison’s disease? Since hypo means ‘low’ and the primary glucocorticoid is cortisol, a low amount of cortisol is ‘hypocortisolism.’ As you might guess, Addison’s is also characterized by hypoaldosteronism, low amounts of aldosterone. You’ll want to remember the roots hypo and its opposite hyper, which means high.
CAUSES
Let’s take a look at what happens to destroy the cells of the adrenal cortex. In about 80% of patients that have Addison’s, primary adrenal insufficiency is caused by an autoimmune response in which the body’s immune system mistakes its own cells or biochemicals for pathogens. Specifically, the body sees some part of a pathway used by the body for synthesis or use of cortisol and aldosterone as a threat and targets it for destruction.
Other things that cause primary adrenal insufficiency are:
- Adrenal dysgenesis, a genetic disorder in which the adrenal glands aren’t formed properly
- Difficulties in converting cholesterol to steroid hormones
- Infection from HIV or tuberculosis
- Other diseases that impair the adrenal cortex, like adrenoleukodystrophy and cancer
CLINCAL FEATURES
- Symptoms of Addison’s can also occur after a patient stops steroid use, especially if the medication taken has been taken for a long period of time or in high doses.
- Sustained use of medications like hydrocortisone and prednisone can desensitize the adrenal gland to the chemical that normally stimulates cortisol production, cause its cells to shrink, and impair its ability to make natural steroid hormones. This is called a iatrogenic response, an instance where treatment causes a disorder.
The symptoms of Addison’s disease are caused by the absence of aldosterone and cortisol. If you think about the functions of these two hormones, then it’s less difficult to determine the symptoms that arise when they’re not present. Here’s where ‘hyper’ and ‘hypo’ start to come into play.
Cortisol
- Keeps blood sugar levels in balance by stimulating the creation of glucose in the liver. Its absence means a drop in blood glucose, which, in turn, leads to fatigue and lethargy.
- Cortisol and aldosterone work together to maintain salt and water balance, so their loss leads to orthostatic hypotension, a sudden low blood pressure that occurs on standing.
Aldosterone
- Its absence also causes a drastic upset in electrolyte balance, leading to nausea, diarrhea, and vomiting. Together, these pose a real danger of causing dehydration, and, eventually, hypovolemia or low blood volume.
- Because electrolytes like sodium and potassium ions are crucial for nerve and muscle function, symptoms like heart arrhythmia and nervous system changes (especially in the form of mood disorders) are common, as is a craving for salt in an effort to replace the sodium being over-excreted in the urine.
Cushing Syndrome
Everyone knows that there’s too much of a good thing. Even a cool glass of lemonade on a hot summer’s day can turn into a sticky mess if the person pouring it isn’t paying attention. We need the hormone cortisol to help us deal with stressful situations. In Cushing’s syndrome, the body experiences the effects of too much cortisol for too long of a period of time. The result? Cortisol, which usually mediates the effects of stress, instead ends up causing damage to the body.
Cortisol is made by the adrenal glands, a pair of glands that rest on top of the kidneys. You can think of the steps of the cortisol pathway as a baseball player who runs the bases after hitting a home run. The pathway starts in the hypothalamus, the part of the brain responsible for much of the body’s ‘autopilot’ activity – things like breathing and heart rate. When the hypothalamus receives a stimulus that the body’s under stress, it releases corticotropin-releasing hormone (or CRH). This speeds to the pituitary, where it tells the master gland to release adrenocorticotropic-stimulating hormone (or ACTH). ACTH races to the adrenal glands to release cortisol. Cortisol then goes on to do things like increase blood sugar levels, lower inflammation, and raise blood pressure.
Before we dig into what causes Cushing’s syndrome, we should clarify the relationship between Cushing’s syndrome and Cushing’s disease. A syndrome is different from a disease, which is a specific disturbance in a part of the body. Cushing’s disease is just one cause of Cushing’s syndrome. In other words, not all cases of Cushing’s syndrome are caused by Cushing’s disease.
CAUSES
Most medical professionals divide these causes into two large categories.
The first is exogenous, meaning ‘generated from without.’
- Long-term use of corticosteroid medications can cause Cushing’s syndrome.
- Iatrogenic steroids often prescribed for inflammatory diseases like arthritis or given by injection for pain. Cushing’s syndrome may develop if the dosage of medication is or becomes larger than the body can handle.
The second large category is endogenous, meaning ‘generated from within.’ Endogenous cases of Cushing’s syndrome are usually caused by one of three things:
- The first is a pituitary adenoma, a benign tumor of the pituitary gland. An adenoma may secrete large amounts of ACTH in a way that the body can’t control. A large amount of ACTH will stimulate the adrenal gland to produce a large amount of cortisol. Here, finally, we have the specific cause of Cushing’s disease. Roughly 70% of endogenous cases of Cushing’s syndrome are caused by pituitary adenomas and therefore are classified as actual cases of Cushing’s disease.
- The second endogenous cause is called ectopic syndrome. You may recall that ‘ectopic’ means ‘in an abnormal place.’ Sometimes tumors of the lungs, pancreas, or thyroid release ACTH. Again, the body does not have the means to control this unplanned ACTH, and it stimulates the adrenal glands to produce too much cortisol.
- The third endogenous cause is primary adrenal disease. In these cases, a tumor of the adrenal gland (again, usually benign) goes rogue and secretes large amounts of cortisol.
Clinical Features
Common Findings:
- Weight gain/ lemon on sticks/ central obesity
- Increase in peripheral resistance = Hypertension
- Increase in blood sugar, FBS = more than 126 mg%
- Increase in cortisol levels causes insulin resistance, which increases sugar in the blood causing secondary DM
- Decrease in bone calcium causes osteoporosis, calcium is needed for muscle contraction.
- Cortisol effects on sex steroid receptors causing oligomenorrhoea, infertility, PCOD and hirsutism
More specific findings include:
- Moon facies
- Proximal myopathy
- Easy bruising
- Purple striae and Thin, fragile skin
- Fat deposition in the face
- Hypokalaemia and metabolic alkalosis are prominent, particularly with ectopic production of ACTH
Screening test
– measurement of 24-h urinary free cortisol
– late-night salivary cortisol measurement
– 1-mg overnight dexamethasone test
Investigation of choice
– low dose dexamethasone suppression test
– inadequate suppression of urinary cortisol [<10 μg/d (25 nmol/d)] or plasma cortisol [<5 μg/dL (140 nmol/L)] after 0.5 mg dexamethasone every 6 h for 48 h.
Biochemical testing
– Low levels of plasma ACTH levels suggest an adrenal adenoma or carcinoma
– Normal or high plasma ACTH levels suggest a pituitary or ectopic source
Imaging
– MRI of the pituitary
– Imaging of the chest and abdomen
Treatment
- Iatrogenic steroids- Taper steroids and Azathioprine
- Oar=T cell ca lung- cisplatin + Trinotecam
- Pituitary adenoma Cushing disease – transsphenoidal surgery
- Adrenal Adenoma – Medical Adrenolectomy
