
SOURCE – Nancy 13th edition
Category: Uncategorized
OROPHARYNGEAL AIRWAY

SOURCE – Nancy 13th edition
Joint Types
Two articulation classification systems
Functional and Structural
Functional classification
- Determined by the degree of movement permitted by the joint. An inverse relationship exists between joint mobility and stability.
The functional classification types are:
- Synarthrosis joints, which are immovable and stable.
- Amphiarthrosis joints, which are slightly moveable and slightly stable.
- Diarthrosis, which are freely moveable and very unstable.
Structural classification
- Determined by the joint’s connective tissue type and whether there is a cavity within the joint.
The structural classification types are:
- Fibrous joints, which are connected by fibrous connective tissue.
Three subtypes of fibrous joints:
Syndemosis (as between the bones of the forearm)
Suture (as between the bones of the skull)
Gomphosis (as between the teeth and the bones of the jaws) - Cartilaginous, which are connected via cartilage.
Two subtypes of cartilaginous joints:
Symphysis joints (joined via a fibrocartilage pad, as the two pubic bones)
Synchondrosis joints (joined by hyaline cartilage, as between the ribs and the sternum)
Synovial
- Comprises an articular cavity enclosed in a deep synovial membrane and a superficial fibrous membrane. The synovial and fibrous membranes comprise the articular capsule.
There are several subtypes of synovial joints: - Gliding joints occur where flat surfaces meet to allow sliding and twisting. The wrist bones, or carpals, are joined by gliding joints.
- Pivot joints form where a round projection fits inside a ring to allow rotation. The first and second cervical vertebrae articulate via a pivot joint.
- Condylar joints occur where one bone fits into an oval-shaped depression in another bone, such as where the radius cradles the carpals.
- Saddle joints occur when the saddle-shaped region of one bone articulates with a depression on another bone, such as where the carpal and first metacarpal (the thumb) meet.
- Ball-and-socket joints form where a ball-like process fits inside a cup-like depression, which allows maximum freedom of motion, such as between the head of the humerus and the glenoid cavity of the scapula.
Clinical Correlation:
- Synovitis is a painful inflammatory condition of the synovial membrane that commonly occurs in rheumatologic conditions such as rheumatoid arthritis, lupus, gout, or simply by overuse injury.
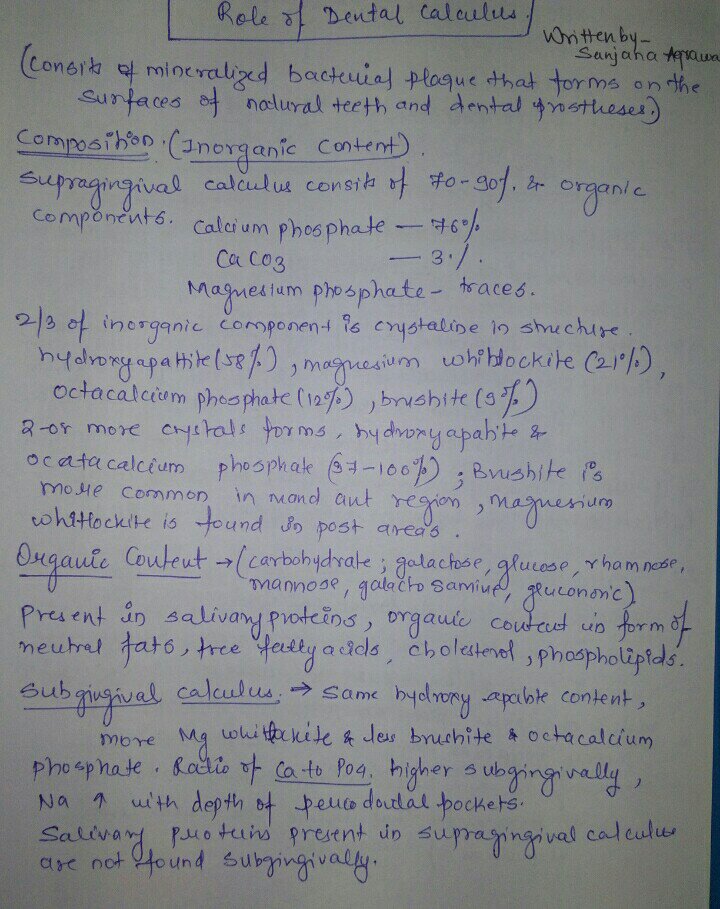
DENTAL CALCULUS

SOURCE – CARANZZA TEXTBOOK
Skeletal Muscle Contraction (Cross-Bridge Cycle)
KEY STEPS
- ATP binds myosin, which causes its release from actin.
- ATP hydrolysis causes the myosin head to rotate.
- High energy myosin binds ATP (forms the cross-bridge).
- Phosphate release initiates the power stroke.
MYOFIBRIL INTERNAL HISTOLOGY
Thick filaments
- Form from myosin
- The A band refers to the length of the thick filaments, “think “A” for d-a-rk – they are aniosotropic (or birefringent) in polarized light.
- H Zone is a zone of only thick filaments.
- M line bisects the A band.
Thin filaments
- Form from actin
- The I band is the region along the thin filaments (between the thick filaments).
- Think “I” for L-i-ght – they are “isotropic” (do not alter polarized light).
Z disks
- Transverse bands at the ends of the thin filaments.
Sarcomere
- The contractile unit of the myofibril.
- Comprises the area between the Z-disks.
- The thin filament slides towards the H zone.
- The (+) end attaches to the Z-disc sarcomere; the (-) end of the filament points toward the H zone.
Actin
- Spherical molecules joined in pairs of strands (like beads on a string). It is referred to as F-actin for filamentous actin, and comprises a polymer of G-actin monomers that are arranged in a double helix.
- There are myosin binding sites on actin and an ATPase site, an ATP-splitting site.
Tropomyosin
- Threadlike strands
Troponin
- Protein complexes that bind tropomyosin, actin, and also calcium (show their calcium-binding sites).
THICK FILAMENTS: DETAILS
- Comprise myosin molecules (technically myosin II), which form a golfclub shape, and comprise two heavy chains and two light chains.
- The head forms from the heavy chain and contains the actin-binding site.
The “cross-bridge” is the bond between actin and myosin.
THE HUXLEY SLIDING-FILAMENT MODEL
The rigor state.
- The myosin head is bound to the thin filament.
- Calcium is bound to troponin.
- Calcium binding to troponin allows myosin access to its binding site on actin.
ATP induces release of actin.
- Myosin has ATP bound to its head.
- The actin molecules are separated from (no longer bound to) the myosin.
- ATP is required to move out of the rigor state.
- If ATP is absent, which occurs after death, rigor will persist, called rigor mortis.
ATP is hydrolyzed to ADP and Inorganic phosphate (Pi).
- The myosin head rotates on the neck: it is now “cocked”: it’s in its high-energy state.
- The “cocked” state causes the thin and thick filaments to again bind via their cross-bridge.
- ADP and inorganic phosphate (Pi) are still bound to the myosin head.
Pi release initiates the power stroke for the myosin head to release its energy.
- Accordingly, the thin filament begins its slide.
The myosin returns to its uncocked, low energy state.
- At some point after the power stroke, ADP is released.
- Note that this is an area of intertextual variation, some authors instead write that ADP is released at the same time as phosphate to initiated the power stroke.
ATP GENERATION: 3 KEY MEANS
Direct phosphorylation:
- Creatine phosphate (a high-energy molecule stored in muscle cells) couples with ADP to make ATP and creatine.
- Creatine kinase catalyzes the reaction.
- As a corollary, creatine kinase is the best marker for muscle disease; it lies within muscle cells, for instance on the inner mitochondrial membrane, myofibrils, and sarcoplasm, and muscle injury releases it into the serum. Thus, muscle diseases are commonly associated with elevated creatine kinase levels.
Anaerobic glycolysis
- Nets 2 ATP molecules.
- Each glucose molecule is broken down into pyruvic acid molecules and ATP, but the pyruvic acid converts to lactic acid.
- Strenuous anaerobic exercise results in lactate build-up, which causes pain.
Aerobic respiration (which occurs in the presence of oxygen)
- Glucose is entirely broken down within the mitochondria to yield carbon dioxide, water, and large amounts of ATP.
- As a corollary, we see that in the presence of oxygen, cells can maximize ATP production.
Insulin and Glucagon
KEY PRINCIPLES:
- Insulin and glucagon are regulatory hormones that coordinate the storage and release of nutrients into the body
- Insulin, the “hormone of excess,” promotes the storage of glucose, fatty acids, and amino acids
- Glucagon, the “hormone of starvation,” promotes formation of glucose and fatty acids
KEY TERMS
- Glycogenolysis is the process by which glycogen is broken down to form glucose
- Gluconeogenesis is the process by which glucose is formed from non-carbohydrate substances (i.e., not glycogen)
- Glycogenesis is the formation of glycogen from glucose (so, the opposite of glycogenolysis)
- Glycolysis is the breakdown of glucose (which generates ATP, and is addressed in detail, elsewhere)
INSULIN
Actions
Insulin lowers blood glucose, amino acid, fatty acid, and potassium concentrations.
- Moves these substances out of the blood and into the cells.
- Promotes their storage and prohibits further synthesis.
- Glucose is stored as triglycerides and glycogen within adipose (fat) and skeletal muscle tissue.
- Within the liver, insulin prohibits glyconeogensis (glucose formation), and promotes glycolysis (glucose breakdown).
- Insulin increases the storage of fatty acids in adipose tissue, and inhibits lipolysis.
- Insulin promotes amino acid and protein uptake by skeletal muscle tissue and increases protein synthesis; it inhibits protein degradation.
- Insulin increases sodium-potassium pump activity, which increases cellular potassium uptake.
Clinical Correlation:
A consequence of insulin insufficiency (Type I diabetes) is hyperkalemia, because potassium shifts to the extracellular fluid. Hyperkalemia presents with weakness, chest pain, and difficulty breathing.
Insulin Release
- Stimulation of pancreatic beta cells release insulin, which then enters the hepatic portal system; recall that the hepatic portal system carries venous blood from the digestive organs.
- From the hepatic portal system, insulin is carried to the heart and enters the systemic circulation to be delivered to its target tissues, which, as we indicated above, primarily include the liver, adipose, and skeletal muscle tissue.
Stimuli for Release
In general, insulin is released after a meal.
- Increased blood glucose (most important), fatty acid, and amino acid concentrations
- Increased gastric secretion, particularly of incretins(i.e., GIP and GLP-1)
- Vagal stimulation
Inhibition of Release
- Low blood glucose concentration
- Increased fasting and/or exercise
- Catecholamines (norepinehrine and epinephrine),
- Somatostatin; recall that somatostatin is released from the delta cells of the pancreas.
GLUCAGON
Actions
- Raises blood glucose and fatty acid concentrations via stimulation of glucose and fatty acid mobilization in the liver.
- Promotes gluconeogenesis, glyconeogenesis, and glycogenolysis, which leads to increases in blood glucose concentrations.
- Increases lipolysis and decreases triglyceride storage, so that fatty acids are released into the blood stream.
Glucagon Release
- Pancreatic alpha cells release glucagon, which, like insulin, enters the hepatic portal system;
- Primary target tissue is the liver itself, which we saw in our previous diagram.
- Released between meals or upon ingestion of proteins.
Stimuli for Release
- Low blood glucose concentrations,
- Increased blood protein levels, and
- Increased gastric secretions, particularly of CCK (which, as you may recall, is itself released in response to protein ingestion).
- Catecholamines; this makes sense as part of the “fight or flight” response, a time when our tissues, particularly skeletal tissues, would need all available sources of fuel.
Inhibition of Release
- High levels of blood glucose and fatty acid concentrations
- Elevated levels of insulin
- Somatostatin
- Somatostatin inhibits both insulin and glucagon release; thus, these three pancreatic endocrine secretions co-ordinate to maintain homeostatic blood nutrient concentrations.
Endocrine Pancreas
PANCREATIC ENDOCRINE CELLS
- Comprise the Islets of Langerhans: each of which is a cluster of 4 endocrine cell types, whose products are ultimately secreted into the hepatic portal blood and delivered to the liver.
- A key function of pancreatic endocrine cells is to maintain basal blood glucose concentration via regulated storage and release: glucose is a major source of energy for the body.
- In order to maintain homeostatic blood glucose concentrations, the islet cells engage in communication via neural, hormonal, and cell-to-cell signaling.
Pancreatic endocrine cell types:
Alpha cells
- Comprise approximately 20% of the islet cells
- They secrete glucagon, which increases blood glucose concentrations between meals.
Beta cells
- Comprise approximately 65% of the islet cells
- They secrete insulin, which lowers blood glucose concentrations after a meal.
Delta cells
- Comprise approximately 10% of the islet cells
- Secrete somatostatin, which inhibits insulin and glucagon secretion to moderate their effects on blood glucose concentrations.
F cells
- Are rare
- They secrete pancreatic polypeptides, whose specific functions are uncertain.
Beta cell insulin secretion.
- Beta cells release insulin in response to multiple stimuli, but glucose is the primary stimulus.
Step 1:
- Glucose diffuses into the beta cell via GLUT – 2 receptors;
Step 2:
- Within the cell, glucose is phosphorylated by the enzyme glucokinase.
Step 3:
- Oxidation of phosphorylated glucose produces ATP.
Step 4:
- ATP closes potassium channels, trapping potassium inside the cell.
- This depolarizes the cell membrane.
Step 5:
- In response to depolarization, calcium channels open, and the intracellular calcium concentration increases.
Step 6:
- This triggers exocytosis of insulin-containing vesicles.
Bear in mind that the beta cell response to fatty acids and proteins is similar, though not identical.
As discussed in detail elsewhere, insulin is released into the nearby capillaries, drains into the hepatic portal system, and, eventually, enters systemic circulation to reach its target tissues.
Clinical Correlations:
Insulin-dependent, aka, Type I diabetes
- Destruction of beta cells (often by autoimmune disorders) causes insufficient circulating levels insulin; thus, carbohydrate, protein, and fat metabolism is inhibited.
- Because Type I diabetes is due to insulin insufficiency, insulin replacement therapy is the primary treatment to normalize blood nutrient concentrations.
Insulin-resistant, aka, Type II diabetes
- Down-regulation of insulin receptors on target tissues, specifically in the liver, skeletal, and adipose tissues, inhibits metabolism of carbohydrates, protein, and fat.
- Despite normal, or even elevated, levels of insulin, the target tissues cannot respond as usual; thus, treatment includes insulin receptor sensitizers (in addition to insulin therapy).
Parathyroid Glands
Hormonal regulation of extracellular calcium and phosphate concentrations by the parathyroid glands.
Key Principles
Free calcium participates in various cellular processes, including:
- Skeletal, cardiac, and smooth muscle contraction
- Nerve conduction
- Blood clotting
- Bone and tooth formation
- Enzyme activation and deactivation
Phosphate is a part of ATP
- Participates in cellular metabolism
- Plays a role in enzyme activation and deactivation
Storage and Release:
Calcium and phosphate are stored within hydroxyapatite crystals of bone
- When bone is resorbed, calcium and phosphate are released into the extracellular fluid
- Calcium and phosphate levels are regulated by the same hormones:
- Parathyroid hormone, which is secreted by chief cells of the parathyroid glands
- Vitamin D (in activated form)
(The physiologic role of calcitonin, a hormone released by the thyroid gland in response to increased calcium concentrations, is as of yet uncertain, and, therefore, omitted in this tutorial.)
PARATHYROID HORMONE PATHWAYS:
In response to lowered extracellular calcium concentration, the parathyroid glands secrete parathyroid hormone (PTH).
Bone:
- In bone, episodic, transient binding of parathyroid hormone causes an increase in new bone synthesis
- Prolonged exposure to parathyroid hormone promotes resorption of old bone, and, therefore, the release of calcium and phosphate into extracellular fluid
Clinical consequences of these dichotomous effects:
- Osteoporosis, which is characterized by loss of bone density, can be treated with intermittent PTH administration
- Continuous release of PTH in individuals with hyperPARAthyroidism causes excessive bone resorption
Kidneys:
- Increased calcium reabsorption in the distal convoluted tubule of the nephrons
- Decreased phosphate reabsorption in the proximal convoluted tubule, which leads to phosphaturia, an increase in phosphate in the urine
– This action is important because, otherwise, reabsorbed phosphate would complex with the reabsorbed calcium, which would negate its physiologic effects in the body.
PTH STIMULATES RENAL ACTIVATION OF VITAMIN D
Kidney
- Vitamin D acts increases renal reabsorption of both calcium and phosphate
Small Intestine
- Vitamin D increases calcium and phosphate reabsorption
Bones
- Vitamin D works with parathyroid hormone to facilitate skeletal remodeling, which requires both synthesis and resorption of bone.
Clinical correlation:
Vitamin D deficiency in children causes rickets, in which skeletal development is impaired, the bones are weak, and, consequently, growth is often stunted.
System-wide consequences of calcium imbalances:
Hypocalcemic individuals experience hyperreflexia, muscle twitching and cramping, numbness and tingling
- Trousseau’s sign, characterized by involuntary hand and feet spasms, carpopedal spasms, which can be provoked by the examiner by inflating a blood pressure cuff to cause prolonged brachial artery occlusion.
- The Chvostek sign, characterized by hyper excitable facial muscle twitching in response to tapping the facial nerve.
Hypercalcemic individuals experience hyporeflexia, muscle weakness, lethargy, and, polyuria.
Thyroid Gland
THYROID GLAND PRODUCTS
T3 (full name, triiodothyronine)
- T3 is more biologically active.
T4 (full name, thyroxine, aka, tetraiodonthyronine).
- The thyroid produces T4 in greater quantities; so, target tissues to need to use 5′ iodinase convert T4 to T3.
THYROID HORMONE SYNTHESIS
- Synthesis occurs both intra- and extracellularly.
Step 1:
- Thyroglobulin is synthesized in the follicular epithelial cell and transported to the lumen.
- Thyroglobulin is a tyrosine-rich protein.
Step 2:
- The “i-trap,” which is a sodium-iodine co-transporter, pulls iodiDe into the cell from the capillaries.
- Iodide is a trace element that does not occur naturally in the body, so it must be consumed in the diet.
Step 3:
- Oxidization of iodiDe to iodiNe by the enzyme thyroid peroxidase.
Step 4:
- Organification, also driven by thyroid peroxidase, to combine iodine with the tyrosine of luminal thyroglobulin;
- As a result of organification, two thyroid hormone precursors form and attach to thyrogobulin:
- MIT (full name, monoiodotyrosine)
- DIT (full name, diiodotyrosine)
Step 5:
- Thyroid peroxidase drives coupling reactions:
- Two DIT molecules combine to form T4.
- One DIT molecule combines with one molecule of MIT to form T3.
- Ultimately, some MIT and DIT will be “left over,” and remain bound to thyroglobulin with T3 and T4 in the colloid.
- Recall that, as we learned earlier, T4 is produced in larger quantities.
Step 6:
- Thyroglobulin, along with thyroid hormone and its precursors, are endocytosed to the follicular cell.
Step 7:
- Upon glandular stimulation, MIT and DIT are released from thyroglobulin; they remain within the cell to be recycled in the synthesis of new thyroglobulin.
- Though omitted for simplicity, MIT and DIT are deiodinated
- IoDide returns to the pool of iodide within the cell.
- Tyrosine molecules are recycled in the synthesis of new thyroglobulin molecules.
- T3 and T4 are delivered to the systemic circulation to reach their target tissues.
- Most T3 and T4 travels in the blood bound to thyroxine-binding globulin (a carrier protein); only free T3 and T4 are physiologically active.
Growth Hormone Physiology & Pathology
Overview
- Growth hormone, aka, somatotropin, (somatotrophin) is secreted by anterior pituitary cells called somatotrophs.
- Somatotrophs make up more than half of the anterior pituitary, and growth hormone is the most abundantly secreted anterior pituitary hormone.
- Growth hormone is responsible for growth of almost all tissues, whether directly or indirectly via insulin-like growth factor 1 (IGF-1).
- Growth hormone secretion is pulsatile, and is highest during sleep.
- Growth hormone levels vary throughout life; they begin to fall after adolescence.
- Negative feedback loops regulate growth hormone secretion.
Growth Hormone Physiology
- First, we draw the hypothalamus and pituitary gland.
- Neurosecretory cells originate in the arcuate nucleus of the hypothalamus, and their axons terminate on capillaries of the hypothalamic-pituitary portal system.
- Within the anterior pituitary, there are various collections of endocrine cells;
– We label the somatotrophs with an S, and show the nearby capillaries that deliver hormone products to the blood supply.
Growth Hormone Release
- The hypothalamus secretes growth hormone releasing hormone (GHRH) into the neurosecretory cells.
- When it reaches the anterior pituitary, GHRH stimulates somatotropin release of Growth Hormone (GH), which then travels in the blood to tissues throughout the body.
Growth Hormone Effects
- Growth effects: it increases cell growth, proliferation, and differentiation throughout the body.
- Direct effects on growth:
– Increases bone length and muscle mass (growth hormone promotes protein deposition). - Indirect effects on growth:
– Diabetogenic effects: growth hormone increases glycogen breakdown in the liver to increase blood glucose, which can be used as fuel by growing body tissues.
– Growth hormone also increases insulin-like growth factor 1release from the liver, which in turn promotes growth and differentiation of various tissues.
Be aware that IGF-1 is sometimes referred to as somatomedin-C
– Glucose-sparing effects: it increases lipolysis, and decreases glucose uptake by skeletal muscle and adipose tissue, which frees up energy for growth of tissues.
Growth Hormone Regulation
- Key regulators:
– At the hypothalamus:
Sleep, hypoglycemia, and stress trigger the release of growth hormone releasing hormone.
Age and obesity are associated with reduced GHRH release, and, via negative feedback loops, glucose, IGF-1, and growth hormone also reduce GHRH release.
– At the level of the anterior pituitary:
Release of growth hormone is inhibited by growth hormone inhibitory hormone (aka, somatostatin, which is released by the hypothalamus), and via negative feedback signals from IGF-1 and Growth hormone (notice that IGF-1 and growth hormone provide negative feedback at both the hypothalamus and the anterior pituitary).
- Additional factors that promote and inhibit growth hormone secretion:
– Stimulates Secretion:
Growth hormone releasing hormone
Decreased blood glucose
Decreased blood free fatty acids
Increased blood arginine (an amino acid)
Protein deficiency and starvation
Stress and excitement (including a variety of experiences, including exercise and trauma)
Testosterone and estrogen
Deep sleep
Ghrelin, which is a growth hormone secretagogue (GHS) that is produced mainly in the stomach.
– Inhibits Secretion:
Growth hormone inhibiting hormone (aka, somatostatin)
Increased blood glucose
Increased free fatty acids
Exogenous growth hormone
Insulin-like growth factor 1 (via negative feedback)
Aging
Obesity
Pause to recognize that low blood glucose, low levels of free fatty acids, and increased levels of amino acids in the blood stimulate growth hormone release, which ultimately reverses each of these states to maintain homeostasis.
Growth Hormone Pathologies
Growth Hormone Defects
Growth hormone deficiency
- Characterized by low levels of growth hormone and IGF-1
– If there is not enough growth hormone to trigger its production, IGF-1 will necessarily be low. - Isolated growth hormone deficiency is often due to defects in the GH1 gene, which is responsible for growth hormone production.
- In other cases, growth hormone deficiency is an aspect of general hypopituitarism, in which other anterior pituitary hormones are also low.
- Patients can be treated with recombinant human growth hormone.
Growth hormone insensitivity is characterized by normal or high levels of growth hormone, and low levels of IGF-1. - This is the result of growth hormone receptor defects
– May be hereditary, as in Laron Syndrome.
– May acquired as a result of malnutrition, liver disease, diabetes, growth hormone receptor antibodies, or other pathologies. - Patients can be treated with recombinant IGF-1.
- In Children:
– Linear growth is slow (sometimes called pituitary dwarfism). - Children often have delayed puberty, with small gonads and genitalia (micropenis).
- In Adults:
– Body composition changes, including reduced muscle and bone mass, and increased fat mass.
– Increased risk of cardiovascular disease (including left ventricular dysfunction and hypertension), and are more likely to develop insulin resistance.
– Additionally, reduced exercise capacity, lethargy, and depression contribute to a lower quality of life in these patients.
Growth Hormone Excess
- Excessive section of growth hormone leads to elevated growth hormone and IGF-1
– Be aware that prolactin is also often elevated. - In both children and adults, the most common cause of growth hormone hypersecretion is an adenoma in the anterior pituitary.
– Treatment often requires tumor removal. - In Children: Gigantism
– Growth hormone hypersecretion occurs prior to fusion of the epiphyseal plates.
– This causes accelerated linear growth, and children are taller than their age/sex-matched peers; delayed puberty is also likely. - In Adults: Acromegaly
– Growth hormone hypersecretion occurs after epiphyseal plate fusion.
– Thus, linear growth can’t occur, but bone deformation, soft tissue swelling, and enlargement of facial features, hands, and feet are common.
– Patients are more likely to experience sleep apnea, diabetes, cardiovascular disease, arthropathy, carpal tunnel, headaches and visual disturbances due to tissue swelling and metabolic changes.
