Category: Uncategorized



HISTOPATHOLOGY OF CONNECTIVE TISSUE TUMORS
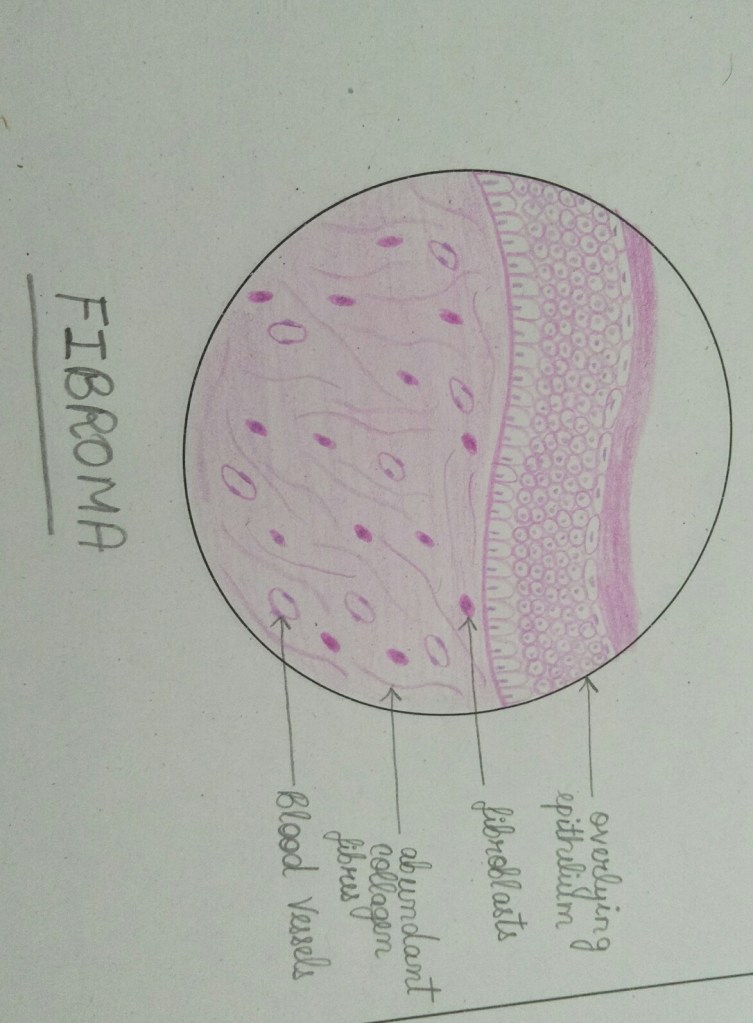
FIBROMA
- Overlying epithelium is of St.Squamous epithelium and is flat devoid of rete pegs.
- Connective tissue contains bundles of collagen fibres interspersed with many fibroblasts and blood vessels.
- Inflammatory cell infiltate present in cases of infection and trauma.
LIPOMA
- It is composed of mature adipocytes mixed with connective tissue septa.
- Adipocytes are round to oval with flat nuclei giving rise to “signet ring” appearance
- Thin fibrous capsule seen.
- Lipomas can be classified as classical lipoma and variants.
- Classical lupoma and fibrolipoma-most common
- Intramuscular and spindle cell variant- second most common.

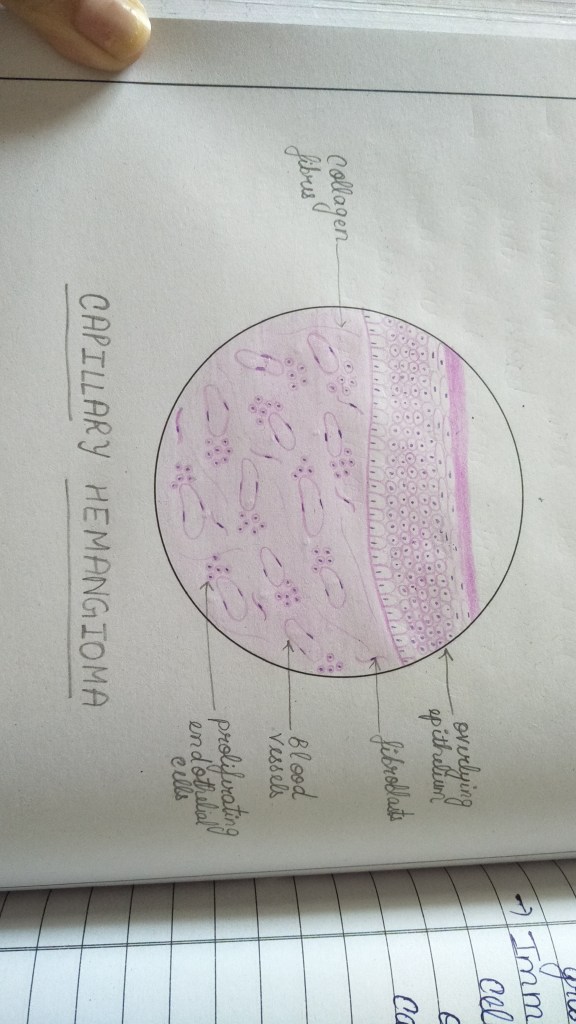
CAPILLARY HEMANGIOMA
- It contains minute,numerous endothelial lined capillaries.
- The endolial cell lining is single layered.
- Endothelial cells are flat,elongated or plump.
- Endothelial cells form aggregates or rosette around capillaries.
CAVERNOUS HEMANGIOMA
- It contains large dilated endothelial lined sinuses.
- These sinuses contain erythrocytes.
- Flattened endothelial cells and single layered.
- Fibrous conn tissue stroma
- Focal areas of haemorrhage and hemosiderin seen.

LYMPHANGIOMA
- It contains large dilated lymphatics with flat single layered endothelial cells.
- These lymphatics contain lymph.
- The lymphatics replace the connective tissue papillae.
- Cavernous type mostly seen.

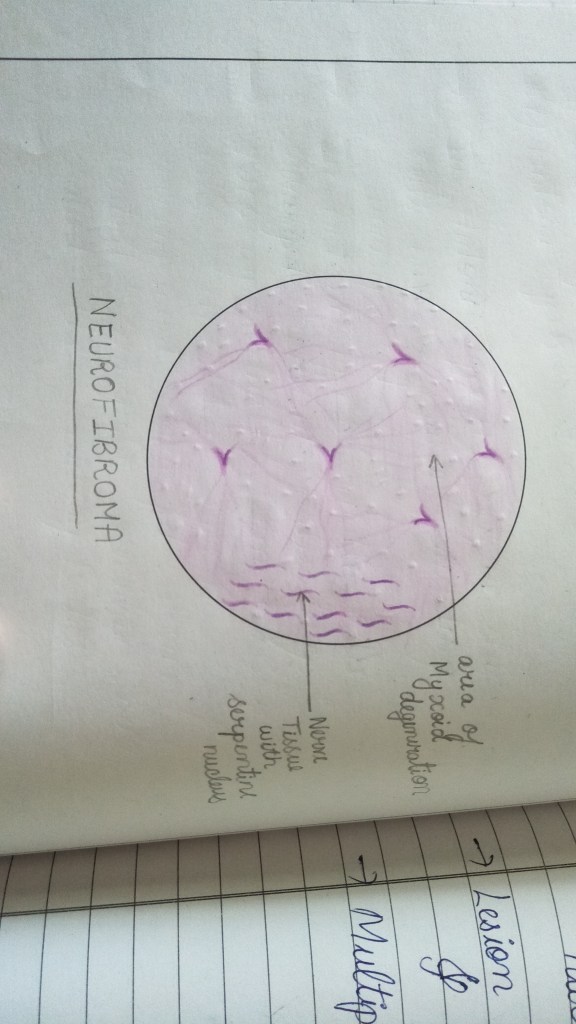
NEUROFIBROMA
- It contains wavy, elongated cels with dark staining nuclei in a collagenous stroma.
- Appears as “shredded carrot” like appearance.
- Cells arranged in fascicles or stripriform pattern.
- Connective tissue shows myxomatous area.
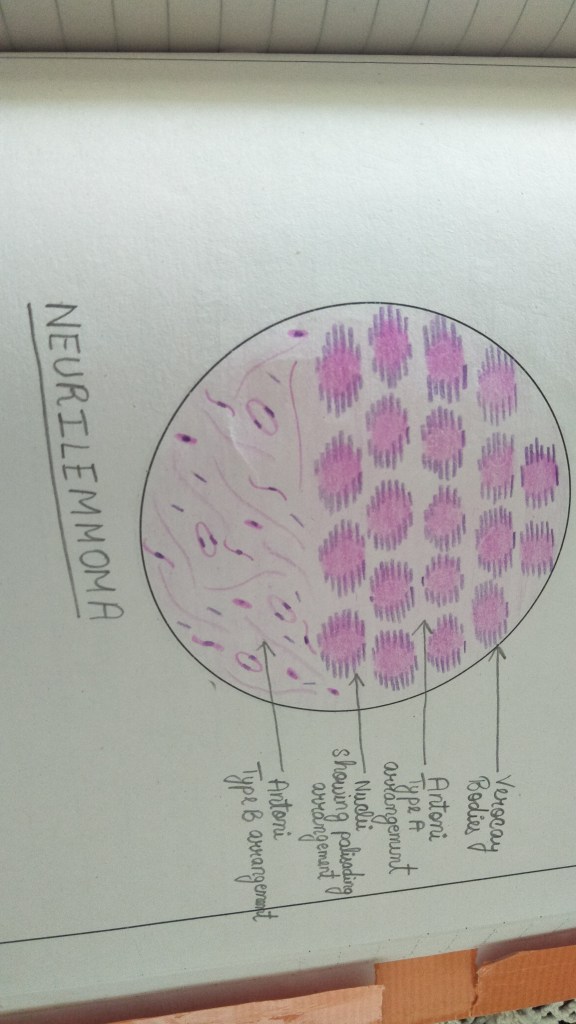
NEURILEMMOMA(SHWANNOMA)
- Tumor derived from shwann cells.
- Two types of arrangement seen.
- Antoni type A- made of cells with elongated or spindle shaped nucleus which are arranged parallel with their intacellular fibres arranged parallel between the rows of nuclei to form characteristic palisading pattern.
- The cells are around eosinophilic acellular area called Verocay bodies.
- Antoni type B- disorganized arrangement of cells and fibres. No palisading pattern.
OSTEOMA
- Maybe compact or cancellous.
- Compact osteoma made up of dense cortical bone with lamellar pattern.
- Both circumferential and interstitial lamellae seen arranged around a central haversian system.
- Osteocytes seen in lacunae.
- Cancellous osteoma made up of trabecular bone with osteocytes,osteoclasts and osteoblasts.


REFERENCES- Shafer’s textbook of oral pathology 9th edition
Myths and facts about dentistry

We often come across few advices which are actually misconceptions among people. Let us see what are those myths and find out the actual facts to spread right knowledge about dentistry.
Myth 1 : Brushing harder cleans better
Fact : absolutely not!! It’s a misapprehension that plaque can be removed by brushing harder. Applying too much pressure may slowly erode enamel, which cannot repair itself once it suffers significant damage. One may experience increased sensitivity and a heightened risk of cavities due to such activity. Brushing too hard can cause the gum tissue to shrink back (gum recession). So brush in a soft and right way.

Myth 2 : White teeth are healthy teeth
Fact : one can have pearly white teeth and still have gum infections or cavities. Likewise one can have perfectly healthy teeth which are off white, yellowish or even brownish. Enamel is on the surface of every tooth and it has a natural hue of white. However, the underlying dentin layer has a slightly yellowish colour. This yellowish hue shows through the enamel in almost everyone.

Myth 3 : If one has no oral health concerns, there’s no need for an exam.
Fact : definitely not!! Here are six reasons as to why one must visit a dentist once in every six months.
Reason 1 : oral cancer is an extremely serious disease that manifests itself in various ways. Without knowing the signs of its early onset, oral cancer is often not diagnoses and can quickly progress and can become life threatening. Dentist is highly trained to recognise these signs and with regular checkup the likelihood of catching oral cancer in time is dramatically high.
Reason 2 : Even with the most diligent tooth brushes and flosses, there are small areas in the mouth that are missed by a regular brushing and flossing. Regular dental cleaning remove tartar from eroding teeth or cleaning holes in them, which is how cavities are created.
Reason 3 : Regular dental cleanings are essential in catching and addressing gingivitis before it gets out of hand. “Better to hold a tooth in mouth rather than replacing the lost ones by a veneer or implant”.
Reason 4 : There are many bad habits that can have a negative impact on our oral health, some of which one may not even realize are causing issues. Some of them include chewing ice, biting nails, clenching jaw, grinding teeth, eating particularly sticky or hard sweets, brushing too hard, drinking cofee and red wine and ofcourse smoking. A regular checkup can help in can identify oral damages caused by these which one may have not noticed.
Reason 5 : A crucial part of visiting dentist is getting one’s teeth and jaw bone x-rayed. X-ray images allow dental professionals to see what is happening beneath the surfaces of your mouth and can find, diagnose issues that may be invisible to naked eye. Like impacted tooth, bone decay, swelling, cysts or tumours.
Reason 6 : In addition to checking mouth, gums and tongue for signs of oral cancer, dentist will also check one’s neck, jaw and lymph nodes located just below jaw line for any swellings or lumps or other abnormalities.

Myth 4 : Teeth cleaning / scaling and polishing will abradd the enamel and cause sensitivity issues.
Fact : Cleaning safely remove the plaque and bacteria that builds up over time on the teeth and gums. They don’t damage enamel on the teeth. Infacf, if teeth are not cleaned regularly, inflammation can occur and this can lead to gum disease sue ro the bacteria residing in the plaques.

Myth 5 : Braces are only meant for the younger.
Fact : getting braces may be a little easier or go a little faster during adolescence but adults from all walks of life should know that age is just a number when it comes to receiving and benefiting from orthodontic treatment. Adults count for 20% of orthodontic patients according to AAO statistics. Although harder bone rissue can mean a longer, more involved treatment process for adults with braces, the right orthodontic treatment plan is usually all it takes to straighten teeth, improve bite alignment, make oral hygiene easier and create a perfect smile at any age.

Myth 6 : There is no need to wear retainers after orthodontic treatment.
Fact : oh yes!! You need to wear those retainers given by your dentists for atleast 9 months and then dropping down to nightly wear after that. Going a year without retainer means that your teeth will have continued to move back to their original position and may even be crooked. The solution may be to restart treatment with braces. Isn’t it better to have retainers in their place rather than spending again on braces?!!

Myth 7 : Dental treatment costs a fortune.
Fact : the only reason one has ro spend so much on a dental treatment is because he/she didn’t take care of their teeth as much as they should have. Neglect, or rathee, result of neglect is always costlier than the the routine dental appointment that pops up in one’s calender twice a year. Moreover, the dental equipment are costlier too because of which a normal dentist demands more which is actually normal compared to what he invests.
Myth 8 : A fast prosthodontist is a good prosthodontist.
Fact : you are mistaken. Fast is not always good. A prosthodontist offers specialized treatment that cannot be rushed. It’s important that they take their time to make sure the job is done right the first time. While dentists may want to keep their patients moving, a prosthodontist takes his time and does what is best for the patient.
Myth 9 : I’m better off with my natural teeth or no teeth.
Fact : ofcourse natural teeth are always preferable. However, if one has lost one or few teeth to injury, disease or decay, a dental implant is truly the next best thing. The tooth that opposes the site of missing tooth may start to grow out from its position because it no longer has the opposing tooth to resist it. One may experience increased sensitivity and other issues around this super-erupted tooth.

References : 123dentist.com, reeseortho.com
FLOSS IT THE RIGHT WAY

Flossing is an integral part of our daily oral hygiene routine. It helps in removing food particles from the areas where toothbrush cannot reach, such as the gum line between the teeth. If food particles and bacteria accumulate in such areas, it eventually leads to gum problems and early gum recession.
Majority of the people brush their teeth regularly but they don’t floss them. To prevent plaque accumulation over the teeth and it between them, it is important to follow a proper flossing technique.
As per the ADA recommendations, the correct steps to be followed while flossing are as follows-
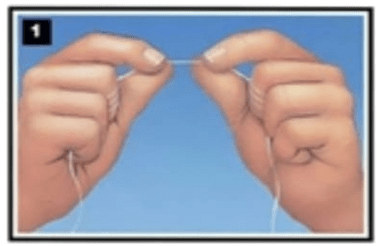
- Break off 18-24 inches of dental floss from the pack.
- To hold the floss correctly, wind most of the floss on your middle fingers, leaving only 1-2 inches of floss for your teeth.
- Position the floss between your two teeth and move it up and down, making sure that it touches the sides of both the teeth. Make sure not to move it towards the gums as it may cause trauma to the gums.
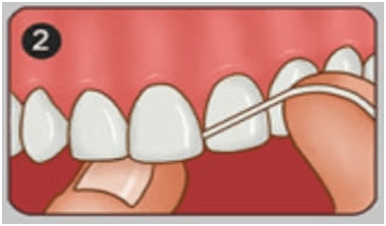
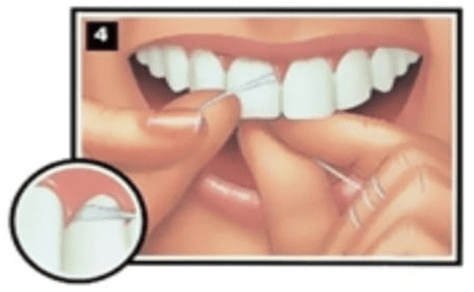
- As the floss reaches the gums, bend it over the tooth to form a C- curve so that the floss it now able to access the space between the tooth and the gums. Move the floss back and forth to thoroughly clean this area.
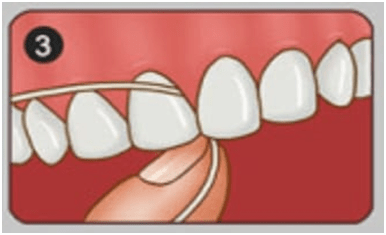
- Bend the floss towards the front and back surface of the tooth to clean both the surfaces. Use your thumb to direct the floss between the upper anterior teeth.
- Gently remove the floss from between the teeth and proceed to the other teeth, making sure to use the clean section of the floss while switching from one tooth to another. Make sure to snap while removing the floss to prevent any injury to the tooth and the gums.
It is recommended that you floss first before brushing your teeth, as flossing loosens the debris and bacteria between the teeth, which can then be easily removed by brushing.
Take about 10-15 minutes daily to floss your teeth, for a healthy and naturally white smile.
DR. DEVYANI ALLEN
BDS, FRCD
CHOOSING THE RIGHT TOOTHBRUSH
Toothbrushing comprises the most important part of our daily oral hygiene regime. Thus, it becomes very important for us to choose a toothbrush which is comfortable to use as well as functionally efficient.
Nowadays, the market is flooded with different types of brushes, be it manual or electric. This evolvement in the variety of toothbrushes has made it difficult for us to decide upon which toothbrush is best for us.
Here are few practical tips which can help you make the correct choice for your healthy whites-
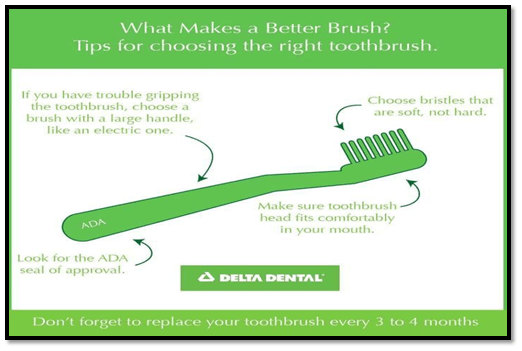
- The brush you choose should have soft bristles as hard-bristled brushes can cause your gums to recede. This can further cause increased dental sensitivity issues.
- A small headed brush is more beneficial as it can easily fit in your mouth can access at least 2 teeth at a time (ADA recommendation 1’’ long and 0.5’’ wide)
- The filaments of the brush should be round-ended to prevent any trauma to the gums.
- A compact, angled arrangement of short and long filaments to access the interdental areas and sulcus.
- A comfortable handle, preferably the one with indentations to prevent slippage from the hand while brushing.
Irrespective of the brush you choose, it is important that you follow the correct brushing technique and brush for atleast 2 minutes to increase the lifespan of your whites.
If you are using a manual brush, it is important to replace it once every 3 months or whenever the brush shows any signs of wear and tear.
So, next time when you are in the supermarket checking out the vast variety of brushes, try to look out for these few things in your brush and you will be able to make the correct choice.
DR. DEVYANI ALLEN
BDS, FRCD
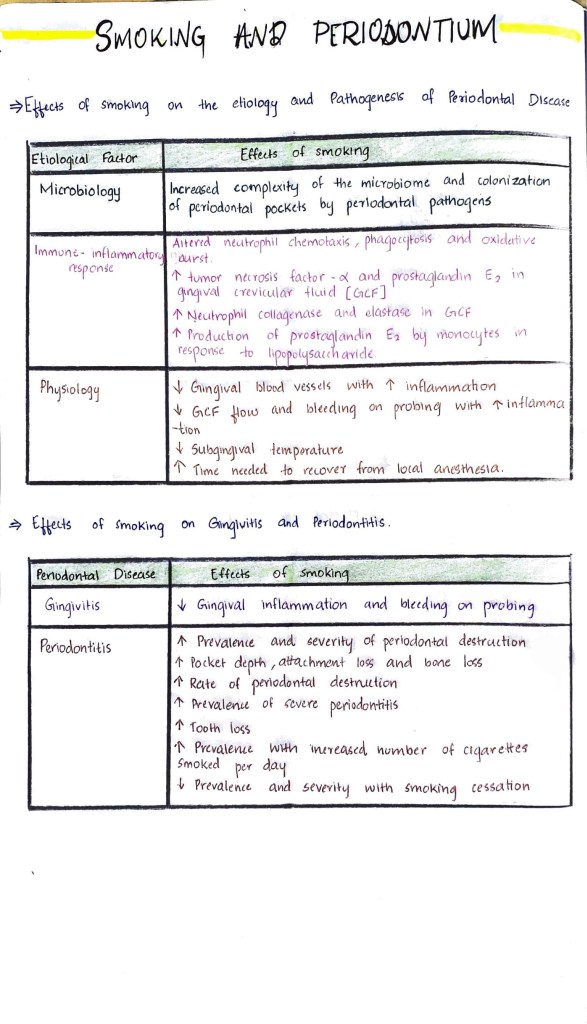
Smoking And Periodontium

CLINICAL EXAMINATION OF DENTIN HYPERSENSITIVITY

- Evidence of dentin exposure (gingival recession, loss of enamel)
- Sensitivity or pain on tactile examination of suspected teeth
- Evaporative stimulus: Suspected tooth is isolated using cotton rolls. If a momentary blast of air from air/water syringe causes sensitivity. It can confirm DH
- percussion sensitivity
- Pain lingering after the stimulus is removed
- Vitality tests to rule out pulpal involvement
- Radiographic examination to check for caries, pulpal or periodontal involvement
- Signs of fractured, leaky or poor restorative margins.
Reference: Clinical operative dentistry-principles and practice : Ramya Raghu, Raghu Srinivasan
DENTAL PLAQUE

Plaque is a sticky film of bacteria that constantly forms on teeth. Bacteria in plaque produce acids after you eat or drink.These acids can destroy tooth enamel and cause cavities and gingivitis
Untreated plaque can harden into (tough to remove ) tartar. Proper oral hygiene, including daily brushing and flossing gets rid of plaque

SYMPTOMS AND CAUSES
● plaque forms when bacteria present in mouth mixes with sugary or starchy foods such as milk, juice, bread ,pasta and soft drinks. These bacteria release acids that breakdown carbohydrates in food and drinks.
● Symptoms : A fuzzy feeling on teeth is the top sign of plaque. Other indicators include halitosis( bad breath ) and red , swollen , tender gums that bleed after brushing.
COMPLICATIONS
Plaque and tartar can lead to
• Cavities
• Gingivitis and periodontal disease
• Tooth decay and loss
• Tooth infection ( Abcessed tooth)
DIAGNOSIS
Since plaque can cause cavities, dental X rays to check cavities. Dental hygienest uses instruments during regular checkups to find and remove plaque
MANAGEMENT AND TREATMENT
Good oral hygiene includes regular brushing and flossing, removes plaque and prevents tartar buildup.
● Fluoride treatments : to slow the growth of plaque causing bacteria and stop tooth decay
● Chlorhexidine Mouthwash
● Dry mouth medication : to increase saliva production
PREVENTION
Plaque can be prevented by :
● Floss daily: Floss once a day with dental Floss or water flosser to get rid of food and plaque stuck between teeth. Studies shows that flossing before brushing teeth removes more plaque
● Brush twice a day: brush for 2 minutes with soft bristled toothbrush and fluoride toothpaste
● Use mouthwash : rinse with an over the counter or prescription antiseptic mouth wash
● Choose healthy food: Cut down sugary, starchy foods and drinks
Source: healthline.com
Ortho Case 2.18
13 year old patient presents complaining of the appearance of his teeth, in terms of UR1.
The problem list:
• Discoloured, ankylosed UR1
• Mild skeletal class III pattern
• Increased vertical proportions
• Mild crowding in the upper and lower arches
• Evidence of dento-alveolar compensation in the lower arch, with a retroclined lower labial segment
What is the long-term prognosis for the UR1? How will this affect the management of this patient’s malocclusion? What changes in the patient’s malocclusion may occur with future growth? Whilst monitoring the patient’s developing malocclusion, how would you manage the ankylosed tooth?
Link: https://drive.google.com/file/d/1oRT2nA2n3Oh3qVjy85bML6drS7Yskxv2/view?usp=drivesdk


Mnemonic on precancerous conditions

