
source – don’t remember, had written it a lot time ago
Category: Physiology
RESPIRATORY FAILURE

source – don’t remember, had written it a lot time ago
MOA OF LOCAL ANAESTHESIA

source – don’t remember, had written it a lot time ago
DIFFERENCE BETWEEN CARDIOVERSION AND DEFIBRILLATION

SOURCE – Nancy Carolina 13th edition
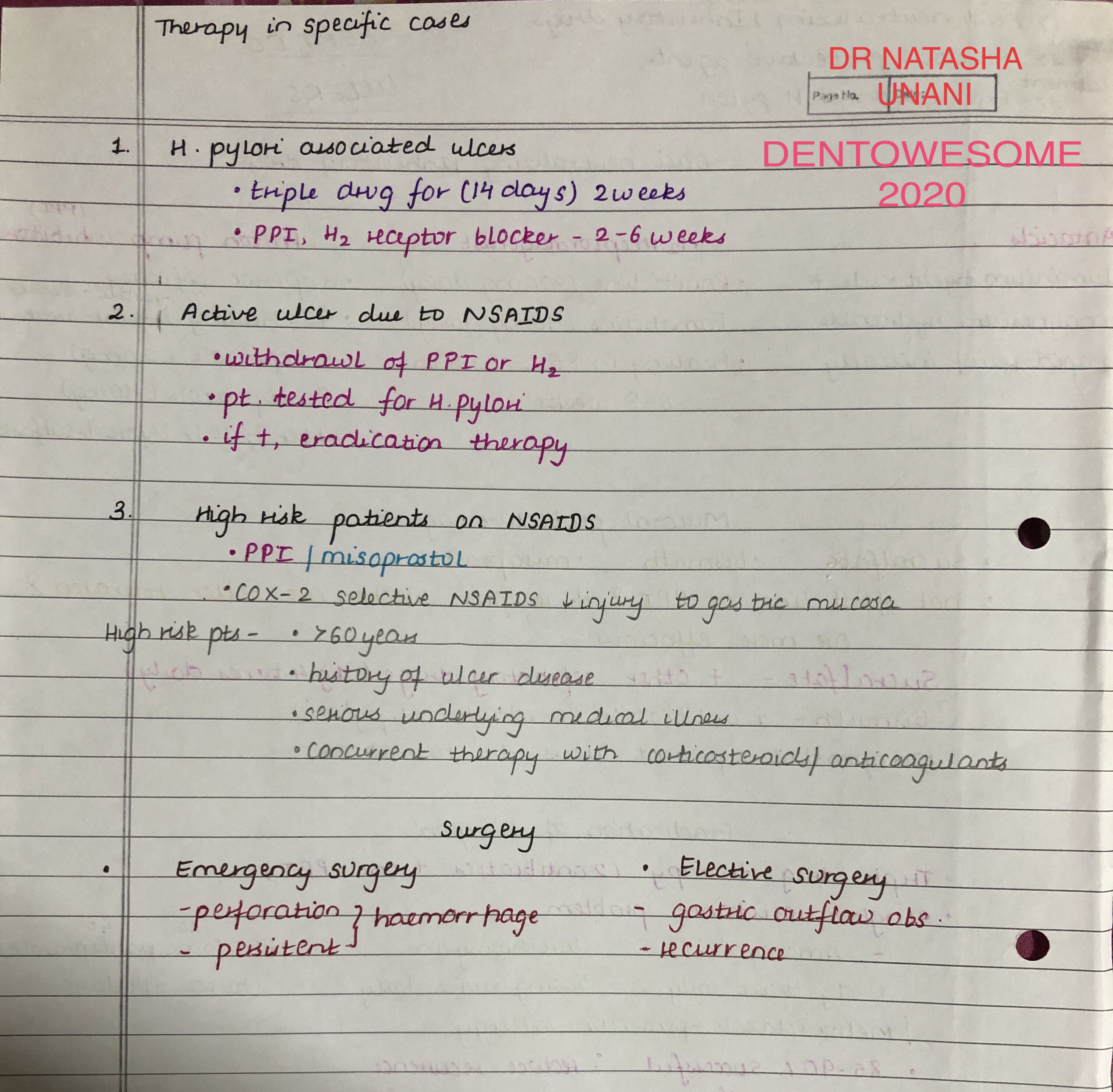
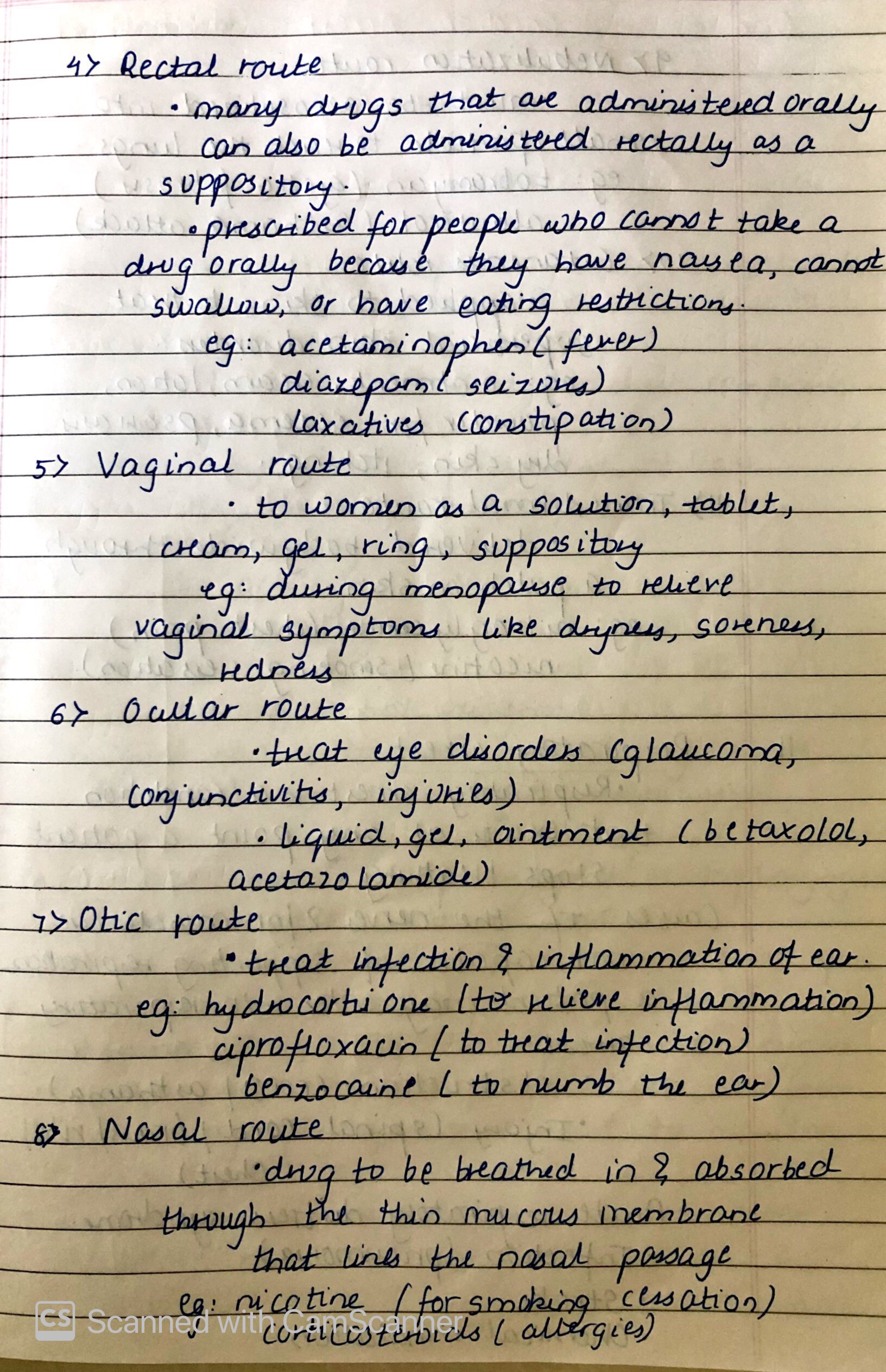
ROUTES OF DRUG ADMINISTRATION



SOURCE – Nancy Carolina 13th edition
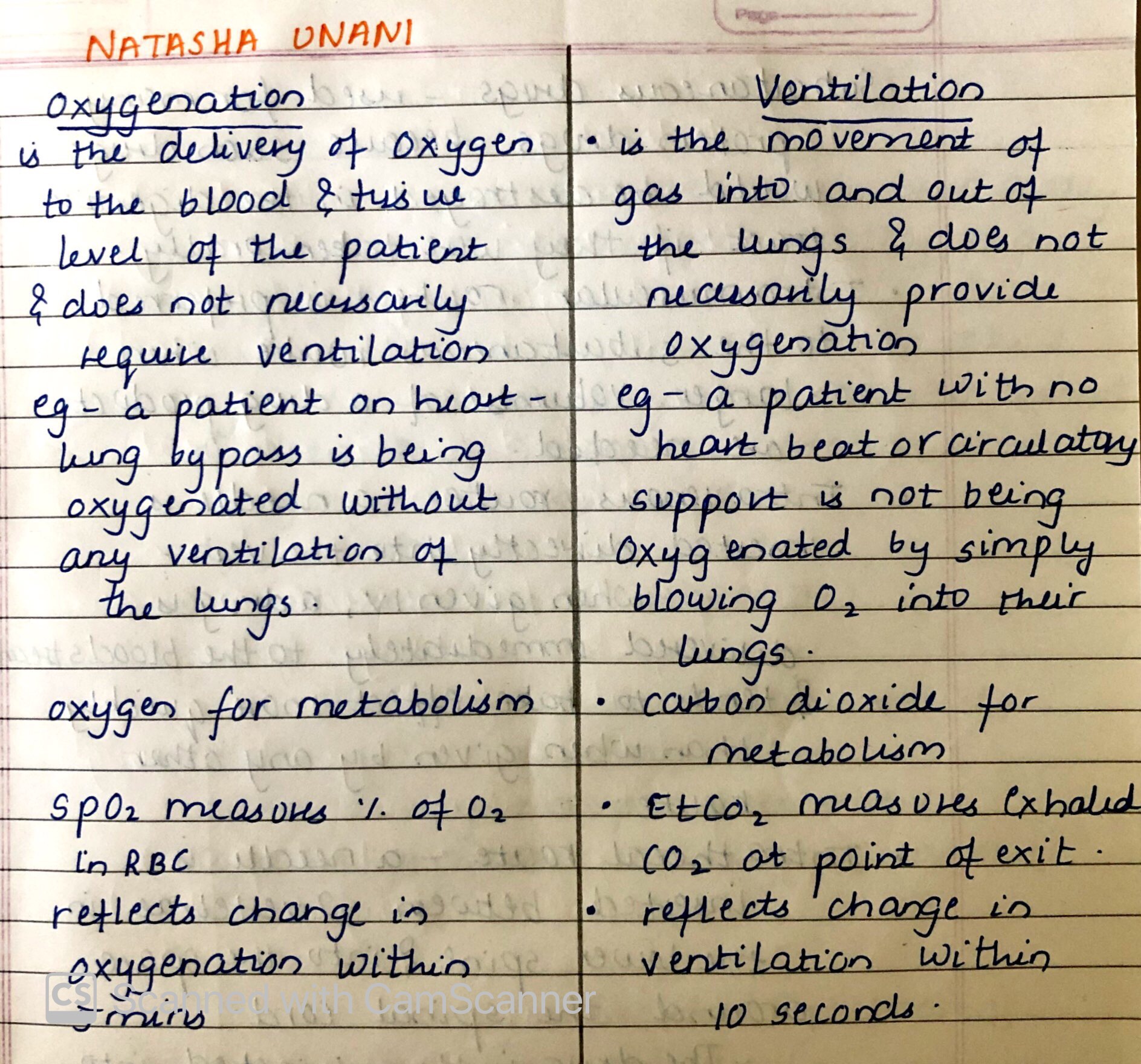
DIFFERENCE BETWEEN OXYGENATION AND VENTILATION
source – don’t remember had written it long back
Nausea and Vomitting
Nausea ,vomitting are common go to side effects of a drug, when external examiner asks during viva of a medical student. But, these symptoms can reveal many underlying conditions and diseases apart from the side effects of many drugs.
Nausea is imminent desire to vomit and often precedes or accompanies vomitting. vomiting is the forceful expulsion of the gastric contents through mouth.
PATHOPHYSIOLOGY:
1. Activation of the CTZ ,sends the impulses to the vomiting centre in brainstem,
2. Gastric fundus and gastroesophageal sphincter relaxes inturn cause raise in intra-abdominal pressure increase,due to increase in abdominal and diaphragm muscle contraction causes the gastric contents to enter the oesophagus ,
3. Increased intra-thoracic pressure results in further movement of food material to mouth
4.Reflex elevation of the soft palate and closure of glottis protect the nasopharynx and trachea and completes the vomiting
Causes of vomiting:
1. DRUGS:
-Cancer chemotherapy
-Antibiotics
-Cardiac antiarrhythmics
-Digoxin
-Oral hypoglycemics
-Oral contraceptives
2.Metabolic and endocrine causes:
-Pregnancy
-Uremia
-Ketoacidosis
-Thyroid and parathyroid disease.
-Adrenal insufficiency
3.Toxins:
-Liver failure
-Ethanol
4.Labyrinthine disease
- Motion sickness
- Labyrinthitis
- Malignancy
5. Bowel obstructing disorder
6. Cardiopulmonary disorders and cardiomyopathies
7.Enteric infections
-viral
-Bacterial
8.Inflammatory dieases.
- cholecystitis.
-Pancreatitis
-Appendicitis
-Hepatitis.
9.Intracerebral disorders
-Intracerebral disorders
-Malignancy
-Abscess
-Hydrocephalus
10. Post operative vomiting
11.Impaired motor functions.
Careful clinical examination, will reveal the underlying cause for nausea and vomiting, like ,vomiting that occurs predominantly in the morning is often seen in pregnancy, uremia, and alcoholic gastritis;projectile vomiting suggests increased intracranial pressure,vomiting during or shortly after a meal may be due to psychogenic causes or peptic ulcer disease.
complications, can be Rupture of the esophagus,hematemesis from a mucosal tear,dehydration, malnutrition, dental caries and erosions, metabolic alkalosis, hypokalemia, and aspiration pneumonitis.
Treatment is mainly based on the treatment of the underlying cause,
-Antihistamines such as meclizine and dimenhydrinate are effective
for nausea due to inner ear dysfunction
-Anticholinergics such as scopolamine are effective for nausea
associated with motion sickness
-Haloperidol and phenothiazine derivatives such as
prochlorperazine are often effective in controlling mild nausea
and vomiting, but sedation, hypotension, and parkinsonian
symptoms are common side effects.
-Metoclopramide may be superior to the phenothiazines in treating
severe nausea and vomiting.IV metoclopramide may be effective
as prophylaxis against nausea when given before chemotherapy.
-Ondansetron and granisetron, serotonin receptor blockers,
and glucocorticoids are used for treating nausea and vomiting
associated with cancer chemotherapy.
-Aprepitant, a neurokinin receptor blocker, is effective at
controlling nausea from highly emetic drugs like cisplatin
HEART FAILURE

SOURCE – Nancy 13th edition
Hindbrain Malformations (eg, Chiari Malformation)
THE MAJOR HINDBRAIN MALFORMATIONS
Chiari malformation
A syndrome of cerebellar herniation through the foramen magnum, which subdivides into three types: 1 through 3, from most mild to most severe.
CHIARI MALFORMATION
Type 1 Chiari Malformation
- Chiari malformation always involves downward displacement of the cerebellar tonsils through the foramen magnum but what determines its morbidity is the degree of cerebellar displacement, the degree of displacement of additional brainstem structures, and the associated pathologic involvement of other areas of the central nervous system.
- There is typically a normal ventricular system: 3rd ventricle and cerebral aqueduct, and 4th ventricle.
- There is an associated syringomyelia (a central cavitation of the spinal cord).
Syringomyelia (Cervical)
- The spinothalamic tract fibers cross at the ventral commissure.
- A fluid-filled cavity (a syrinx) expands outward from the central canal and disrupts the crossing fibers and ascending spinothalamic tracts.
- The clinical exam findings of a cervical syringomyelia include a suspended-sensory level wherein small fiber sensation is lost in a cape-like distribution in the arms and upper trunk but preserved in the legs, upper neck, and face.
- The location of the syrinx in the at the cervical level affects the cervical crossing fibers; hence the cape-like distribution.
- This upper limb distribution of deficit also occurs because the inner (arm) spinothalamic fibers lie more central than the outer white matter leg fibers (and, thus, are affected first).
Although the literature suggests that the association between syringomyelia and Chiari Type 1 malformation is quite common, frequent MRI imaging has taught us about the gross underestimation of the prevalence of more mild, asymptomatic Chiari Type 1 malformation cases.
Type 2 Chiari Malformation (aka Arnold-Chiari malformation)
- There is cerebellar tonsillar herniation and kinking below the foramen magnum.
- This kinking can block the output of CSF, which can cause hydrocephalus, which manifests with a dilated 3rd ventricle, cerebral aqueductal stenosis (narrowing) or atresia, and downward displacement of the 4th ventricle.
- The effect is to cause callosal dysgenesis (thinning) and enlargement of the diencephalon with often an absent septum pellucidum.
- Type 2 malformation is most often associated with a lumbar meningomyelocele (a protrusion of the spinal cord and meninges through a defect in the posterior vertebral column).
We can imagine that this tethering of the lumbar cord could serve as the nidus of the downward displacement of the posterior fossa structures by the tethering effect of the meningomyelocele but however logical this theory, it hasn’t been substantiated in the scientific literature.
Type 3 Chiari Malformation
The severest, rarest form.
- There is a high cervical and occipital encephalocele, which involves:
-Occipital lobe herniation
-Cerebellar herniation
-Spinal cord herniation
-Cystic dilatation of the 4th ventricle
-And squashing of the corpus callosum and diencephalon from the caudal dragging of the occipital and cerebellar herniations.
*DANDY-WALKER MALFORMATION*
Cerebellar agenesis and a grossly dilated 4th ventricle.
- Hydrocephalic 3rd ventricle
- Enlarged diencephalon
- Dysgenic corpus callosum (much like in the Chiari Type 2).
- Cerebellar agenesis and a grossly dilated 4th ventricle.
- Dandy Walker malformation involves cystic dilatation of the fourth ventricle, agenesis of the cerebellar vermis, and hydrocephalus with thinning or absence of the corpus callosum may be absent.
- Dandy Walker malformation may cause impaired motor development, macrocephaly (enlargement of the skull), and indicate that it can be associated with other syndromes such as Walker Warburg syndrome, which combines a Type 2 Lissencephaly with Dandy Walker malformation, or other syndromes involving cardiac, neural, and limb developmental anomalies.
Congenital Left to Right Shunts
HEALTHY HEART
Typically, post-natal systemic and pulmonary circulation run in parallel and maintain separation between low and high oxygen blood. When separation is incomplete, low and high oxygen blood mix, which produces systemic blood with insufficient oxygen concentrations.
The Great Vessels
- The aorta carries blood with a high oxygen concentration to the body tissues.
- The pulmonary trunk carries blood with a low oxygen concentration to the lungs.
- Ductus arteriosus
- Allows blood to flow from pulmonary trunk to aorta, bypassing the lungs.
- The ligamentum arteriosus is the adult remnant of the ductus arteriosus.
Left to right shunts
In conditions with left to right blood shunting, oxygenated blood recirculates through the lungs rather reaching the body tissues.
Ventricular septal defects
Characterized by an incomplete ventricular septum, which allows oxygenated blood to pass from the left ventricle to the right, which then returns it to the lungs.
Atrial septal defects
Allow oxygenated blood from the left atrium to pass into the right heart and, ultimately, back through the pulmonary circulation.
Patent ductus arteriosus
Typically, the ductus arteriosus regresses after birth and becomes the ligamentum arteriosus; however, in some cases, the channel persists.
- Low pulmonary vascular pressure allows oxygenated blood to “backflow” from the aorta into the pulmonary trunk, which then recirculates it through the lungs.
Eisenmenger syndrome
Occurs when an uncorrected congenital left to right shunt induces anatomical changes that reverse the shunt.
- A congenital left to right shunt increases pulmonary blood flow.
- Increased pulmonary blood flow work induces hypertrophy of the right ventricle.
- Hypertrophic right ventricle becomes so powerful that it eventually overwhelms the pressure from the left ventricle and sends deoxygenated blood directly into the left ventricle, causing hypoxemia.
