Arrest or prevention of bleeding by physiological process is called hemostasis
Factors :-
F1. Fibrinogen
F2. Prothombin
F3. Thromboplastin
F4. Calcium
F5. Labile
F6. Not known
F7. Stable
F8. Antihaemophillic
F9. Christmas
F10. Stuart
F11. Plasma thrombin antecedent
F12. Hegman
F13. Fibrin stabilizing
Mechanism :-
Injury vessel walls – Formation of clot – Seal off damage blood vessel – Prevent blood loss
Series of event :-
Constriction of blood of blood vessel – Temporary haemostatic plug by platelet – haemostasis
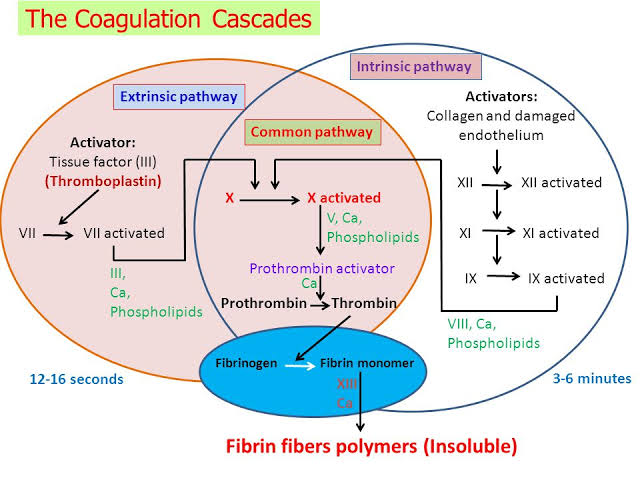
Factors responsible for coagulation :-
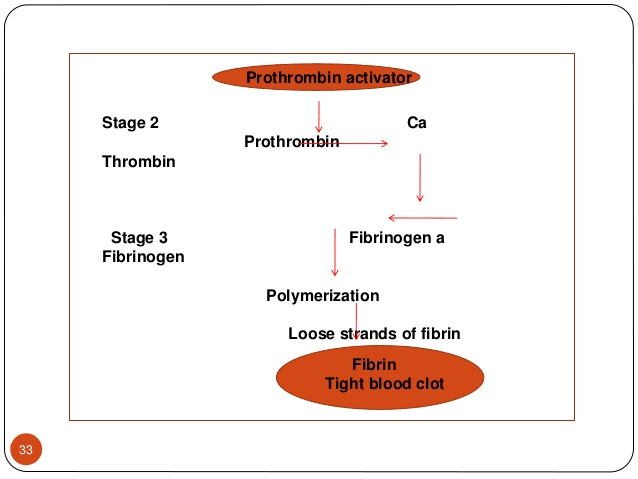
Fibrin formation :- by soluble plasma fibrinogen due to f3,f4,f6
Thrombin formation :- inactive prothrombin into thrombin by prothrombin activator
Prothrombin activator :- by extrinsic and intrinsic factor
Clot retraction :- conversion of prothrombin to thrombin within 15-30min
Role of Calcium :- it act as catalyst in cascade reaction
Why does not blood clot in circulation? Smoothness of endothelial line prevents adhesion. Negatively charged particles repells cloting factor. Natural anticoagulant eg :- heparin in circulation
Reference :- Book Human physiology for bds A.K Jain Google website slide player
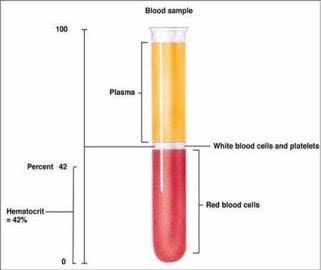
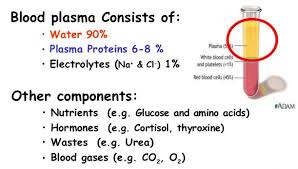
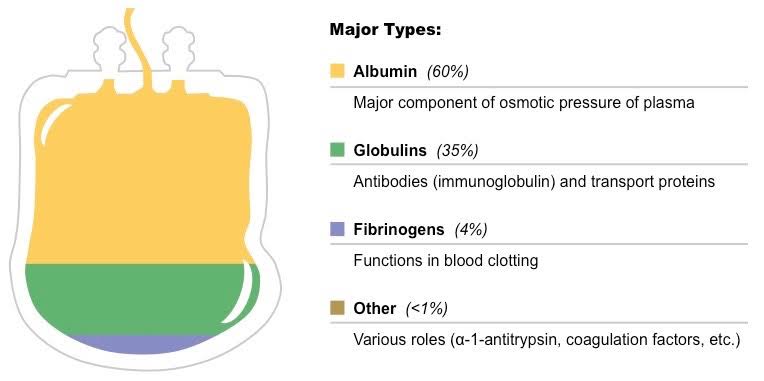
Plasma proteins :- They are also know as blood proteins. They are proteins which are present in blood plasma
Constituents :-
Origin :-
Embryo from Mesenchymal cell
Adult albumin from liver
Globulin from tissue, macrophages,plasma cells, lymphocytes
Types :-
Albumin :- 1.control collodial osmotic pressure 2.transport anion,cation,drugs,hormones,enzymes,billirubin
Globulin :- regulate iron absorption and transport
Fibrinogen :- helps in clotting
Hepatoglobin :- prevent loss of iron in urinary excretion
Variation in plasma concentration :- Decrease – haemorrhage causes loss of plasma protein. Fibrinogen, albumin,globulin are regenerated by restoration effect in few days. Decrease of albumin causes during pregnancy,chronic liver disease, malnutrition,fasting, malabsorption,burn,nephrosis. Increase – loss due to burn or dehydration
Functions :-
Helps in coagulation of blood
Helps in maintaining colloidal osmotic pressure by urea,Na+,glucose
Helps in maintaining Hydrostatic Pressure across cavity wall
Helps in maintaining viscosity of blood
Helps in Hypoproteinemia
Helps in immune function
Reference :- Book Human physiology for bds A.K Jain Google website studyblue.com, Philadelphia.edu.jo
Integumentary system serves to both protect the body and assist in the maintenance of homeostasis.
Comprises the skin, which divides into:
The Epidermis
The Dermis
The Skin Accessory Organs (derivatives): hair, glands, and nails
EPIDERMIS
Superfical to Deep:
Stratum corneum
Outermost layer; it comprises numerous rows (25-30) of flat, dead cells.
Contain keratin.
Continually sloughed.
Stratum lucidum
Comprises clear-appearing cells.
Lack nuclei and organelles.
Contain keratin and eleidin.
Stratum granulosum
Comprises 3-5 rows of cells that contain keratohyaline granules.
Help form the keratin cells of the epidermis.
Stratum spinosum
Comprises, most notably, several rows of keratinocytes.
They are called prickle cells due to their spiny appearance.
Within the stratum spinosum layer, desomosomes exist, which form intercellular bridges.
Stratum basale
Forms the deepest layer of the epidermis.
It comprises a single layer of cuboidal keratinocytes that are active in cellular reproduction (mitosis).
Responsible for hair growth
Occurs when stratum basale generates new hair cells that push the old, keratinized hair cells through the follicle to form hair fibers.
Note that melanocytes and Merkel cells also exist within this layer.
Melanocytes are responsible for the formation of melanin, which derives from tyrosine.
“Come Let’s Get a Sun Burn”
Use the “Come Let’s Get a Sun Burn” to remember the layers
Come – Corneum
Let’s – Lucidum
Get a – Granulosum
Sun – Spinosum
Burn – Basale
TYPES OF SKIN
Thin skin
Most ubiquitous form of skin
Thin skin lacks a stratum granulosum and stratum lucidum and has a relatively small amount of stratum corneum.
75 to 150 μm thick.
Thick skin
Restricted to discrete areas that are commonly traumatized.
Key regions: palms and soles.
Thick skin contains both stratum granulosum and stratum lucidum.
Has a prominent stratum corneum.
400 to 600 μm thick.
DERMIS AND SKIN ACCESSORY ORGANS
Papillary layer, with dermal papillae
Forms a thin layer of loose connective tissue with finger-like projections, called dermal ridges (aka dermal papillae).
They interdigitate with the epidermal down-growths (epidermal papillae) — they form fingerprints.
Reticular layer
Forms the bulk of the dermis.
It comprises a dense layer of collagen bundles and elastic fibers
(as opposed to the papillary layer, which is loosely constructed)
Hypodermis
Superficial fascia layer (and not a layer of the skin).
ACCESSORY ORGANS
Derivatives/appendages of the skin.
Hair
Shaft, root, and dermal papilla.
Hair follicle invaginates the epidermis.
The outer root sheath of the hair follicle is continuous with the epidermis.
Hair follicle comprises:
Hair shaft, which is the slender filament at the center of the follicle that extends above the epidermis.
Hair root, which is the expanded region of the hair follicle, deep within the dermis at the root of the hair follicle.
Dermal papilla, which contains the capillary network that nourishes the hair follicle; not to be confused with dermal papilla that interdigiate with epidermis.
Arrector pili
Smooth muscle attached to the dermal sheath surrounding the hair follicle.
Glands
Sebaceous glands
Commonly associate with hair follicles;
Sebaceous glands are branched acinar, holocrine glands, which have a lobulated appearance.
They secrete sebum (an admixture of an oily/lipid substance and degenerating epithelial cells) into hair follicles.
Keeps hair supple, skin soft, protects against microorganisms, and maintains the hydration status of the epidermis.
Sweat Glands: Eccrine and Apocrine
Eccrine glands secrete sweat and are most prominent on the palms, soles of the feet, and forehead.
Sweat is formed through the filtration the blood into a hypotonic solution that is primarily water with small amounts of such products as salt, antibodies, metabolic waste, vitamin C, and dermcidin.
Apocrine glands are specialized, and (unlike the nearly ubiquitous eccrine glands) are confined to specific regions, namely: the axilla, areolar nipple, and perianal region.
Other apocrine, non-sweat producing glands are ceruminous glands, which lie in ear canals and secrete cerumin, and mammary glands, which produce and secrete milk.
Nails
Comprise a nail bed, nail plate, cuticle, lunula, hyponchium, and nail root.
Other stuctures:
Blood vessels
Vascularize the dermal papilla
Sensory nerve receptors
Within papillary layer
Meissner copuscles
Mechanosensitive (light touch detection)
Unmyelinated nerve fibers
Transmit pain and temperature sensation.
Within reticular layer
Pacinian corpuscles
Krause end-bulbs
Mucocutaneous (eg, oral cavity) receptors.
Clinical Correlations
Neuropathy
See Sensory Receptors
CLINICAL CORRELATIONS: COMMON SKIN LESIONS
Flat, Discolorations
Macules
Patches
Raised Lesions
Papules
Nodules
Plaques
Blisters
Vascular Lesions
Petechiae
Purpura
Ecchymosis
Infectious Lesions
Pustules
Vesicles
Venous-backflow Lesions
Varicose Veins
Stasis Dermatitis
PHASES OF HAIR GROWTH
Human hair grows at 2mm per day.
Human head has ~ 150,000 hairs.
Anagen phase
Growing phase
Catagen phase
Growth respite phase.
Telogen phase
Terminal resting phase (when hair falls out).
HAIR COLOR
Hair derives its color from the melanocytes that lie within the hair follicle basement membrane on the surface of the dermal papilla.
Physiology is among the most important topics from NEET MDS point of view as it forms the basic building blocks of some of the highly scoring and significant subjects such as Oral Medicine, Pathology and General medicine. The biggest challenge for students preparing for NEET MDS is that the students find themselves forgetting the topics they took days to finished. Here arises the biggest confusion as to which subjects should be approached when and how. The article aims to highlight the preparation strategy that must be followed when you are preparing for Physiology. Let us first take a look at list of standard books to refer & most important topics that you cannot afford to leave out at any cost.
Given below are the list of Questions MERITERS experts will answer that are essential for an effective and efficient preparation:
How much Time should be allocated for the Subject?
Theory reading – 4 Days
MCQ Practice- 10-15 Days
How much Time should be allocated to each Topic?
Theory reading – 3-4 Hours
MCQ Practice- 5-8 Hours
How many Times should the subject be Revised?
4-6 times revision is required
What is the Ideal time to Start the subject?
3rd quarter of the preparation
After completing 13-14 subjects
Physiology – Important Topics
UNIT
MOST IMPORTANT TOPICS
GIT and liver
Saliva, oesophagus and stomach Pancreatic secretions Gall bladder and bile Small and large intestine Digestion
Respiratory system
Transport of gases Oxygen dissociation curve lung volume and capacities Hypoxia Regulation of breathing and respiratory failure Surfactant and miscellaneous
Renal system
Renal system an overview
Muscles and Neuromuscular junction
Types of nerve fibers Muscle spindle and Golgi tendon Nerve conduction and NM junction Nerve injury
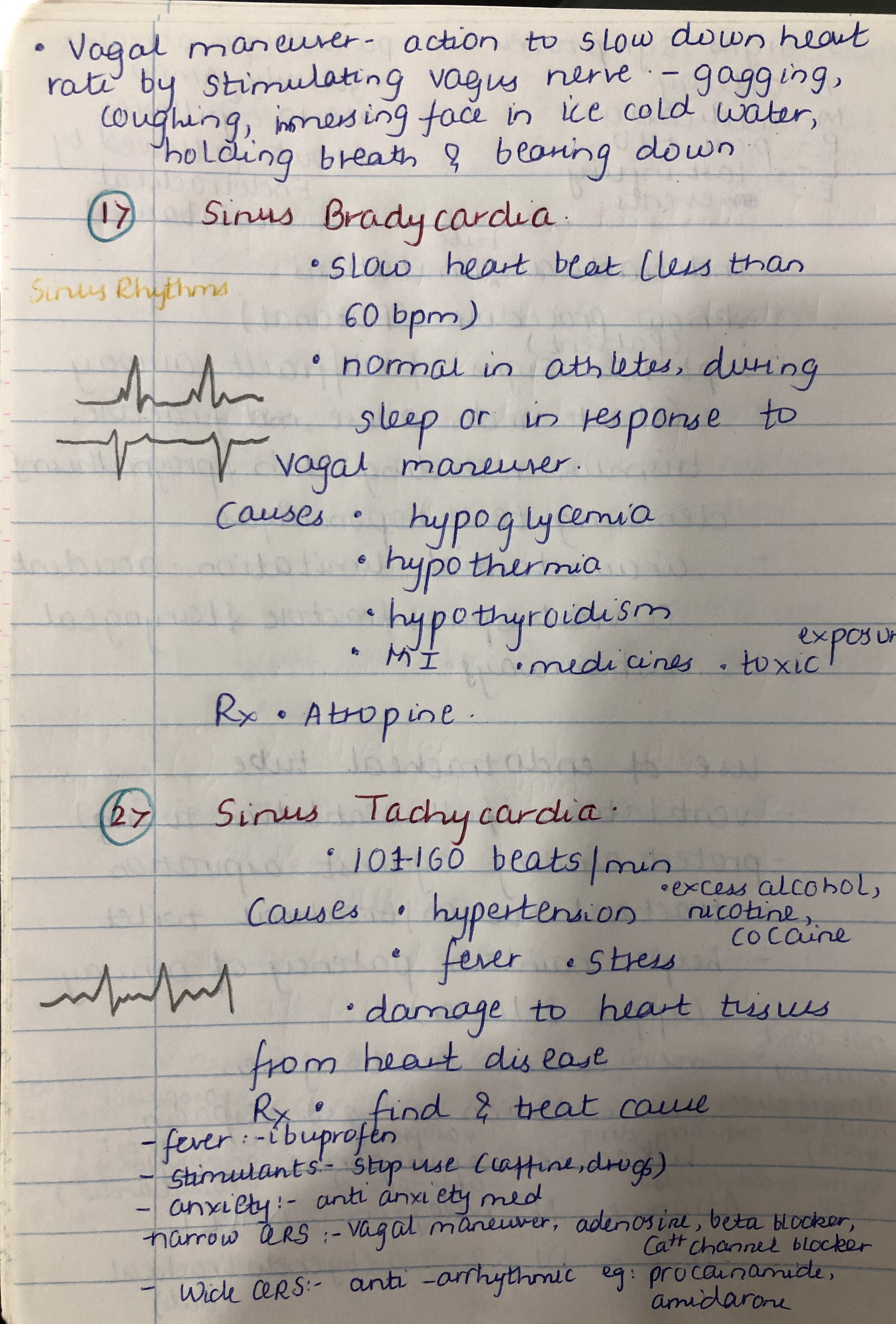
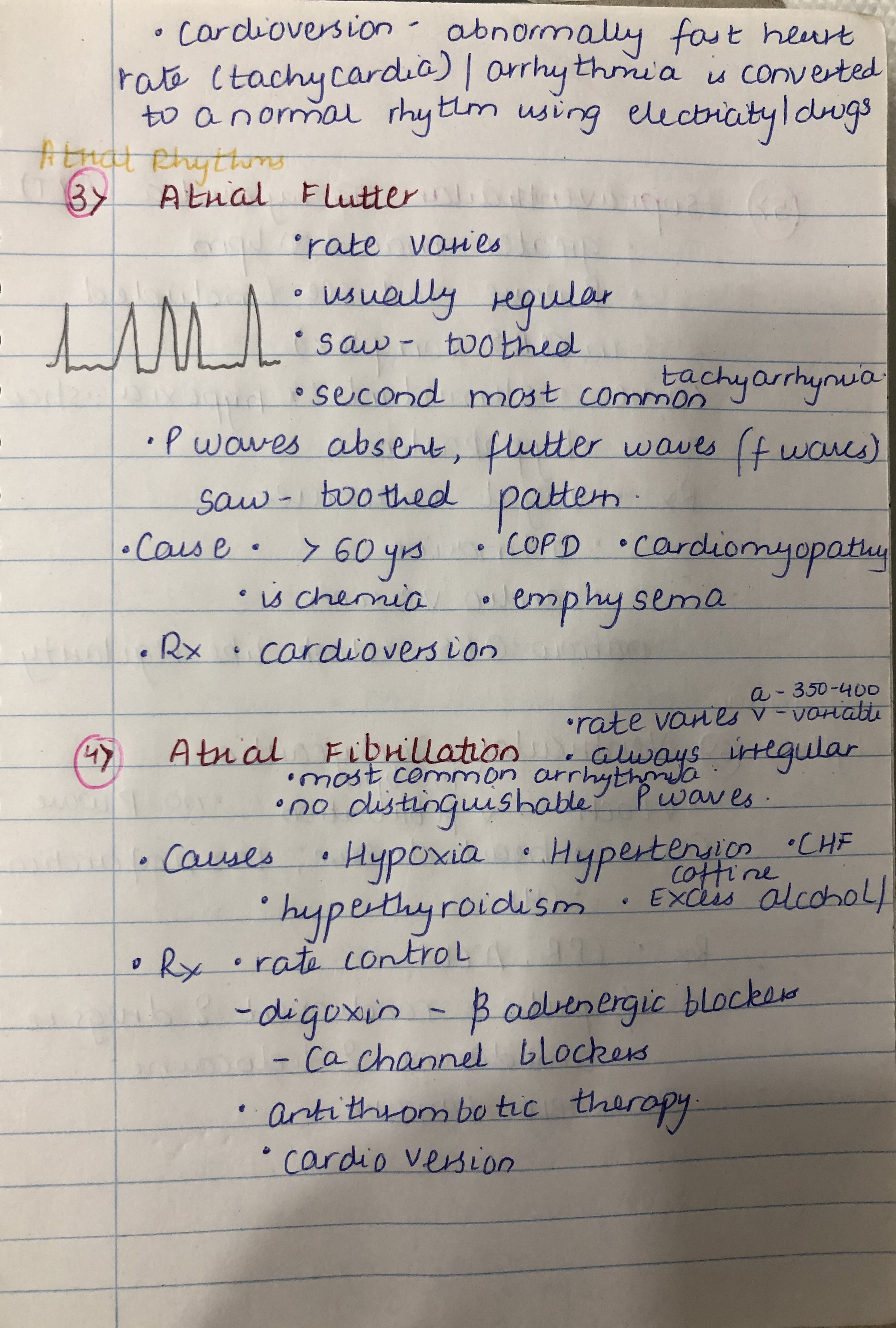
Cardiovascular system
Electrical activity of heart Heart as a pump Blood pressure Cardiovascular regulatory mechanism Circulation through special regions
Central nervous system
Central nervous system an overview
Hematology
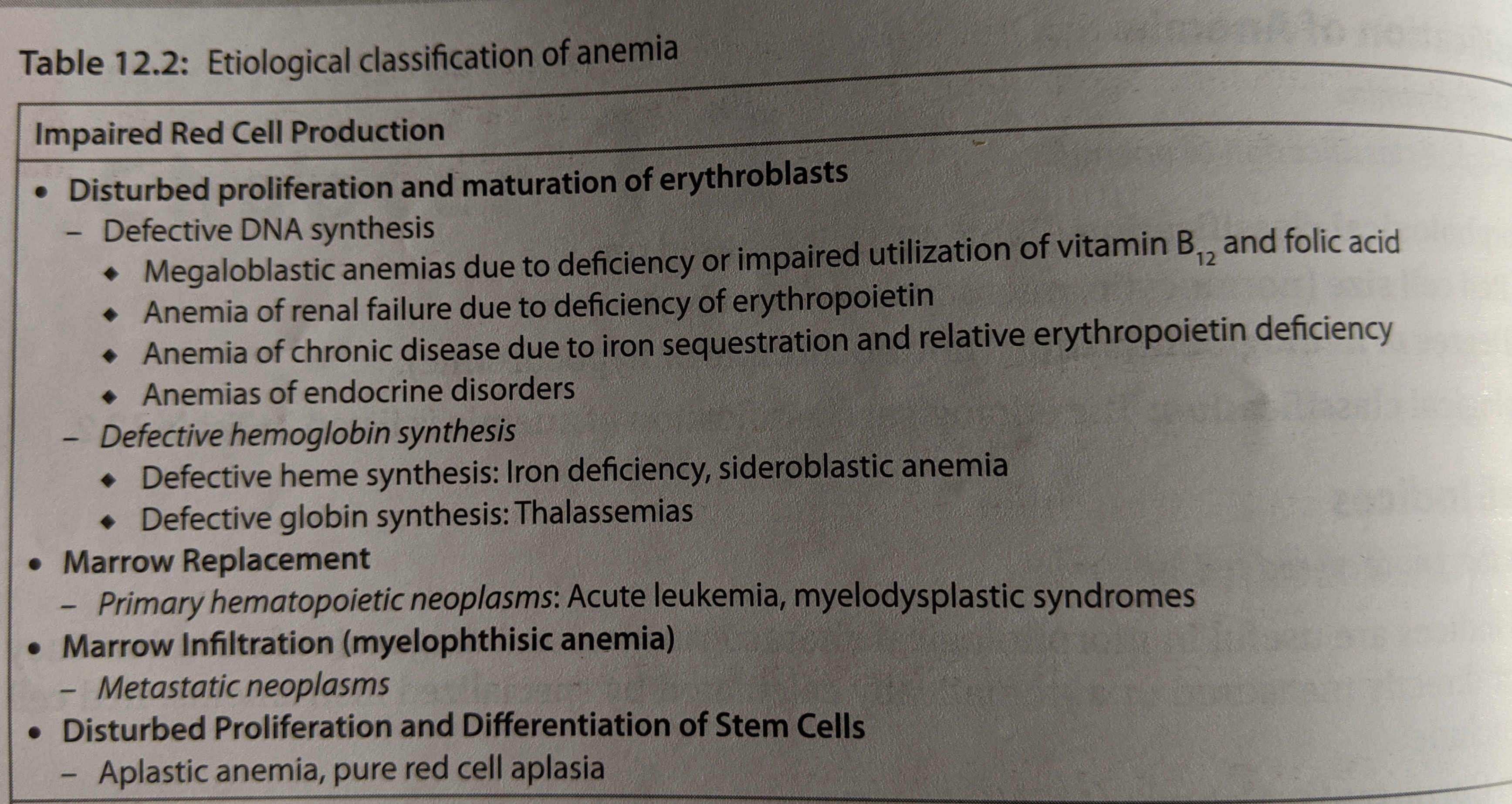
Blood an overview(add absorption increasing factors) Anaemia
Endocrinology
Receptors and secondary messengers Calcium metabolsm and Parathyroid gland Pancreatic hormones Pituitary gland Thyroid and Adrenal gland Other hormones including reproductive hormones
General Physiology
Cell membrane Transport across cell membrane Genral Physiology and Body fluids Cell organells Extracellular matrix
What Type of Questions were asked in NEET?
1. Single best answer
Fact Based (Memory)
Concept based
Numerical/Value Based
2. Image based questions
3. True or false type questions
Please watch the above featured video for more detailed explanation about this article.
We hope this blog will assist you in preparing this subject meticulously for MDS entrance exams. Prepare judiciously..
Metabolic acid-base disorder presents as an imbalance between bicarbonate, the primary extracellular buffer, and fixed, aka, non-volatile, acids.
Respiratory acid-base disorder presents as an imbalance between bicarbonate and carbon dioxide, the volatile acid.
Acid-base Disorders are distinguishable by their arterial blood profiles, compensatory respiratory and renal mechanisms, and common causes.
ACIDEMIA
pH < 7.35
Metabolic acidosis
Bicarbonate < 20 mEq/L
Caused by either a gain in hydrogen ions and/or a loss of bicarbonate, which lowers pH.
Consequently, the arterial blood profile shows reduced bicarbonate concentration and elevated hydrogen ion concentration.
In response to a drop in pH, the respiratory systemcompensates with hyperventilation:
Excess carbon dioxide is “blown off,” which lowers the partial pressure of carbon dioxide in the blood; the arterial blood profile reflects this.
Though slower to respond, renal bicarbonate conservation and acid excretion produce a more effective and longer-lasting pH elevation.
Anion Gap
Causes of metabolic acidosis into at least two categories: those associated with a normal anion gap (AG), and those associated with an elevated anion gap.
In a routine blood test, only some cations and anions are measured; the anions that are not measured constitute the “anion gap.”
Because the total concentration of anions must be equal to the total concentration of cations, we know that the anion gap, the unmeasured anions, must be equal to: The measured cations (usually sodium) minus the measured anions (usually bicarbonate and chloride).
A normal average anion gap value is 12 mEq/L (typical range = 8 – 16 mEq/L).
Thus, an increased anion gap indicates that bicarbonate, a measured anion, has been lost and replaced by the unmeasured ions
A normal anion gap indicates that chloride is the ion that replaced the lost bicarbonate, which makes sense given that it is the other measured anion in the anion gap equation.
Common causes of a normal anion gap include:
Diarrhea
Renal tubular acidosis
Renal failure
Hyperchloremia
Addison disease
Acetazolamide
Spironolactone
Saline infusion
Common causes of an increased anion gap include MUDPILES:
Methanol intoxication (methanol is also called “wood alcohol,” commonly found in antifreeze and industrial settings)
Uremia
Diabetic ketoacidosis
Paraldehyde (which is sometimes used to treat alcoholism and certain convulsive and mental disorders)
Iron overdose
Lactic acid
Ethylene glycol poisoning (ethylene glycol is a compound commonly found in antifreeze)
Salicylate ingestion (key ingredient in aspirin, poisoning is common in children)
Respiratory acidosis
Pco2 > 44 mmHg
Caused by a gain in carbon dioxide and bicarbonate.
The degree of change in pH depends on the duration of the disorder:
The pH is more reduced in acute acidosis than in chronic because, in chronic acidosis, sufficient time has elapsed for renal mechanisms to have some effect.
There is no respiratory compensation when the respiratory system is itself the source of the imbalance.
To raise pH, the nephrons conserve bicarbonate and excrete hydrogen ions; notice that this is similar to the renal response to metabolic acidosis.
Caused by:
Hypoventilation
Inhibition of the medullary respiratory center, which can be induced by sedatives or brainstem lesions
Neuromuscular defects that inhibit the anatomical structures responsible for ventilation
Gas exchange defects, such as COPD.
ALKALEMIA
pH > 7.45
Respiratory alkalosis
Pco2 < 36 mmHg
pH is increased in proportion to the duration of the disorder.
There is no respiratory compensation for respiratory-induced acid-base disturbances.
Nephrons excrete excess bicarbonate and reduce titratable acid and ammonium ion secretion to conserve hydrogen ions; this is similar to the renal response to metabolic alkalosis.
Caused by:
Hyperventilation, which “blows off” too much carbon dioxide and lowers its arterial partial pressure.
Stimulation of the medullary respiratory center, hypoxemia (low blood oxygen), and physical or mental distress.
Metabolic alkalosis
Bicarbonate > 28 mEq/L
Caused by a loss of hydrogen ions and/or a gain in bicarbonate, which raises pH.
Consequently, the arterial blood profile shows elevated bicarbonate concentration, and decreased hydrogen concentration.
In response to elevated pH, hypoventilation retains carbon dioxide, which increases its arterial partial pressure; this is reflected in the arterial blood profile.
The nephrons increase bicarbonate excretion, and, by reducing secretion of titratable acids and ammonium, conserve hydrogen ions; these actions lower pH.
Most commonly caused by
Vomiting (HCL is lost from the body)
Loop and thiazide diuretics, which increase bicarbonate excretion in the urine.
Vomiting and diuretics cause extracellular fluid volume contraction, which, as we’ve learned elsewhere, triggers hormonal responses that increase bicarbonate reabsorption and maintain the metabolic alkalosis.
Hyperaldosteronism (excessive aldosterone secretion) causes over-excretion of hydrogen ions.
Volatile acid is the product of aerobic cellular respiration, which releases carbon dioxide. As we’ve learned elsewhere, when carbon dioxide interacts with water in the body fluids, carbonic acid forms.
“Volatile” refers to the fact that carbon dioxide is expired by the lungs
Non-volatile acids are the products of protein and phospholipid metabolism
They include sulfuric acid and phosphoric acid
They are excreted in the urine as titratable acids
Because enzymes and other proteins only function at particular pH values, the body must regulate the acidity of the intra- and extracellular fluids.
Three lines of defense against acid-base imbalance:
In the body, fluids (chemical mixtures), called buffers, minimize pH changes until hydrogen balance can be regained.
The respiratory system expires carbon dioxide, the source of volatile acid.
The urinary system excretes the non-volatile, aka, fixed, acids.
These systems operate interdependently to maintain an arterial blood plasma pH of 7.4.
Acid Production by Body Tissues
Body tissues produce acids, including carbon dioxide, sulfuric acid, and phosphoric acid
Each of these acids releases hydrogen ions that must be buffered in the body fluid compartments.
Buffering in Fluid Compartments
Intracellular compartment of body tissues = proteins and organic phosphates
Intracellular compartment of red blood cells = hemoglobin
Extracellular fluid = bicarbonate, which is the most important extracellular buffer, and, phosphate and proteins.
Acid Removal
In the Lungs
When carbonic acid reaches the lungs, it dissociates to form carbon dioxide, which is expired in ventilation.
When pH falls, increased ventilation triggers to release excess carbon dioxide. Rapidly, the partial pressure of carbon dioxide drops, and the acidity of the blood is reduced.
In the Kidneys
Nephrons reabsorb bicarbonate from the filtrate, and excrete hydrogen ions as tritratable acids and ammonium in the urine.
Nearly all of the filtered bicarbonate is reabsorbed from the proximal tubule.
Some hydrogen ions attach to ammonia and are secreted into the filtrate as ammonium; some of this ammonium is then reabsorbed from the thick ascending limb (where it participates in countercurrent multiplication in the renal interstitial fluid).
In the alpha-intercalated cells of the distal nephron, ammonium is again secreted into the tubular fluid, along with phosphoric acid. Phosphoric acid forms when hydrogen ions attach to phosphate, and is often referred to as “titratable acid”
Ammonium and phosphoric acid formation and secretion involve bicarbonate synthesis and reabsorption; this new bicarbonate contributes to the extracellular buffers.
Both mechanisms are responsive to aldosterone, which is a hormone secreted by the adrenal cortex secreted in response to low pH.
Clinical correlations
Aldosterone deficiency inhibits ammonium excretion, and causes type 4 renal tubular acidosis. Because potassium excretion is also inhibited by aldosterone deficiency, this type of acidosis is characterized by hyperkalemia.
Alkalosis is a consequence of excessive removal of hydrogen ions from the body fluids; as a result, the blood becomes more alkaline).
Acidosis is the opposite: excessive hydrogen ions are added to the blood or retained; the blood becomes more acidic. Retention of acids can be a sign of renal failure.
Acids and bases are defined by their ability to donate or accept hydrogen ions
Acids are chemical substances that can donate/release, hydrogen ions in water.
Bases, aka, alkalines, are chemical substances that can accept hydrogen ions.
pH
pH is a measure of the concentration of hydrogen ions in solution
pH scale displays the concentration of hydrogen ions from 0 – 14.
An acidic solution has a pH less than 7; it has a high concentration of hydrogen ions.
A neutral solution has a pH of 7
A basic solution has a pH of greater than 7; it has a lower concentration of hydrogen ions.
Calculation of pH:
Negative logarithmic function.
pH values for human bodily fluids:
Gastric juice, which is secreted by organs of the digestive system, has a pH value around 2; its acidity aids in food digestion.
Saliva is slightly acidic, but much closer to neutral than are the gastric juices.
For comparison, pure water has a neutral pH, 7.
Arterial blood has a pH of approximately 7.4
Homeostasis
Biological organisms are constantly adding acids to their bodily fluids during metabolism, but our blood is slightly basic.
Intra- and extra-cellular buffers operate to maintain homeostasis.
Buffers minimize changes of pH in solutions; they reversibly donate or accept hydrogen ions.
Example: Bicarbonate buffer system: When hydrogen ions are added to the extracellular fluid, they combine with bicarbonate to produce carbonic acid, which is a weaker acid.
If the extracellular fluid becomes too basic, the reaction can be reversed: Carbonic acid can dissociate to form hydrogen ions and bicarbonate; when pH increases (becomes more alkaline), carbonic acid dissociates to form bicarbonate, which is a base, and hydrogen ions.
Clinical Consequences
If the body cannot maintain homeostasis due to pathology, disturbances in bodily fluid pH inhibit enzymatic reactions. -Thus, failure to regulate pH causes a range of clinical symptoms associated with acidosis (too high blood acid content) or alkalosis (too low blood acid content); elsewhere, we discuss how the kidneys and lungs work to maintain homeostatic pH levels.