source – don’t remember, had written it a lot time ago
Category: Pharmacology
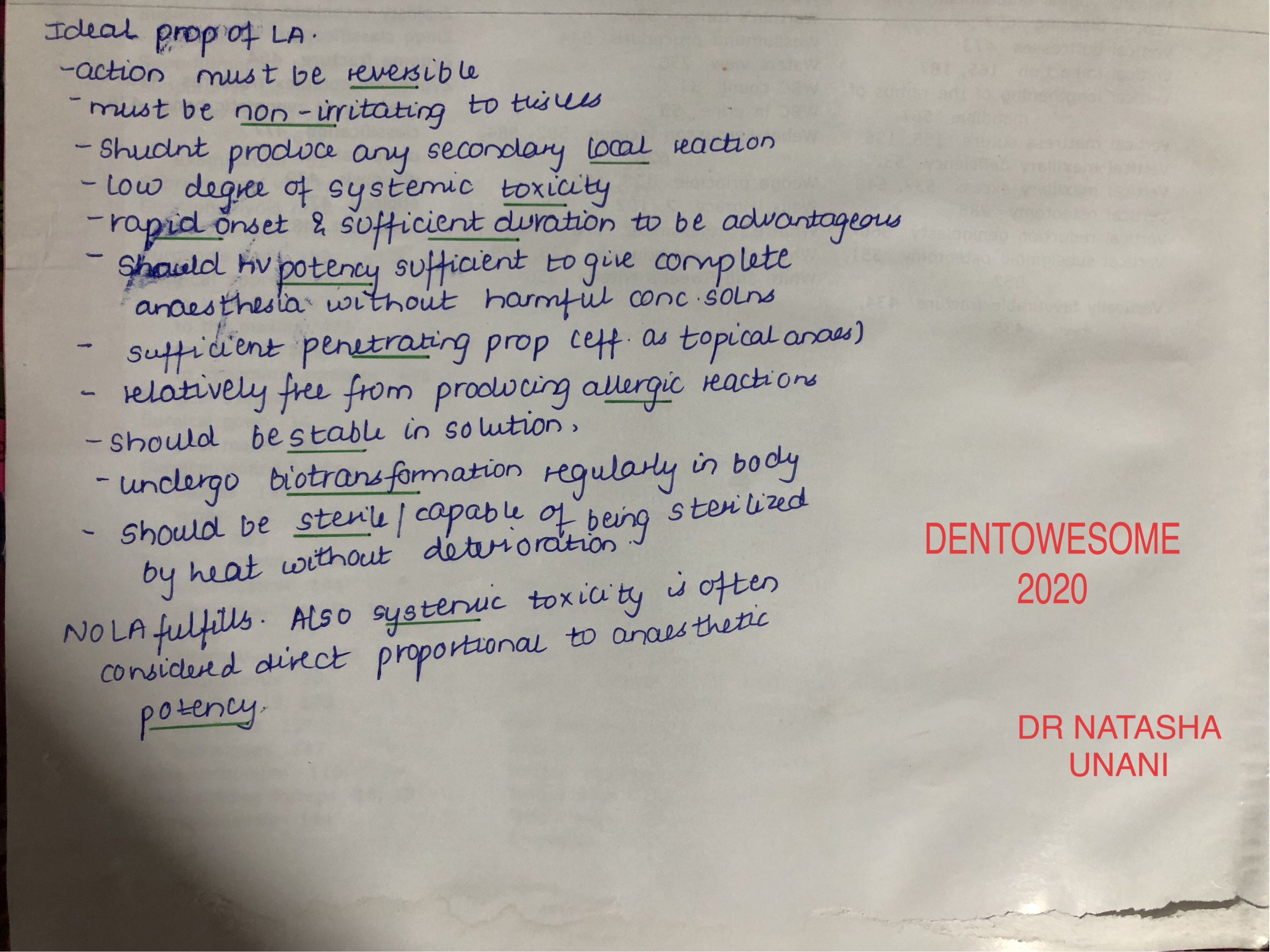
IDEAL PROPERTIES OF LA
source – don’t remember, had written it a lot time ago
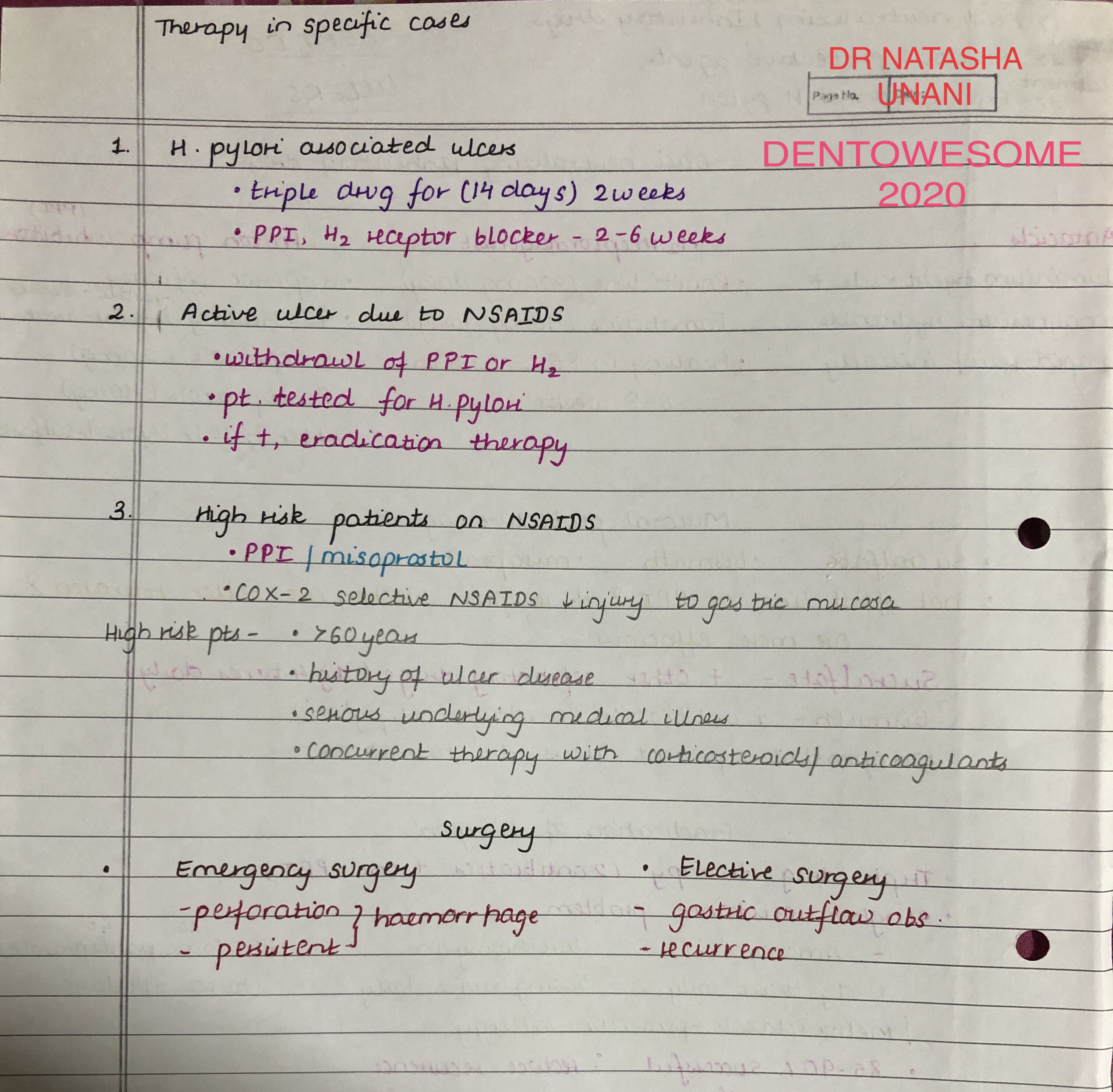
PEPTIC ULCERS

source – don’t remember, had written it a lot time ago
RESPIRATORY FAILURE

source – don’t remember, had written it a lot time ago
Anti-arrhythmic Drugs: Classes II through IV (+ Others)
Class II: Beta blockers
- Treat both supraventricular and ventricular arrhythmias.
- Slow channel blockers, so they work at the sinoatrial and atrioventricular nodes; more generally, as we’ve learned elsewhere, beta blockers reduce sympathetic stimulation.
- We draw the normal curve of an action potential through the nodes.
- Then, we show that beta blockers inhibit phase 4 depolarization and slow conduction through the atrioventricular node.
- Suppress ectopic pacemakers.
- Slow heart rate and reduce contractility.
- Prolong the PR interval on ECG.
- Examples
– Drugs that are often used to prevent recurrent myocardial infarction:
Propranolol, which also stabilizes membranes (a class I action)
Metoprolol
Nadolol
Timolol
– Esmolol is a cardioselective beta-1 receptor blocker and is short-acting.
– Thus, it is used to treat acute arrhythmias. - Common beta blocker side effects: bradycardia, hypotension, bronchospasm (with non-selective beta blockers, specifically), and, myocardial depression.
Class III: Potassium Channel Blockers
- Treat tachyarrhythmias, including re-entry arrhythmias.
- We Draw the normal curve of an action potential in the ventricles.
- Then, we indicate that potassium channel blockers delay repolarization, prolong the action potential, and lengthen the effective refractory period.
- The drugs we’ll focus on the most, amiodarone and its derivative, slow the heart rate and atrioventricular node conduction; these additional actions are due to their abilities to block beta adrenoreceptors, sodium, potassium, and calcium channels.
- Class III drugs prolong the QT interval on the ECG.
- Examples
– Amiodarone, which, due to the various channels and receptors it blocks, is a mix of classes I-IV. Its wide spectrum of action makes it a popular drug of choice in a variety of arrhythmias.
Amiodarone is lipophilic, and is widely distributed through the body tissues.
Widespread potential side effects:
Liver toxicity and cirrhosis
Interstitial pneumonitis, which can lead to pulmonary fibrosis
Corneal microdeposits, which are caused by amiodarone-induced lipidosis in the eye
(we show their “whorl-like” pattern(
Photosensitivity/phototoxicity can produce a rash or even give the skin a gray-blue tint
And, because amiodarone is iodine-rich, it can cause hypo- or hyperthyroidism.
Amiodarone can also cause sinus bradycardia
– Dronedarone is a synthetic, non-iondinated derivative of amiodarone (it doesn’t have iodine).
It is used to treat atrial fibrillation, and is generally considered less toxic, but less powerful, than amiodarone.
It is, however, associated with liver toxicity.
– Sotalol, which also has class I beta blocking actions, is associated with torsades de pointes. - As a warning, write that most class III drugs are significantly pro-arrhythmic; amiodarone and dronedarone are important exceptions, as they less likely to precipitate arrhythmias.
Class IV: Calcium Channel Blockers
- Treat supraventricular arrhythmias and to reduce ventricular rate in atrial flutter and atrial fibrillation.
- They block calcium channels, so they are most effective at the sinoatrial and atrioventricular nodes, which rely on calcium ions for rate control.
- We draw the curve of a normal nodal action potential, and show that calcium channel blockers prolong nodal conduction and the effective refractory period.
- They prolong the PR interval on ECG (like the Class II drugs).
- We use non-dihydropyridine calcium channel blockers
- Examples
– Verapamil and Diltiazem; both target myocardial cells, and diltiazem has some vasodilator effects.
Both drugs are associated with constipation, and, due to their negative inotropic effects, can cause bradycardia and lower cardiac output.
Thus, use caution when combining these drugs with beta blockers, which have similar effects, and, avoid using in patients with heart failure with reduced ejection fraction.
Class V: Others
Finally, let’s consider the “others” category, sometimes collectively called “Class V”.
Adenosine is used to treat supraventricular tachycardias; it slows or blocks conduction in the atrioventricular node.
– It’s important to know that theophylline (a common asthma medication) and caffeine reduce adenosine’s efficacy by blocking its receptors.
– Adenosine may trigger bronchospasm.
Magnesium ions are sometimes used to treat torsades de pointes and digoxin toxicity.
Potassium ions may be used in some patients to slow conduction and can suppress ectopic pacemakers.
Digoxin can be used in some patients to treat atrial flutter or atrial fibrillation; it slows or blocks conduction in the atrioventricular node by inhibiting sodium-potassium ATPase.
– However, digoxin can cause ectopic arrhythmias, gastrointestinal and visual side effects, and breast enlargement (gynecomastia, in males), and has been associated with increased risk of breast and uterine cancer, likely due to its phyto-estrogen effects.
Anti-Arrhythmic Drugs: Class I
Anti-Arrhythmic Drugs Overview
- Arrhythmias are characterized by abnormal generation and/or conduction of electrical impulses, which produce abnormal rate and/or activation sequences in the cardiac tissue. Ultimately, this can reduce cardiac output.
Supraventricular Arrhythmias
Ventricular Arrhythmias
AV Node block - Class 1 drugs are sodium channel blockers; we’ll focus on this group in this tutorial.
- Class 2 drugs comprise the beta blockers.
- Class 3 drugs include the potassium channel blockers.
- Class 4 drugs comprise the calcium channel blockers.
- Magnesium and adenosine are also used to treat arrhythmias.
- Paradoxically, anti-arrhythmic drugs can actually precipitate fatal arrhythmias; thus, the potential harm of these drugs may outweigh their potential benefits in some patients.
Action Potenial
Review
- Phase 0 = Fast sodium channels open and ions quickly move into the cell, which causes rapid depolarization.
– Class 1 antiarrhythmics affect the slope of this line. - Phase 1 = Potassium channels open, which allows potassium ions to move out of the cell and cause early repolarization.
- Phase 2 = The plateau phase; potassium continues to move out of the cell, and calcium move into it.
- Phase 3 = As more potassium channels begin to open, and calcium channels close, Phase 3 is characterized by rapid repolarization.
- Phase 4 = Resting phase, during which “leaky” potassium channels maintain resting membrane potential.
- Effective refractory period is the time when new action potentials cannot be triggered.
Effects of Class 1 anti-arrhythmics on this curve
- These drugs are fast-sodium channel blockers; they also have local anesthetic properties.
- They slow the rate of Phase 0 depolarization and conduction velocity.
- Class 1 drugs are further classified by their effects on the duration of action potentials.
– Class 1a drugs prolong the duration of the action potential
– Class 1b drugs shorten its duration
– Class 1c drugs have minimal effect
Details
Class 1a
- Used to treat atrial and ventricular arrhythmias.
- Moderate sodium channel blockers, and also block some potassium channels.
- They prolong the action potential duration, effective refractory period, QRS complex, and QT interval.
- Examples and their most common side effects:
– Procainamide is associated with hypotension; long term use is typically avoided because the drug can cause lupus-like syndrome, characterized by arthralgia and purpura.
It is generally considered the third best choice in myocardial infarction arrhythmias (behind amiodarone and lidocaine).
– Quinidine is associated with gastrointestinal side effects, cinchonism (headache, dizziness, and tinnitus), and thrombocytopenia.
– Disopyramide are due to its anticholinergic effects (for example, constipation, urine retention, dry mouth, blurred vision). Can worsen glaucoma, and is not suitable for patients with heart failure. - All Class 1a drugs can precipitate torsades de pointes.
Class 1b
- Used to treat ventricular arrhythmias.
- They are weak sodium channel blockers, and are selective for ischemic tissue and depolarized Purkinje fibers and ventricular myocytes.
- These drugs shorten the action potential duration and effective refractory period, but have no effect on the QRS complex or QT interval.
- Lidocaine is the prototypical class 1b drug; it is second in line to treat arrhythmias associated with myocardial infarction (behind amiodarone).
– Lidocaine has low toxicity, but, in vulnerable patients or when given in high doses or administered too rapidly, it is associated with neurological, and, more rarely, cardiovascular side effects.
– Neurological effects include paresthesia (tingling, “pins and needles,” usually in the hands and feet), dizziness, and confusion.
– Cardiovascular effects include sinus bradycardia, arrhythmias, and shock. - Phenytoin is often considered an honorary member of class 1b anti-arrhythmias; it is used to treat arrhythmias caused by digitalis.
Class 1c
- We’ll list characteristics for the prototypical drug, Flecainide; as we’ll see, however, not all class 1c drugs have the same effects.
- Used to treat supraventricular arrhythmias.
- Strong sodium-channel blockers that also block some potassium channels.
- Flecainide has no effect on the duration of action potentials or the effective refractory period; it prolongs the QRS complex with little effect on the QT interval.
- Common side effects are dizziness, headaches, and visual disturbances, which may include blurred vision or difficulty focusing, or the appearance of flashing lights or spots.
- Propafenone has similar side effects; it can exacerbate heart failure (propafenone also blocks beta channels and has negative inotropic effects).
– Unlike flecainide, it is associated with prolonged QT intervals and effective refractory periods. - Moricizine is another class 1c anti-arrhythmic, but it is no longer used in the United States.
- Class 1c drugs are pro-arrhythmic; they are not suitable for patients with structural heart disease.
MOA OF LOCAL ANAESTHESIA

source – don’t remember, had written it a lot time ago
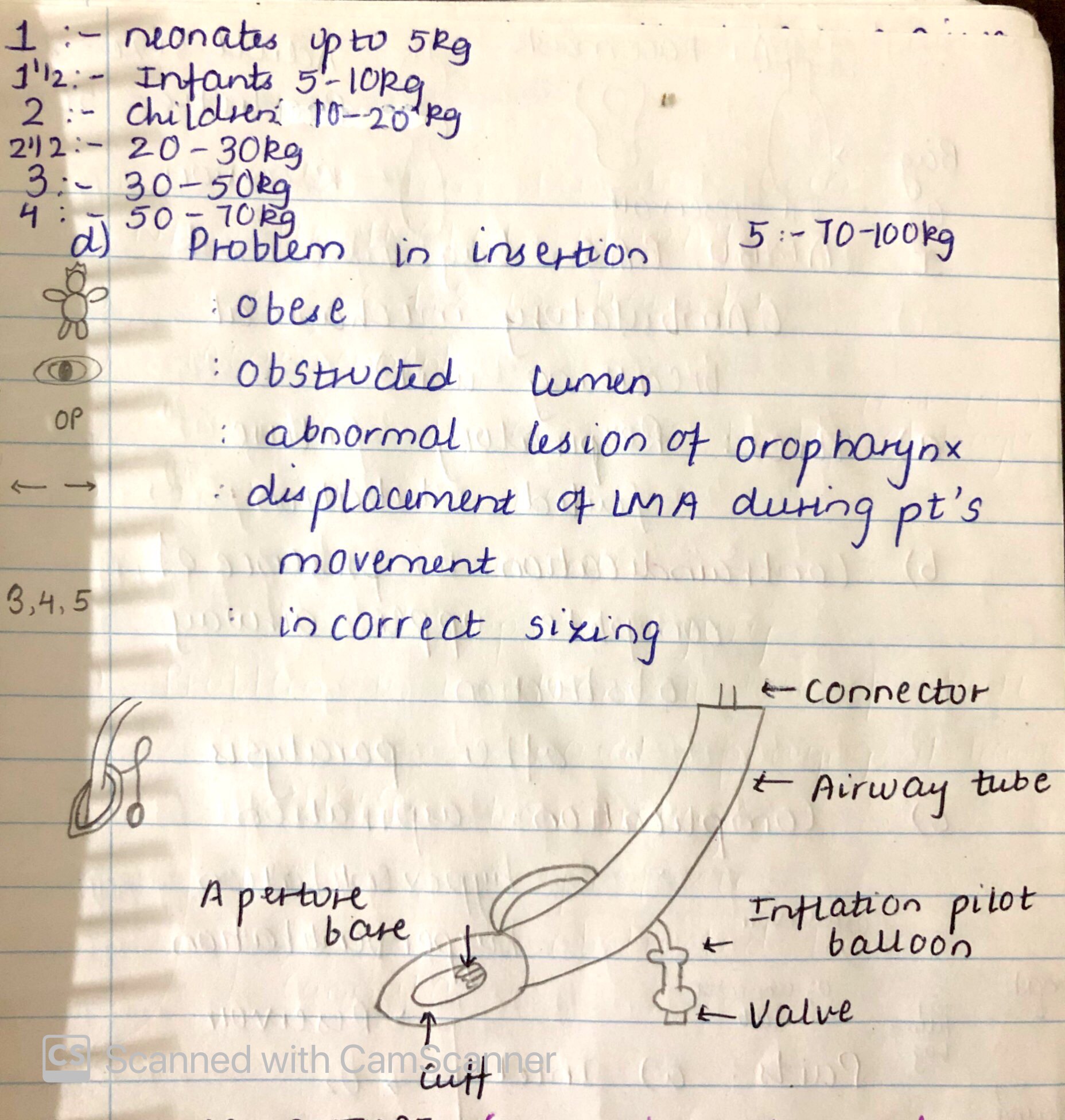
LARYNGEAL MASK AIRWAY

SOURCE – NANCY 13th EDITION
HEART FAILURE

SOURCE – Nancy 13th edition
what you should know about conscious sedation
- Introduction:
Minimally depressed level of consciousness that retains the patient’s ability to independently and continuously maintain an airway and respond appropriately to physical stimulation or verbal command and that is produced by a pharmacological or non-pharmacological method or a combination.
- 2. Features:
- Retains the patient’s ability to maintain a patent airway independently and continuously
- Permits appropriate response by the patient to physical stimulation or verbal command
- Maintains protective reflexes.
- Different routes of administration:
- IV route: deep conscious sedation
IV sedation are more effective than the same drugs taken orally
Advantage: surgeon or anaesthesiologist has complete control of the entire procedure
Disadvantage: profound amnesia
Entral/oral route: sedation dentistry
- All body functions remain normal and the person is able to breathe on their own.
- The patient will often fall asleep. Some degree of amnesia is common.
- The disadvantage with this method of sedation is that the level of sedation for each person is not predictable
- Inhalation conscious sedation : nitrous oxide/ oxygen sedation also known as ‘laughing gas’
- This is the most frequently used sedation method in dentistry.
- All bodily functions remain normal.
- Clinical effects:
- For 20–30 min acute detachment and later a state of relaxation.
- Anterograde amnesia (loss of memory following administration of the drug) for the same period.
- Cardiovascular depression is minimal (the relative hypotension and bradycardia due to the relief of hypertension and tachycardia caused by anxiety).
- In most cases, minimal respiratory depression is seen. The exception is in patients with impaired respiratory function or in those who have taken other depressants such as opiates, alcohol, where the effect may be more marked. However, excessively rapid intravenous injections have the potential to cause respiratory depression leading to apnoea and respiratory arrest, which is life-threatening if not diagnosed and treated promptly.
- Additional properties of benzodiazepines:
- Muscle relaxant
- Anticonvulsant (used to treat status epilepticus).
- Objectives:
- To allay apprehension, anxiety or fear
- To decrease stress associated with traumatic or prolonged procedures
- To control gagging
- To stabilise the blood pressure for patients with hypertension or history of cardiovascular disease.
- Commonly used pharmacological agents:
Benzodiazepines:
- Antianxiety
- anticonvulsant,
- sedative,
- muscle relaxant
- amnesic properties.
Midazolam and diazepam are the medications used in the dental operating set-up.
Midazolam:
Midazolam is a short acting benzodiazepine CNS depressant.
Indication: short diagnostic and surgical procedure
Properties:
- Water soluble
- Nonirritating to veins
- Faster and shorter acting
- Three times more potent than diazepam
- It may be administered IV, IM, PO, rectally or nasally. The most common route of Midazolam is IV.
- Sedative agent that should be administered slowly over 2 min for a single large bolus dose. Rapid or excessive IV doses may result in respiratory depression or arrest. If not recognised and treated promptly, death or hypoxic encephalopathy may result.
- The initial IV dose may be as little as 0.5–1.0 mg.
- Onset of sedation after IV injection is achieved within 3–5 min.
- The duration of effect ranges from 1 to 6.
- The half-life ranges from 1.2 to 12.3 h.
Adverse effect:
- Hiccups
- Nausea
- Vomiting
- Headache
- coughing and pain at the injection site
Diazepam:
- Indicated for conscious sedation prior to short diagnostic or surgical procedures, either alone or with a narcotic.
- It may be administered IV, IM or PO, although IM administration is very painful and hence not recommended.
- It cannot be mixed with other medications or diluted as it carries the risk of precipitation.
Adverse effect:
- Extremely irritating to the tissues
- Venous thrombosis
- Phlebitis
- Apnoea
- Hypotension
- Diazepam can be given orally as a premedication prior to many nonpainful surgical procedures.
- Effective anxiolytic.
Fentanyl:
- Fentanyl is a synthetic opioid. It is indicated for analgesic action short duration procedures.
- If given alone, dosage should begin at 1–2 μg/kg, which is about 75–150 μg for an average size adult.
- Fentanyl has an immediate response and effective excellent analgesia.
- It has a half-life of 2–4 h .
- Rapid IV administration can lead to a rigid chest wall and difficulty in
breathing. This effect may be reversed with naloxone (Narcan)
Dose: 2-4mg/kg
- Fentanyl is used effectively as sedation, adjunct to regional/local
anaesthetics.
- Combined with benzodiazepines, it can obviate the need for inhaled anaesthetics for diagnostic, endoscopic, angiographic and other minor procedures in poor risk patients, as well as for burn dressing.
Ketamine: Dissociative anasthesia
- Ketamine is a nonbarbiturate hypnotic with very high margin of safety. It has good tissue compatibility (no irritation to veins).
- Profound analgesia, immobility, amnesia with light sleep and feelings of dissociation from one’s own body.
DOSE: A dose of 1–3 mg/kg IV (average 1.5 mg/kg) or 6.5–13 mg/kg IM (average 10 mg/kg).
- Ketamine produces the above effects within a minute and recovery start after 10–15 min, but patient remains amnesic for 1–2 h.
- Ketamine is effective for short procedures as operations on head and neck especially in asthmatics.
- It is also useful for repeated use particularly for burn dressings
- Combined with diazepam, it is useful in angiography, cardiac catheterisation and trauma surgery.
Disadvantage:
- Increased intracranial and intraocular pressure with increased occurrence of nausea and vomiting.
Propofol:
- It is the recent IV anaesthetic agent, used for induction/maintenance of anaesthesia.
- Major advantage of propofol is rapid recovery irrespective of the duration of infusion.
Dose
1–2 mg/kg/min (for sedation)
• Possess significant antiemetic property at low doses
• Rapid recovery without hangover effect
• Full orientation returns within 5–10 min
