MOA: binds to antithrombin III thereby potentiating inactivation of thrombin and factors IX, Xa, XI, XII; prevents fibrinogen → fibrin; preferential inactivation of thrombin over other clotting factors
DOSE: Venous thromboembolism: 80 units/kg IV x 1, then 18 units/kg/hour ACS or Afib: 60 units/kg IV x 1, then 12 units/kg/hr
EMERGENT INDICATION: thromboembolism; ACS (enoxaparin preferred for NSTEMI)
WARNINGS: bleeding (protamine may be given for reversal), dosing errors, Preg C
Ensure correct brand is used as there are different formulations with different bioavailabilities. Complex interactions. Always check with existing drugs.
Mode of Action: blocks K efflux (Class III antidysrhythmic); also has Na channel blocking (class I), beta blocking (class II), and Ca channel blocking (class IV) properties.
DOSE: : Pulseless VF/VT: 300mg IV rapid push followed by 150mg IV rapid push if necessary at next pulse check.
Stable wide complex tachycardias: 150mg IV over 10 minutes, followed by infusion of 1mg/min x 6hours, then 0.5 mg/min thereafter.
▪Dependence after 4-6 weeks with a withdrawal syndrome.
▪Long acting metabolites e.g. with Diazepam can give hangover effects.
Interactions:
▪Effects are reversed by Flumazenil but risk of rebound seizure.
▪Caution with other sedative medications.
▪p450 enzyme inhibitors can increase diazepam levels - See BNF/Datasheet.
▪Caution with IM olanzapine.
Dose:
》Anxiety/Sedation : Diazepam 2 mg tds up to 30 mg per day in divided doses.
》Seizures: Diazepam 5-10 mg slow iv (Diazemuls is less irritating). Up to 20 mg may be used with skill and facilities for managing of any respiratory depression.
》Seizures : A PR Diazepam formulation can be used with doses of 2.5 mg/5 mg/10 mg/20 mg as required. Useful when IV access not available or in children.
➡️ Bacteriostatic antibiotics limit the growth of bacteria by interfering with bacterial protein production, DNA replication or other aspects of bacterial cellular metabolism.
They must work together with immune system to remove the micro-organisms from the body. Example:
Tetracyclins
Sulphonamides
Macrolides
Lincosamides
Chloramphenicol
trimethoprim
Most antimicrobial agents in clinical use are bactericidal,
Note that while it is rational to favor bactericidal agents over bacteriostatic agents, neither has ever been shown to be superior (probably because true recovery from infection cannot occur until the body is able to mount an appropriate immune response, thus “buying time” may be just as good as active killing)
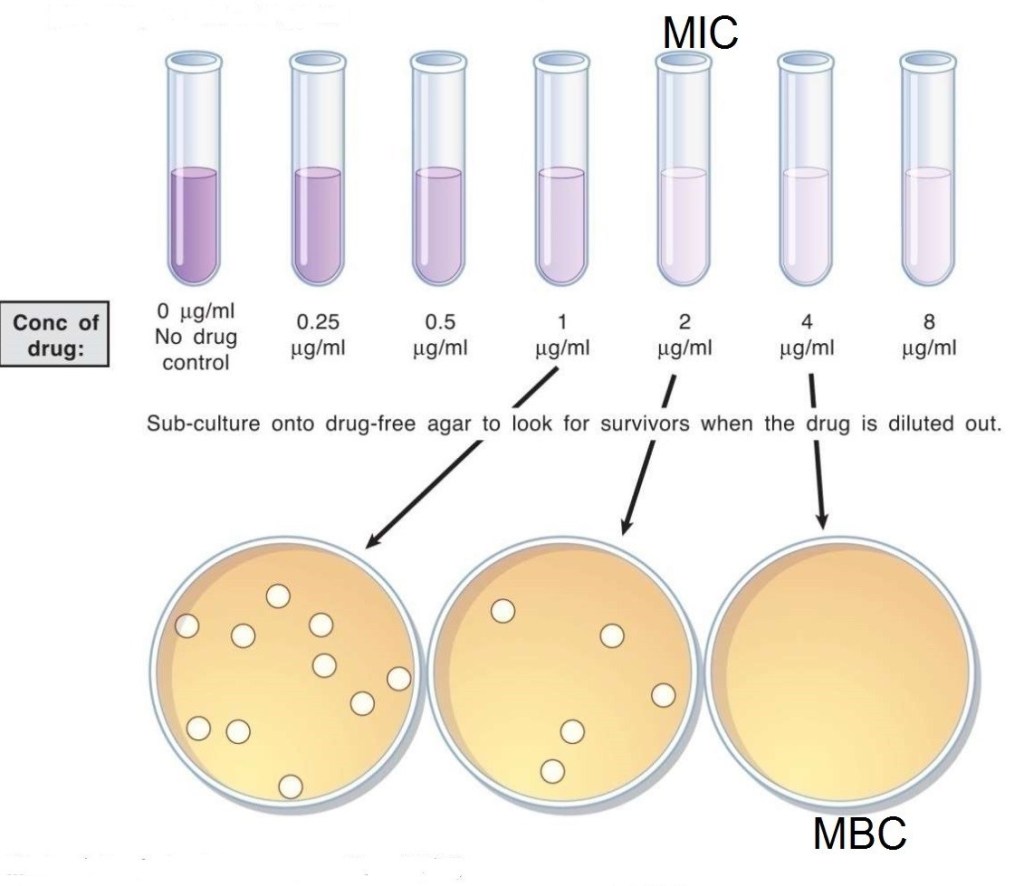
Minimum inhibitory concentration (MIC) versus minimum bactericidal concentration (MBC).
➡️ The MBC is the minimum concentration of drug which can kill the micro-organisms.
➡️ The MIC is the minimum concentration of drug which can inhibit the growth of micro-organisms.
🔷 CHOOSING APPROPRIATE ANTIBIOTIC (A Clinician’s guide to the CARAT criteria)
Council for Appropriate and Rational Antibiotic Therapy (CARAT) criteria for accurate use of antibiotic therapy ● Evidence-based results ●Therapeutic benefits ● Safety ● Cost-effectiveness ● Optimal drug dose and duration —Shorter-course, more aggressive therapy
(i) Evidence-based results:
In choosing an antibiotic, clinicians should consider the clinical evidence demonstrating that the drug is clinically and microbiologically appropriate, the efficacy of that drug in well-designed clinical trials, and the antibiotic resistance patterns of the local region. Clinicians should then use their professional judgment to choose the optimal antibiotic.
(ii) Therapeutic benefits:
If possible, the clinician should identify the causative pathogen and use surveillance data on regional antibiotic resistance patterns in selecting the optimal therapeutic agent.
(iii) Safety:
In treating patients with a particular drug, safety must be weighed against efficacy. Clinically applicable treatment strategies should be chosen to maximize efficacy while minimizing side effects.
(iv) Optimal drug for optimal duration:
Optimal drug selection requires finding the antimicrobial class and the specific member of that class that is best suited to treat a particular infection. Because empiric therapy is necessary in most cases, multiple factors have to be considered. Among these are whether the etiologic agent is likely to be gram-positive or gram-negative, whether a narrow or broad-spectrum agent should be chosen, the resistance patterns of the likely pathogen to this drug, both nationally and regionally, and the individual patient’s medical history, including recent antibiotic exposure.
Optimal duration means prescribing the selected drug for the shortest amount of time required for clinical and micro- biologic efficacy. There are many reasons for reducing an- timicrobial therapy to the shortest appropriate duration. They include the potential for reduced occurrence of adverse effects, increased patient adherence, decreased promotion of resistance, and decreased costs.
(v) Cost-effectiveness:
Choosing inappropriate therapy is associated with increased costs, including the cost of the antibiotic and increases in overall costs of medical care because of treatment failures and adverse events.