Gingivectomy means excision of the gingiva. By removing the pocket wall, gingivectomy provides visibility and accessibility for complete calculus removal and thorough smoothing of the roots, creating a favorable enviornment for gingival healing and restoration of a physiologic gingival contour.
Indications:
Elimination of suprabony pockets, regardless of their depth, if the pocket wall is fibrous & firm.
Elimination of gingival enlargements
Elimination of suprabony periodontal abscesses.
Contraindications:
The need for bone surgery
Situations in which the bottom of the pocket is apical to the mucogingival junction.
Esthetic consiserations, particularly in the anterior maxilla.
SURGICAL GINGIVECTOMY
Armamentarium:
Mouth mirror, probe
Pocket markers, Kirkland and orban interdental gingivectomy knives
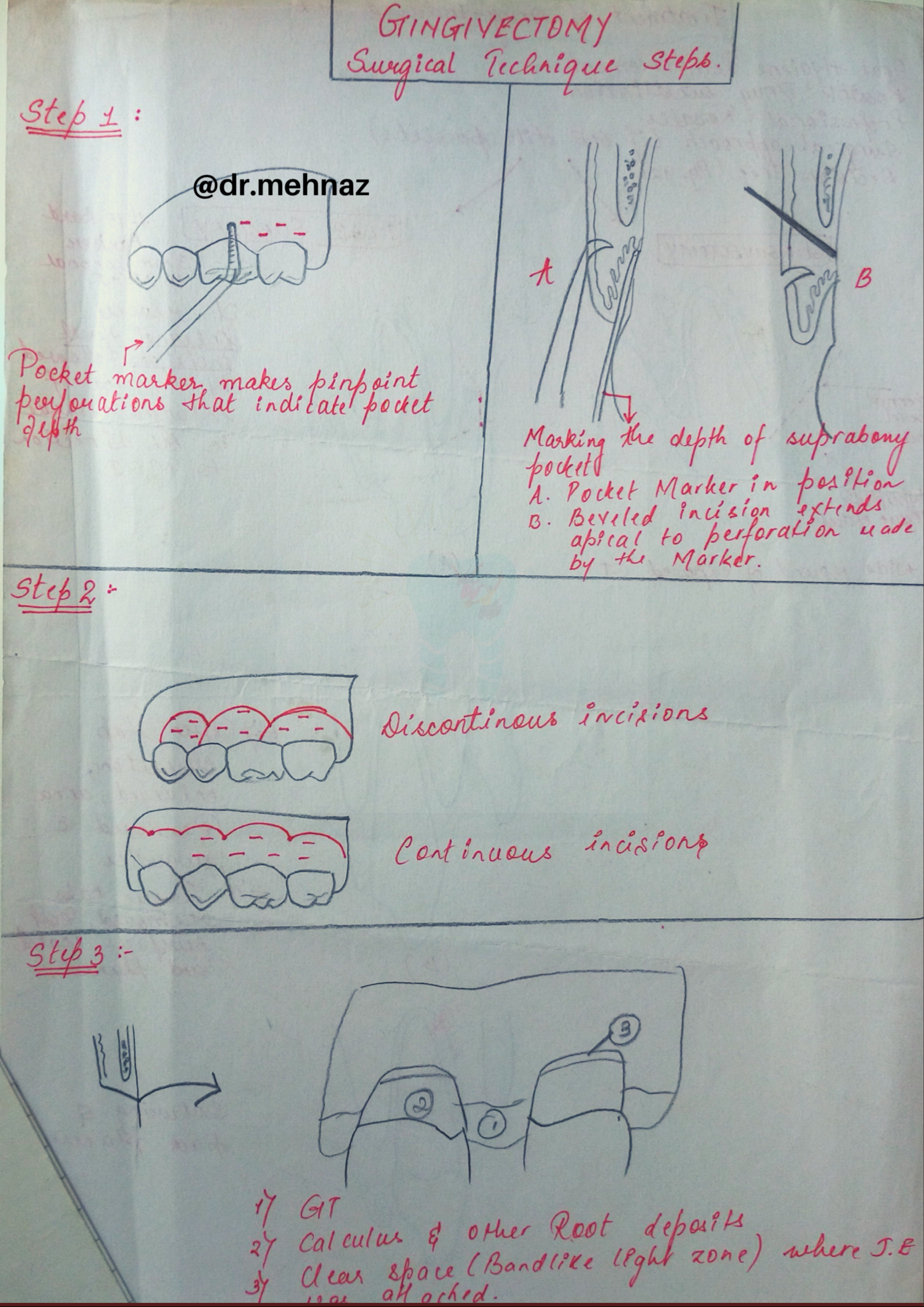
Step 1: The pockets on each surface are explored with a periodontal probe and marked with a pocket marker.
Step 2: The incision is started apical to the points marking the course of the pockets and is directed coronally to a point between the base of the pocket and the crest of the bone.
Step 3: Remove the excised pocket wall, clean the area, and closely examine the root surface.
Step 4: Carefully curette the granulation tissue, and remove any remaining calculus and necrotic cementum so as to leave a smooth & clean surface.
Presentation Tip💡: Try to present your answers with flowcharts & diagrams rather than long paragraphs!! It will definitely have more impact & help you score well in exams..👍👇🏻
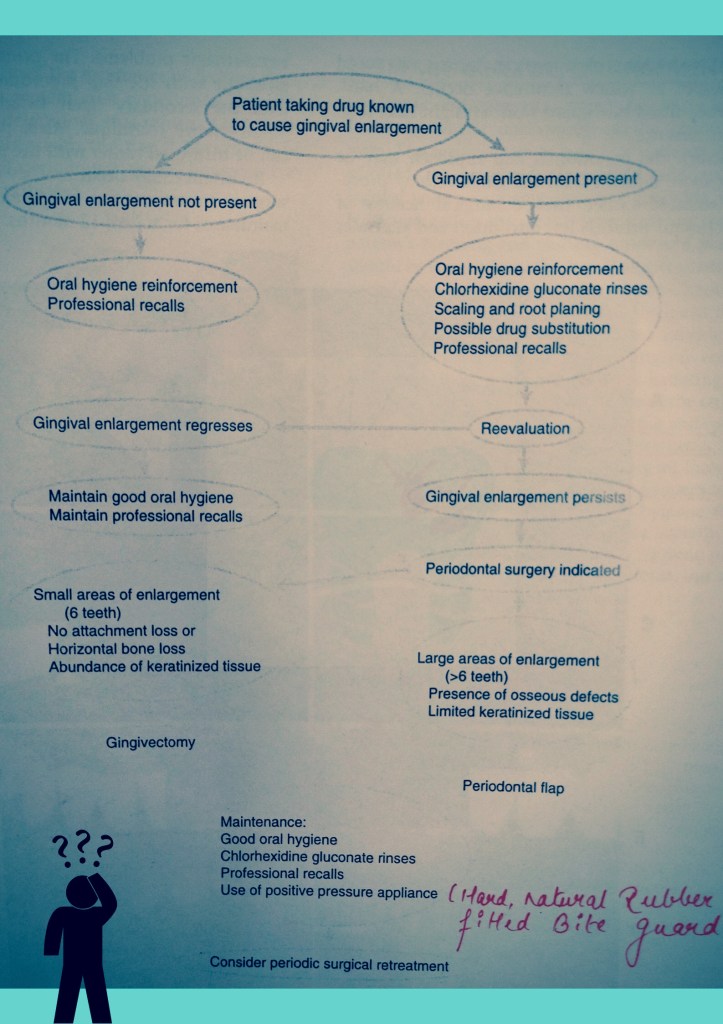
Surgical Approach (Diagrammatic View); MGJ: Muco-gingival junction; BL: Bucco-lingual; CT: Connective TissueDecision Tree fortreatment of Drug-Associated Gingival Enlargement
Source: Carranza’s Clinical Periodontolgy, 10th Ed
It is a natural Fibrin-based biomaterial prepared from autologous blood and is clinically used to deliver growth factors in high concentration to the site having a bone defect or requiring augmentation.
It is introduced by Dr. Choukroun. et. Al, 2000. It is a second generation platelet concentrate that contains platelets and growth factors, prepared from self blood devoid of anticoagulant or other artificial modifiers.
Preparation
10ml of human blood is taken in a test-tube without any anticoagulant and is centrifuged in a tabletop centrifuge machine for 12 minutes at 2500RPM or 10 minutes at 3000RPM.
After centrifugation, the three components in the blood are localised in the test tube.
Red blood cells (at bottom)
A Fibrin clot (in middle)
Plasma (at top)
Fibrin clot is extracted from the test-tube with a pair of sterile forceps and PRF is obtained by removing the red clot from its lower end.
Crevicular fluid is a serum ultrafiltrate that accumulates in gingival connective tissue resulting from increased vascular permeability. When its production increases, it passes to the gingival crevice.
Gingival crevicular fluid contains products derived from microbial plaque, tissue breakdown, host cells, and host immunity that, in some instances, have been demonstrated to be related to the active phases of periodontal destruction.
Aspartate aminotransferase (AST) is an enzyme normally confined to cell cytoplasm, but is released to the extracellular environment upon damage. AST levels in serum and other body fluids ( cerebrospinal fluid, arthritic joint fluids) have been used for several decades as a laboratory diagnostic aid for assessing tissue destruction (i.e.MI, hepatitis). Furthermore, the amount of AST activity observed generally reflects the extent of cell death and, consequently, the magnitude of tissue destruction. AST activity greatly depends on cellular damage in periodontal tissues. Levels of various inflammatory cytokines can also be determined in GCF.
The periimplant gingival sulci has been shown to be similar to the periodontal crevice with respect to gingival fluid flow. In spite of this observation, to date relatively few studies have focused their attention on the investigation of the periimplant crevicular fluid (PCF) components and their relationship with the peri-implant condition.
Functions of GCF:
• Promotes adhesion of the gingival crevice epithelium to the enamel through the presence of salivary and plasma proteins. • Defense through the presence of inflammatory cells and molecules. • Elimination of micro-organisms and food debris through the washout effect of fluid formation.
Muhad Noorman P, Final year Student – Team Dentowesome
Scoring good and better marks are always priority of any student irrespective of their level and class . Hard work and smart work helps to score good marks.
Some tips to study smart and score more marks
1) Always organise yourself, Neverprocrastinate. Don’t think about wasted days ,look forward days ahead and make efficient planning.
2) Give importance to every subject equally, start with easy and end in hard nuts.
3) Identify your best time, and place to study. Ignore and never seek how you’re peer group works. Always your peer lies about studies, focus on yourself 🙂
4) Cut your social distraction, even though it sounds like a rocket science, regular practice helps to cut your Distraction. Utilise focus mode in android phones, Install Forest app. It Helps to prioritise your study hours.
5) Teach yourself as if you’re a teacher, trust me you’ll crack a million topics.
6) Teach you’re peer group , it’ll help to recollect and brush up your brain.
7) Regularly shift your studyplace , between a period of 1 hour or 2 hour later, brain and mind always rejects learning from a same environment.
8) Get familiarise with the exam layout, use previous year question, understand nature of questions , prepare accordingly.
9) Always finish with previous questions first and if time allows study other topic left, mentioned in University syllabus.
10) Reading a book not studying : Revise topic after 1 or 2 hour, Prepare notes, put away books . Attempt topic as an exam question. Self realization is best methodology to improve yourself.
11) Never cut too many corners: Often we get devastated listening rumors , predictable questions . And the truth is anything can come.
12) Practice mock exams during free times. Practice always make a man perfect.
13) Organize your answer while writing in exam papers. Never forget, Presentation matters. Include as much as figures, flowcharts, pie diagrams..etc.. Proove examiner you have an edge over topics. Underline important points with seperate ink.
14) Last but not least get an adequatesleep.(Ideally 6 to 7 hours) Give some time for your brain and hippocampus to process your memory.
These are incorporated into the deeper layers of enamel and dentin during odontogenesis and alter the development and appearance of the enamel and dentin
.Alkaptonuria: Dark brown pigmentation of primary teeth is commonly seen in alkaptonuria. It is an autosomal recessive disorder resulting into complete oxidation of tyrosine and phenylalanine causing increased level of homogentisic acid.
Hematological disorders
• Erythroblastosis fetalis: It is a blood disorder of neonates due to Rh incompatibility. In this, stain does not involve teeth or portions of teeth developing after cessation of hemolysis shortly after birth. Stain is usually green, brown or bluish in color.
• Congenital porphyria: It is an inborn error of por- phyrin metabolism, characterized by overproduction of uroporphyrin. Deciduous and permanent teeth may show a red or brownish discoloration. Under ultraviolet light, teeth show red fluorescence.
• Sickle cell anemia: It is inherited blood dyscrasia characterized by increased hemolysis of red blood cells. In sickle cell anemia infrequently the stains of the teeth are similar to those of erythroblastosis fetalis, but discoloration is more severe, involves both dentitions and does not resolve with time.
Amelogenesis imperfecta: It comprises of a group of conditions, that demonstrate developmental alteration in the structure of the enamel in the absence of a systemic disorders. Amelogenesis imperfecta (AI) has been classified mainly into hypoplastic, hypocalcified and hypomaturation type.
Fluorosis: In fluorosis, staining is due to excessive fluoride uptake during development of enamel. Excess fluoride induces a metabolic change in ameloblast and the resultant enamel has a defective matrix and an irregular, hypomineralized structure
Vitamin D deficiency results in characteristic white patch hypoplasia in teeth.
Vitamin C deficiency together with vitamin A deficiency during formative periods of dentition resulting in pitting type appearance of teeth.
Childhood illnesses during odontogenesis, such as exanthematous fevers, malnutrition, metabolic disorder, etc. also affect teeth.
Dentinogenesis imperfecta : It is an autosomal dominant development disturbance of the dentin which occurs along or in conjunction with amelogenesis imperfecta. Color of teeth in dentinogenesis imperfecta (DI) varies from gray to brownish violet to yellowish brown with a characteristic usual translucent or opalescent hue.
Tetracycline and minocycline: Unsightly dis- coloration of both dentitions results from excessive intake of tetracycline and minocycline during the development of teeth. Chelation of tetracycline molecule with calcium in hydroxyapatite crystals forms tetracycline orthophosphate which is responsible for discolored teeth.
Posteruptive Causes
Pulpal changes: Pulp necrosis usually results from bacterial, mechanical or chemical irritation to pulp. In this disintegration products enter dentinal tubules and cause discoloration.
Trauma: Accidental injury to tooth can cause pulpal and enamel degenerative changes that may alter color of teeth.Pulpal hemorrhage leads to grayish discoloration and nonvital appearance. Injury causes hemorrhage which results in lysis of RBCs and liberation of iron sulfide which enter dentinal tubules and discolor surrounding tooth.
Dentin hypercalcification: Dentin hypercalcification results when there are excessive irregular elements in the pulp chamber and canal walls. It causes decrease in translucency and yellowish or yellow brown discoloration of the teeth.
Dental caries: In general, teeth present a discolored appearance around areas of bacterial stagnation and leaking restorations.
Restorative materials and dental procedures: Discoloration can also result from the use of endodontic sealers and restorative materials.
Aging: Color changes in teeth with age result from surface and subsurface changes. Age related discoloration are because of:– Enamel changes: Both thinning and texture changes occur in enamel.
– Dentin deposition: Secondary and tertiary dentin deposits, pulp stones cause changes in the color of teeth.
• Functional and parafunctional changes: Tooth wear may give a darker appearance to the teeth because of loss of tooth surface and exposure of dentin which is yellower and is susceptible to color changes by absorption of oral fluids and deposition of reparative dentin.
Extrinsic Stains
Daily Acquired Stains
Plaque: Pellicle and plaque on tooth surface gives rise to yellowish appearance of teeth.
Food and beverages: Tea, coffee, red wine, curry and colas if taken in excess cause discoloration.
Tobacco use results in brown to black appearance of teeth.
Poor oral hygiene manifests as:
– Green stain
– Brown stain
– Orange stain.
Swimmer’s calculus: – It is yellow to dark brown stain present on facial andlingual surfaces of anterior teeth. It occurs due toprolonged exposure to pool water.
Gingival hemorrhage.
Chemicals
• Chlorhexidine stain: The stains produced by use of chlorhexidine are yellowish brown to brownish in nature.
Metallic stains: These are caused by metals and metallic salts introduced into oral cavity in metal containing dust inhaled by industry workers or through orally administered drugs.
Stains caused by different metals
• Copper dust—green stain • Iron dust—brown stain • Mercury—greenish black stain • Nickel—green stain • Silver—black stain.
Reference- Nisha garg textbook of endosontics and Anil Ghom textbook of oral medicine
iiHematological disorders iii. Disease of enamel and dentin
iv. Liver diseases.– Medications i. Tetracycline stains and other antibiotic use
ii. Fluorosis stain.
• Posteruptive causes of discoloration– Pulpal changes – Trauma – Dentin hypercalcification – Dental caries – Restorative materials and operative procedures – Aging – Functional and parafunctional changes.
Extrinsic stains • Daily acquired stains
– Plaque – Food and beverages – Tobacco use – Poor oral hygiene – Swimmer’s calculus – Gingival hemorrhage.
Chemicals – Chlorhexidine
– Metallic stains.
2.Classification of extrinsic stains (Nathoo in 1997)
• N1 type dental stain (direct dental stain): Here colored materials bind to the tooth surface to cause discoloration. Tooth has same color, as that of chromogen.
• N2 type dental stain (direct dental stain): Here chromogen changes color after binding to the tooth.
• N3 type dental stain (indirect dental stain): In this type prechromogen (colorless) binds to the tooth and undergoes a chemical reaction to cause a stain.
3.Different Types of Stains according to Color:
BLACK COLOR-
It usually results due to contact with certain metallic elements such as silver, iron and lead.It may appear as thin line running approximately 1 mm or so above the gingival margin, it may occur on both the facial and lingual surfaces of teeth.Stain is firmly attached to the surface but remains extrinsic, thus it may be removed by brush and abrasives. But, it recurs later on.
Green stain
It usually occurs as thick deposit involving the cervical one-third of facial surface of maxillary incisors of young children. It affects boys more frequently than girls.
It is associated with poor oral hygiene and decalcification is sometimes present in enamel, underlying the deposit. It occurs due to chromogenic bacteria or fungi or it may be caused by bacterial action on remnants of enamel cuticle. It is extrinsic and may be removed by simple brushing and abrasive.
Orange stain
It occurs infrequently and usually involve both facial and lingual surfaces of the incisors. It is easily removed than green stain and its cause is unknown but it is believed to be the result of chromogenic bacteria. It is associated with poor oral hygiene and removed with the help of brush and abrasives.
Brown stain
It can be seen in non-smokers and is usually lighter brown than that of tobacco and form a tenacious, but delicate film on surface of the teeth. It is usually seen more commonly on lingual surface of lower incisors and buccal surface of maxillary molar teeth. It is formed due to altered salivary mucins which have undergone change through the action of bacterial enzymes.
REFERENCE- NISHA GARG TEXTBOOK OF ENDODONTICS AND ANIL GHOM TEXTBOOK OF ORAL MEDICINE