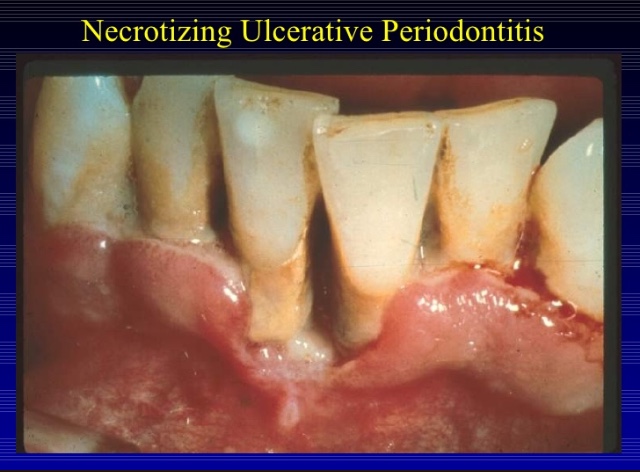
⦿ Necrotizing ulcerative periodontitis may be an extension of necrotizing ulcerative gingivitis into the periodontal structures, leading to periodontal attachment and bone loss.
⦿ It is characterized by soft tissue necrosis, rapid periodontal destruction, and inter-proximal bone loss.
RISK FACTORS:
- Immunosuppressed patients; HIV- +ve with CD4 count <200 is more strongly associated with NUP.
- Severe malnutrition
- Smoking
- Poor oral hygiene
- Stress
- Sequela of necrotizing ulcerative gingivitis.
CLINICAL PRESENTATION:
POPULATION:
⦿ Usually: young adults(age 18-30); sometimes: malnourished children or immunocompromised individuals.
Symptoms: Intense, excruciating pain
SIGNS:
⦿ Similar to NUG, clinical cases of NUP are defined by necrosis and ulceration of the coronal portion of the interdental papilla and gingival margin, with a painful bright red marginal gingiva that bleeds easily.
⦿ Severe loss of periodontal attachment.
⦿ Deep interdental osseous craters typify periodontal lesions of NUP.
⦿ Deep pocket formation is not evident because the ulcerative and necrotizing nature of the gingival lesion destroys the marginal epithelium and connective tissue, resulting in gingival rescession.
⦿ Advanced lesions lead to severe bone loss, tooth mobility and ultimately tooth loss.
⦿ Oral malodor, fever, malaise or lymphadenopathy may occur.
⦿ Characteristic microbiota: fusiform bacteria, P Internedia, P gingivalis, Treponema sp., and C.Albicans.
HIV/AIDS Patient:
⦿ Linear gingival erythema, NUG and NUP are the most common HIV- associated periodontal conditions.
⦿ NUP lesions in AIDS patients can be much more destructive and frequently result in complicatons that are extremely rare in non AIDS patient.

HIV POSITIVE NUP:
⦿ PRESENTATION:
⦿ Periodontal attachment and bone loss may be extremely rapid.
⦿ Progression of the lesions to involve large areas of soft tissue necrosis, with exposure of bone and sequestration of bone fragments.
⦿ This type of severe, progressive lesion with extension into the vestibular area and the palate is referred to as necrotizing ulcerative stomatitis.
INVESTIGATION:
⦿ Obtain a detailed M/H, including nutrition and health habits.
⦿ Medical consult to rule out any immunosuppressive disease may be necessary. NUP has been associated with HIV+ve and AIDS patient.
⦿ Obtain a dental history: previous history of NUG/periodontal disease., foul metallic taste, pasty saliva, intense excruciating pain.
⦿ Perform an extraoral examination: check for lymphadenopathy in the head and neck, facial asymmetry.
⦿ Perform an intraoral examination: look for C/F of NUP.
DIFFERENTIAL DIAGNOSIS:
- Acute herpetic gingivostomatitis
- Desquamative gingivitis
- Agranulocytosis
- Leukemia
- Noma
- Necrotizing stomatitis
- Chronic periodontitis
TREATMENT:
⦿ Common initial treatments:
- Perform debridement under local anesthesia, including gentle scaling.
- Remove pseudomembrane, using cotton pellet dipped in 0.12% chlorhexidine.
- Provide the patient with oral hygiene instructions and prescribe antibacterial mouthwash.
- Tell the patient to control pain with analgesics.
- Provide patient counseling: ensure proper nutrition, take vitamin supplements, avoid spicy foods, adopt appropriate fluid intake, increase sleep, decrease stress, and quit smoking, if possible.
- Prescribe antibiotics if signs of systemic involvement.
- If the patient is immunocompromised, it is important to follow up with their physician when you prescribe antibiotics. The risk of super infection with oral candida must be considered when using systemic antibiotics in immunocompromised patients. In those cases anti-fungal medication might be needed.
FOLLOW UP
- Depending on the degree of immunosupression, it may be advisable to perform only conservative, minimally invasive procedures and monitor them closely.
- Assess treatment outcomes in 24 hours, then every other day until all acute signs and symptoms are controlled. Frequent periodontal maintenance visits and meticulous oral hygiene are necessary as NUP may continue to progress rapidly.
- After the first consult or control of the acute stage, referral to a periodontist or oral surgeon is advised.
- Follow up with a comprehensive periodontal evaluation.
References: Essentials Of Periodontology by S Sahitya Reddy; Carranza’s clinical periodontology; Internet images



