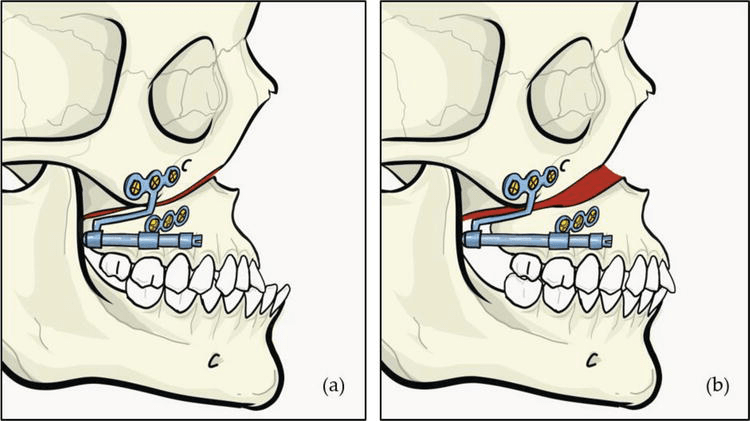
If you’ve ever had a conversation with an orthodontic or maxillofacial surgeon, you’ve probably heard the term “Le Fort I osteotomy” thrown around like it’s a casual brunch topic. But don’t worry—this isn’t some medieval torture technique (though patients might beg to differ post-op). It’s actually a routine and life-changing surgical procedure used to correct conditions like vertical maxillary excess, midface hypoplasia, and anterior open bite. Basically, it’s the orthodontic equivalent of upgrading from a flip phone to a smartphone—function meets aesthetics in the best way possible.
As surgeons started routinely repositioning the maxilla in the late ’70s, they noticed something peculiar—some patients who had undergone cleft palate repairs started experiencing changes in their speech post-surgery. And not just a “my voice sounds weird on a voicemail” kind of change, but significant alterations that could be temporary or, in some cases, permanent. This led to an influx of studies trying to figure out exactly what was happening and why. Because let’s face it, no one signs up for surgery expecting to sound like they just inhaled helium for life.
The Root of the Problem: It’s All About the Muscles (and Scars)
Speech issues in cleft patients boil down to a mix of developmental malformations, scarring, and structural obstacles in the oral and pharyngeal regions. Picture a team of musicians where half the instruments are missing, and the rest are playing in the wrong key—yeah, not great for clear articulation. The muscles involved in lifting the soft palate (like the levator veli palatini) and their antagonists (like the palatoglossus) often develop improperly, leading to speech challenges. Add in post-surgical scar tissue, oronasal fistulas, and crossbites, and you have a recipe for some serious phonetic acrobatics.
VPI: When Airflow Has a Mind of Its Own
One of the biggest speech-related concerns in cleft patients is velopharyngeal insufficiency (VPI)—a fancy way of saying the velum (soft palate) and pharyngeal wall aren’t sealing off the nasopharynx properly during speech. This results in excess air escaping through the nose, making speech sound overly nasal, like someone permanently stuck in the middle of a bad cold. On the flip side, some patients with severe midface deficiency develop hyponasality, where the nasal passage is too blocked, making them sound like they have a clothespin on their nose.
Then there are articulation defects, where certain consonants refuse to cooperate. Think of sibilants (like ‘s’ and ‘sh’), fricatives (like ‘f’ and ‘v’), and plosives (like ‘p’ and ‘b’) suddenly staging a rebellion. These errors can result from anatomical misalignment, making the production of crisp, clear sounds a daily challenge.
So, What Does Surgery Actually Do to Speech?
Studies have tried to pin down exactly how maxillary surgery impacts speech, but results have been all over the place—partly because speech is complicated and partly because patient samples have been small and assessment methods inconsistent. However, some trends are clear:
- Maxillary advancement can improve speech for some patients by providing better tongue space and articulation.
- Others may experience temporary speech regression as their muscles adjust to the new positioning.
- For cleft patients with pre-existing VPI, surgery might actually worsen velopharyngeal function, requiring additional speech therapy or even secondary surgeries.
📊 Study Breakdown: The Who, What, and How
👥 Patients: The Speech Test Subjects
| Total Patients Enrolled | 80 |
|---|---|
| Patients with Complete Data | 54 |
| Gender Distribution | 37 Male, 17 Female |
| Age Range at Surgery | 8 – 33 years |
💡 Fun Fact: Speech evaluations were taken anywhere from 3 months to 6 years post-op—because, let’s face it, speech takes its sweet time adjusting.
🛠️ Surgery Types: The Maxillary Makeover
| Surgical Procedure | Patients (n=54) |
|---|---|
| Le Fort I Advancement Only | 34 |
| Le Fort I + BSSO (Mandibular Setback) | 20 |
💬 Translation: 34 patients got a one-way ticket to maxillary forward town, while 20 had their mandible set back to balance the whole look. 😁
🗣️ Speech Evaluation: The Verbal Verdict
To keep things scientific (but still understandable), speech was assessed using a system developed in 1979 by McWilliams and Phillips at the University of Pittsburgh. And yes, it’s been around longer than most of us.
🔎 What Was Measured?
1️⃣ Hypernasality (aka the unintentional nose filter)
- Scored from 0 (normal) to 4 (severe hypernasality)
2️⃣ Hyponasality (think: permanently stuffed nose sound)
- Rated as: 0 = none, 2 = moderate/severe
3️⃣ Articulation Errors 🎙️
- Measured in sibilants, fricatives, and plosives (aka the sounds that make or break clear speech)
4️⃣ Velopharyngeal Valve Function 🚪
- Classified as:
- 0 = Normal
- 1-2 = Borderline competent
- 3-6 = Borderline incompetent
- 7+ = Incompetent (oops…)
📉 Speech Score Breakdown
| Speech Score | VP Valve Status |
|---|---|
| 0 | Normal 🟢 |
| 1-2 | Borderline competent 🟡 |
| 3-6 | Borderline incompetent 🟠 |
| 7+ | Incompetent 🔴 |
💡 The Big Question: Did the surgery help or hurt speech? Well…
- Some patients improved 🎉
- Some stayed the same 🤷♂️
- And a few had new speech issues 🤦♀️
📉 Speech at 3 Months Post-Surgery: The Plot Thickens
The biggest shocker? A general decline in velopharyngeal competence. Before surgery, 42% of patients had normal VP function. Three months later? Just 18%! 🚨
🔍 VP Mechanism Changes Post-Surgery
| VP Status | Pre-Surgery (%) | Post-Surgery (%) |
|---|---|---|
| Competent 🟢 | 42% (23) | 18% (10) |
| Borderline Incompetent 🟡 | 9% (5) | 22% (12) |
| Complete VPI 🔴 | 13% (7) | 20% (11) |
💬 Translation: Speech went from “I got this” to “Houston, we have a problem.” 🚀
Overall speech scores? Worse. 😬
- Pre-surgery average: 2.46
- Post-surgery average: 4.24
- And yes, it was statistically significant (P < .05).
🎤 Articulation: A Silver Lining?
Not all was lost! Articulation defects—like trouble with fricatives, plosives, and sibilants—actually improved slightly.
| Articulation Defects | Pre-Surgery (%) | Post-Surgery (%) |
|---|---|---|
| Any Speech Defect | 84% (46) | 73% (40) ✅ |
| Errors Related to Anterior Dentition | 64% (35) | 47% (26) ✅ |
💡 Moral of the story? If you’re struggling with anterior sounds before surgery, you might get a speech upgrade. But if your VP function is already on the edge… buckle up.
🔄 Hypernasality vs. Hyponasality: The Great Speech Shuffle
One of the quirks of Le Fort I advancement? Some patients swap speech issues like a game of Uno. 🎭
| Speech Condition | Pre-Surgery (n) | Post-Surgery (n) |
|---|---|---|
| Hyponasality (Stuffed Nose Sound) | 18 | 8 ✅ |
| Mild Hypernasality (Nasal Twang) | 10 | 16 ❌ |
| Moderate Hypernasality | 2 | 8 ❌ |
| Severe Hypernasality | 2 | 1 ✅ |
🔄 So if you went in sounding blocked, there’s a chance you walked out with a bit too much air coming through instead!
👥 Does the Type of Surgery Matter?
Group 1: Le Fort I Only
- Pre-surgery articulation defects: 88% 🗣️
- Post-surgery: 74% ✅
Group 2: Le Fort I + BSSO (Mandibular setback included)
- Pre-surgery articulation defects: 75%
- Post-surgery numbers cut off (sorry, suspense lovers!)
👉 Moral of the story? It doesn’t seem to matter if you just advance the maxilla or combine it with a mandibular setback—speech still takes a hit!
🔬 Pharyngeal Flaps: Helping or Hurting?
18 patients had a pharyngeal flap before surgery. Here’s how they fared:
- 9 got worse 😵
- 8 stayed the same 🤷
- 1 got better 🎉
Not exactly an inspiring success rate.
📖 The Great Speech Debate: Who Said What?
Team “Maxillary Advancement Worsens VPI” 🚨
- Schwartz & Gruner (1980s): 84% of cleft patients had worse velopharyngeal function at 4 months post-op. 😬
- Mason et al. (1980): Cleft patients are at higher risk of hypernasality due to their unique anatomy.
- Witzel (1990s): If you were borderline VPI before surgery, you’re at major risk afterward.
🔎 Translation? If your velopharyngeal valve was iffy before surgery, it might throw in the towel afterward.
Team “Speech Stays the Same (or Improves)!” 🎉
- McCarthy et al. (1980s): No increase in VPI, but yes, articulation changed.
- Dalston & Vig (1984): No articulation improvement (speech therapists, you can relax).
- Witzel et al. (University of Pittsburgh, 1990s): Dental occlusion affects articulation, and correcting the bite can help!
- Ruscello et al. (1990s): 85% of patients with pre-op articulation defects improved within 6 months.
- Vallino (1987): 88.2% of patients saw speech improvements post-op.
🔎 Translation? If your main issue is articulation errors from a bad bite, then surgery could be your speech therapist in disguise.
💥 What Happened in This Study?
Our 54-patient study found:
1️⃣ More patients developed borderline incompetence or full-blown VPI post-op 🤦
2️⃣ Reduced intraoral air pressure made sibilants, fricatives, and plosives harder to pronounce
3️⃣ Velar closure during speech became incomplete, leading to nasal air leakage
So, we’re leaning toward maxillary advancement potentially worsening VP function. But does this mean doom for all cleft patients? Not necessarily!
🎭 The Balancing Act: Beauty vs. Speech?
🦷 Pros of Le Fort I Advancement:
✅ Better bite & occlusion 🦷
✅ Improved articulation (for some) 🎤
✅ Aesthetically pleasing results ✨
🚨 Cons of Le Fort I Advancement:
❌ Higher risk of hypernasality 🗣️
❌ VPI might worsen (especially in cleft patients) 😷
❌ Some sounds (like “s” and “p”) might become trickier
🤔 So, Should We Be Worried?
Not necessarily! Here’s what to consider:
🔹 If your velopharyngeal function is already borderline, be cautious.
🔹 If you have articulation issues from malocclusion, surgery might help!
🔹 Speech therapy post-op can help retrain articulation and airflow.
🎤 The Curious Case of Pharyngeal Flaps
If you’re one of the lucky 18 who had a pharyngeal flap before maxillary advancement, congratulations! 🎉
💡 Key Findings for Pharyngeal Flap Patients:
👉 50% of them improved or retained their pre-surgical speech function.
👉 67% were already in the “competent or borderline competent” speech category pre-op.
👉 Hyponasality cases dropped. (Since advancing the maxilla opened things up.)
🎯 Moral of the story? If you’re prone to VPI, a pharyngeal flap might be your best friend before Le Fort I surgery. But don’t rush into it post-op! Give it at least a year before considering further surgery.
🤔 To Advance or Not to Advance?
Maxillary advancement surgery is a balancing act—you win in aesthetics & occlusion but might lose a bit in speech function. 😵💫
👑 Winners:
✔️ People with articulation errors from a bad bite (Your “s” sounds are about to get crisp! 🍏)
✔️ Those suffering from hyponasality (Breathing free at last! 😮💨)
🚨 Potential Strugglers:
❌ Patients already borderline for VPI (Things might get worse. 🙈)
❌ Those at risk for hypernasality (Your voice might sound like it’s permanently in helium mode. 🎈)
💡 Final Take: Speech vs. Surgery – Who Wins?
Le Fort I is like buying a new, expensive phone—better features, but you might drop a few calls (aka speech issues). 📱📉
👂 Key Takeaways:
1️⃣ Articulation = Likely to improve.
2️⃣ Hypernasality = May get worse.
3️⃣ VPI = Can be a concern, especially for cleft patients.
4️⃣ Pharyngeal flaps = Might help, but timing is key!