1. Why is the inter-incisor angle critical to stability in Class II div 2?
- Class II div 2 has increased inter-incisor angle
- Excessive angle → deep overbite and mandibular locking
- Normalizing angle:
- Reduces vertical overlap
- Allows lower incisors to sit in zone of balance
- Palatal torque of upper incisors is essential
- If angle is not corrected → lower incisors relapse
Viva punchline:
👉 Stable overbite correction depends on normalization of the inter-incisor angle.
2. Why doesn’t lower incisor advancement relapse?
- Relapse occurs only if teeth move outside muscular envelope
- Lower incisors are advanced:
- Within lower lip contour
- Not beyond soft-tissue limits
- Simultaneous:
- Upper incisor intrusion
- Palatal torque
- This unlocks the mandible
- New incisor position becomes physiologic
Viva punchline:
👉 Because the lower incisor is advanced within the soft-tissue envelope.
3. Why is flattening the curve of Spee essential?
- Class II div 2 → exaggerated curve of Spee
- Lower incisor advancement creates:
- ~4–5 mm space anteriorly
- ~8–10 mm total
- ~2 mm per side used for:
- Flattening curve of Spee
- Remaining space used for alignment
- Flattening is part of correction, not space loss
Viva punchline:
👉 Curve of Spee flattening enables non-extraction treatment.
4. Why upper removable appliance first?
- Achieves multiple goals simultaneously:
- Bite opening
- Upper incisor palatal torque
- Buccal segment distalization
- Correction of scissor bite
- Upper incisor intrusion
- Frees mandible from locked position
- Fixed appliance alone cannot do this efficiently
Viva punchline:
👉 Upper removable appliance provides coordinated first-phase correction.
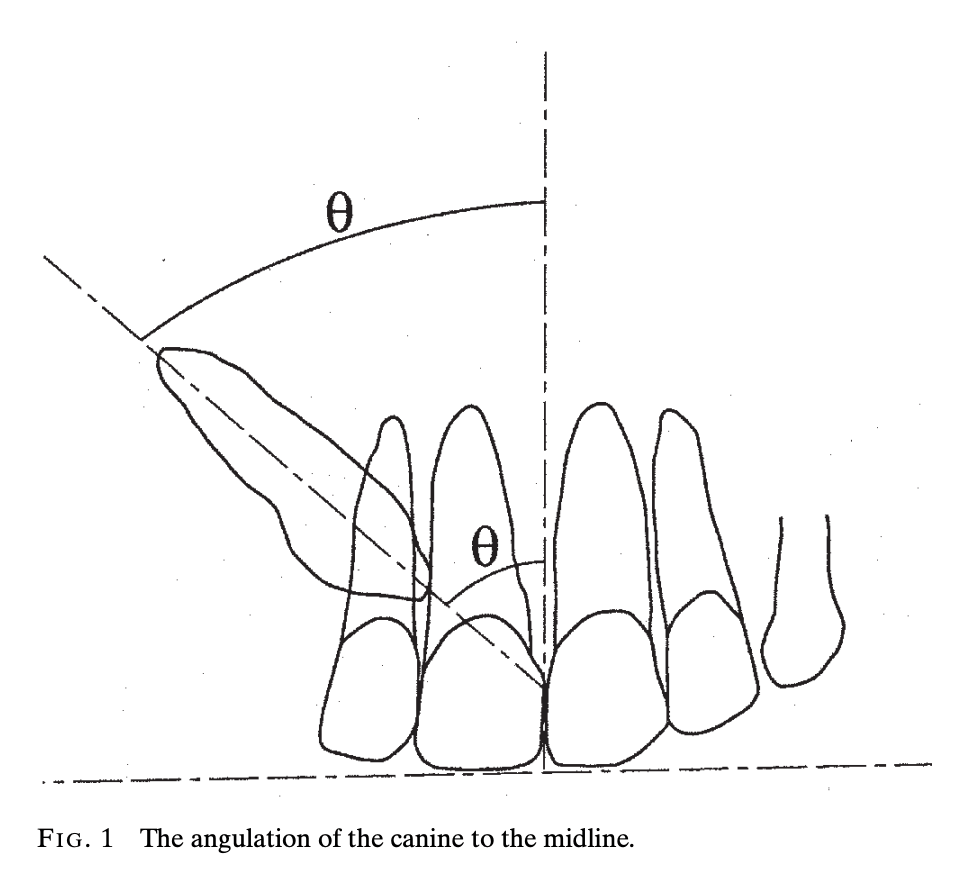
5. Importance of upper incisor centroid
- Centroid = midpoint of incisor root
- Helps assess:
- Root position
- Torque control
- Lower incisor tip position relative to centroid determines:
- Inter-incisor angle
- Stability
- Lower incisor behind centroid → unstable
- Slightly ahead → stable relationship
Viva punchline:
👉 Centroid guides stable inter-incisor positioning.
6. When to extract? Why not first premolars?
- Extractions only if:
- Severe skeletal discrepancy
- Inadequate space after leveling
- First premolar extraction:
- Compromises buccal segment correction
- Second premolars preferred:
- Maintain Class I molar correction
- Decision after therapeutic diagnosis
Viva punchline:
👉 Extraction decisions are delayed and conservative in Class II div 2.
7. Why long-term lower bonded retainer?
- Lower anterior relapse is unpredictable
- Tight perioral musculature common
- Lower anterior segment is foundation of correction
- Bonded retainer:
- Maintains AP and transverse position
- Stable lower incisors support upper incisors
- Upper arch often needs minimal retention
Viva punchline:
👉 Lower bonded retainer ensures long-term stability.
8. Role of upper incisor–lip relationship
- Upper incisor should:
- Contact inner slope of lower lip
- Show 2–3 mm at rest
- Defines soft-tissue boundary
- Dictates:
- Amount of intrusion
- Palatal torque
- Aesthetic goal = biomechanical goal
Viva punchline:
👉 Soft-tissue aesthetics guide incisor positioning.
9. Why no encroachment on lower lip?
- Teeth outside soft-tissue envelope relapse
- Lower lip exerts strong muscular pressure
- Advancing beyond lip contour → instability
- Staying within lip contour ensures:
- Muscular support
- Long-term stability
Viva punchline:
👉 Respecting the soft-tissue envelope prevents relapse.
10. Therapeutic diagnosis and extraction decision
- Therapeutic diagnosis = diagnosis through treatment response
- In Class II div 2:
- Complete first-phase correction
- Reassess space and alignment
- Avoid premature extraction decisions
- Especially useful in borderline cases
Viva punchline:
👉 Extraction is decided after observing treatment response.