Many lesions that occur on the jaw present with similar radiographic appearances making it difficult to differentiate among them . Despite development of various cross sectional imaging modalities ,the radiographs are still remain the first and most important investigations.
So some of the common features that we as dentist might come across are listed below.I believe this would come handy for your radiodiagnosis😊.
- Ghost teeth appearance-regional odontodysplasia
- Ground glass appearance-monostotic fibrous dysplasia, hyperparathyroidism, middle stage of paget’s disease & ossifying fibroma,sickle cell anemia
- Garrington sign-osteosarcoma (localised symmetrical widening of PDL
- Hanging drop appearance-orbital blow out fracture
- Heart shaped radiolucency-nasopalatine /incisive canal cyst
- Honey comb appearance-anerysmal bone cyst,odontogenic myeloma,central giant cell granuloma,central hemangioma

- Lincoln sign-paget’s disease (increased uptake in the mandible mimicking Lincoln’s beard.
- Mass of color/ cauliflower like appearance-calcified lymph nodes
- Moth eaten appearance-chronic osteomyelitis, early stage of ostesarcoma,radiolucent stage of fibrous dysplasia,squamous cell carcinoma,leukemia,malignant lymphoma
- Mottled appearance-ossifying fibroma,fibrous dysplasia
- Onion peel /skin appearance-Garre’s osteomyelitis, Ewing’s sarcoma,eosinophilic granuloma,caffey’s disease.
- Orange peel appearance-mixed stage of fibrous dysplasia (peud-de-orange)

- Pear shaped appearance-globulomaxillary cyst
- Pepper pot appearance-hyperparathyroidism
- Peripheral cuffing of bone-peripheral giant cell granuloma
- Pressure type appearance-squamous cell carcinoma of gingiva
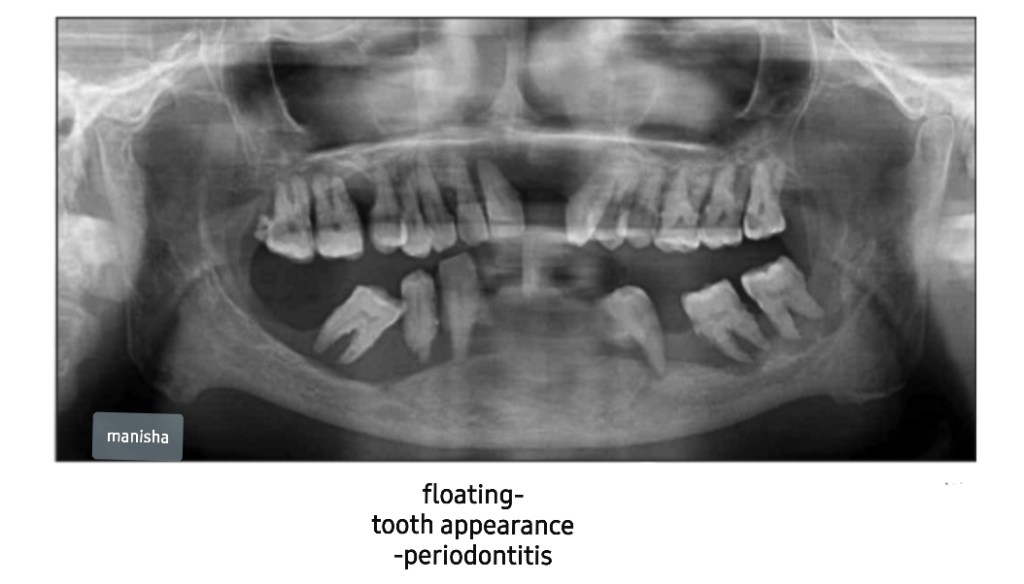
- Punched out appearance-multiple myeloma
- Rootless teeth appearance-dentinal dysplasia
- Salt and pepper appearance-hyperparathyroidism, thalassaemia
- Sausage like appearance-sialographic appearance of sialodochitis
- Sialectasis-sialographic appearance of sialadenitis
- Sharpened pencil appearance-osteoarthritis /rheumatoid arthritis of TMJ
- Shell teeth appearance-type III dentinogenesis imperfecta

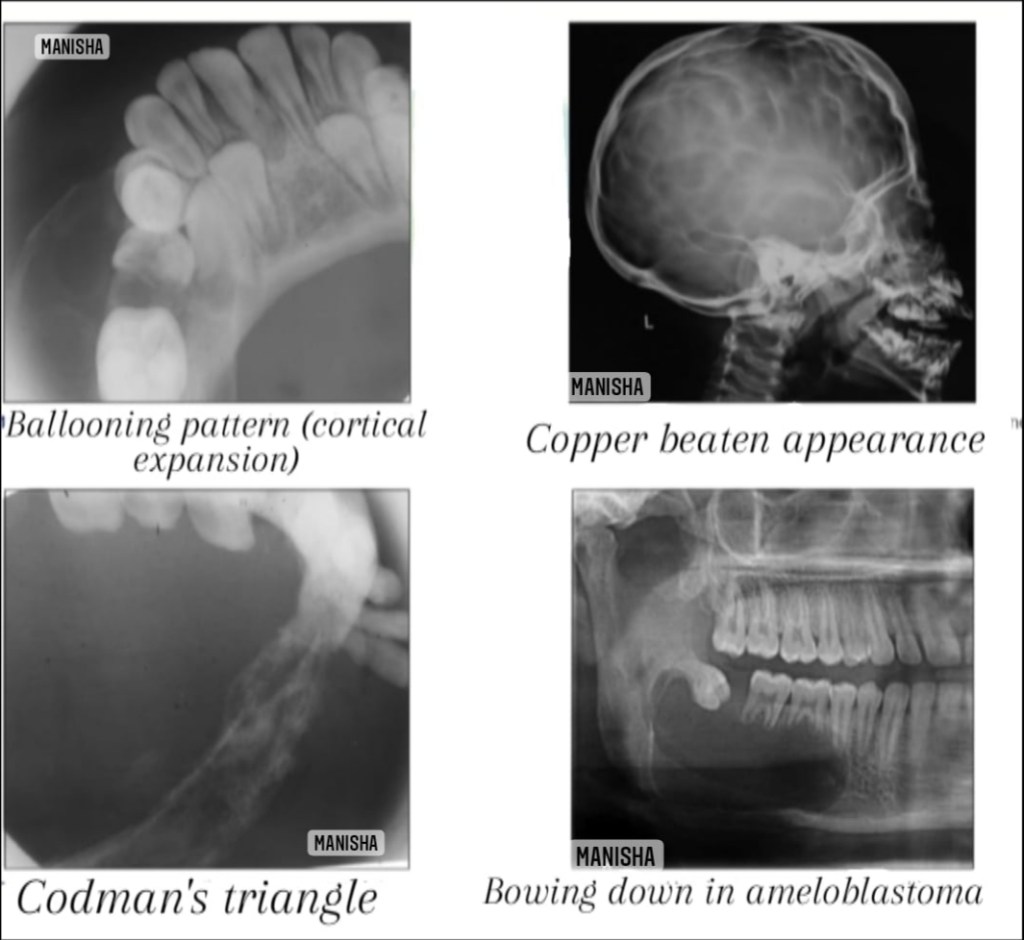
- Soap bubble appearance-ameloblastoma,aneurysmal bone cyst,central hemangioma,central giant cell granuloma, odontogrnic keratocyst
- Step ladder appearance-sickle cell anemia
- Sunburst/sunray appearance-central hemangioma,osteosarcoma,Ewing’s sarcoma
- Target sign-(rounded radiopacity with a central radiolucency)-impacted tooth in bucco lingual direction(lower 3rd molar)
- Tennis racket appearance-odontogenic myxoma
- Thistle tube appearance-type II dentinal dysplasia
- Thumb print /fingerprint appearance-mixed stage of fibrous dysplasia
- Tram track sign/calcifications-Sturge Weber syndrome
- Trap door appearance-orbital blow out fracture
- Tree in winter appearance-normal sialographic appearance of parotid gland
Some of the radiographic features are pathogonomic to a specific disease, thus can be helpful in narrowing down of differential diagnosis.
🖋Manisha M.A
Sources:White and Pharoah’s -Oral radiology textbook,Shafer’s textbook of oral pathology (8th edition) , Websites-www.ijournalhs.org, Article-Phore S,Panchal RS,Bhagla P, Nabi N.Dental radiographic signs.Indian j health sci 2015;8:85-90.