It refers to the cellulitis of the submandibular and submental regions combined with inflammatory oedema.
Causes:
🔍 Streptococcal organisms are responsible for the infection around the submandibular region.
🔍 Anaerobes also play a major role.
Clinical Features:
👩⚕️ Elderly patients who present with a diffuse swelling in the submandibular and submental regions (brawny oedema).
👨⚕️ Oedema of the floor of the mouth is seen which causes elevation of the tongue that in turn results in difficulty in swallowing.
👩⚕️ High grade fever with toxicity.
👨⚕️ Putrid halitosis is also characteristic of Ludwig’s angina.
Treatment:
💊 Rest and hospitalization
💊 Appropriate antibiotics should be given.
💊 Intravenous fluids to correct dehydration and Ryle’s tube feeding.
💊 If conservative management is not responsive in the patient, then surgery is preferred.
Surgery:
✂️ Under General Anaesthesia, a 5-6 cm curved incision is made below the mandible in the submandibular region and over the most prominent part of the swelling.
✂️ The submandibular gland is mobilised, mylohyoid muscle is divided, and the pus is drained.
✂️ Even if there’s no pus, the oedematous fluid comes out which in itself will improve the patient condition greatly.
✂️ The wound is closed by loose sutures, after cleansing the cavity with antiseptics and a drainage tube is inserted.
Complications:
⚠️ Mediastinitis and Septicaemia.
⚠️ Oedema of the glottis which is caused due to the spread of the cellulitis via a tunnel connecting stylohyoid muscle and submucosa of the glottis.
🔼 Clinical Presentation: Slow growing, non tender, a simple fibroma arising from the periodontal membrane, presents on the gum. May undergo sarcomatous change.
Giant Cell Epulis: (⭐ AKA Myeloid Epulis)
🔼 Consistency: Soft to firm gums with indurated underlying mass due to expansion of bone.
🔼 Clinical Presentation: It is an osteoclastoma arising in the jaw. Presents as hyperaemic vascular, oedematous, may ulcerate and result in haemorrhage. X ray shows pseudo trabeculation.
🔼 Treatment: Small tumours are treated by currettage; Large tumours are treated by radical excision.
Carcinomatous Epulis:
🔼 Consistency: Hard or malignant in consistency.
🔼 Clinical Presentation: This is an epithelioma arising from mucous membrane of the alveolar margin. Presents as a non healing, painless ulcer slowly infiltrating the bone. Hard regional lymph nodes are due to metastasis.
🔼 Treatment: Wide excision which includes removal of segment of the bone.
Broken Bone Fact #1: It’s no secret that smoking is bad for you, but did you realize that it can also have a negative impact on your ability to heal from broken bones?
Broken Bone Fact #2: If you aren’t sure you have a fracture, you can always try treating your injury at home with the “RICE” treatment: Rest, Ice, Compression and Elevation.
Broken Bone Fact #3: Ability to move isn’t a sure indicator of a broken bone, as the only way to confidently identify a fracture is with an X-ray. Infact, broken bones are almost always movable!
Broken Bone Fact #4: Fractures happen more easily as you get older. If you are over 85, your chance of breaking a bone is four times higher than if you are between the ages of 65 and 75.
Broken Bone Fact #5: At the end of the day, it’s better to see a doctor for your concerns. If you take too long to speak to your doctor about your possible broken bone, your bone could begin healing on its own in a crooked, painful and uncomfortable fashion!
STUDY NOTES ⚕️
Fracture:
A fracture is a structural break in the normal continuity of bone. This also includes hairline fractures.
Mechanism of Injury:
Direct violence ➡️ Fracture of tibia or mandible can occur due to a fall.
Indirect violence ➡️ Fracture of clavicle due to fall on outstretched hand.
Traction injuries ➡️ Traction of the ligament attached to the medial malleolus may lead to its fracture.
Compression fracture ➡️ It may occur due to fall from a height. May also be associated with impacted fracture of the vertebral body.
Types of Bones:
🔸Tubular bone
🔸Cancellous bone
Types of Fracture:
• Closed or Simple: There is no communication between the site of Fracture and the exterior.
• Open or Compound: There is a wound leading to the site of Fracture or communication between the Fracture site and the exterior.
Classification:
I. Depending on etiology of Fractures
II. Depending upon the plane of Fracture surface
III. Special Fractures
I. Depending on the etiology of Fractures
1️⃣ Traumatic Fractures
2️⃣ Pathological Fractures:
2a) Tumours 👉 Giant cell tumours, Secondaries in bone, bone cysts.
2b) Infections 👉 Acute osteomyelitis
2c) Metabolic bone diseases 👉 Hyperparathyroidism, Osteoporosis, Paget’s disease, Multiple myeloma, etc.
3️⃣ Stress Fractures:
Commonly seen in metatarsal bones (particularly in the second metatarsal due to prolonged marching).
Hence it is also called as ‘march fracture’.
II. Depending upon the plane of Fracture surface
• Transverse
• Spiral
• Oblique
• Comminuted
• Compression
III. Special Fractures
📍 Depressed Fractures
• Results due to sharp localised blow because of which a cortical bone segment is depressed.
• That needs to be treated with elevation of bone outwards.
• This type of Fracture is commonly seen in the skull.
📍 Fracture-Dislocation
• Fracture-Dislocation gives rise to severe pain and the continues till the dislocation is reduced.
• Classic example: Anterior dislocation of shoulder with Fracture of neck of humerus.
📍 Fracture involving a joint
• These Fractures should be treated with care OTHERWISE joint stiffness and late osteoarthritis can occur.
📍 Complex Fractures
• These Fractures involve major vessels or nerves.
• Example: Fracture of humerus associated with radial nerve injury or fracture of lower femur associated with popliteal artery injury.
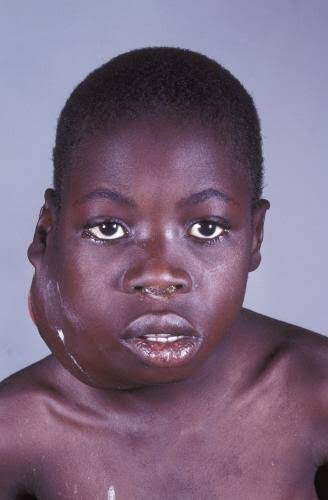
It is also called as ‘African jaw lymphoma’. It is a lymphoreticular cell malignancy. In the African form jaw involvement is 75% and in cases of the American form, abdomen involvement is more common. It is a B-cell neoplasm.
Etiology
• Epstein-Barrvirus(EBV)which also causes nasopharyn- geal carcinoma and infectious mononucleosis is considered to be the etiological factor. There are higher EBV antibody levels in patients of Burkitt’s lymphoma.
Clinical Features
Age and sex—peak incidence is in children between 6to 9 years. Males are affected more commonly than the females, with a ratio of 2:1.
Site distribution—more are found in maxilla than in mandible, where it may spread rapidly to the floor of the orbit. Almost always occurs in molar area. In the African form, more than one quadrant is involved while in the American form, only one quadrant is involved.
Onsetandprogress—the most important hall mark of this tumor is the fast growth with a tumor doubling time of less than 24 hours.
Symptoms—the most common presenting features are swelling of the jaws, abdomen and paraplegia. It is painless.
Sign—peripheral lymphadenopathy is common.
Prognosis—it is rapidly fatal in the absence of treatment,with death occurring within 6 months.
Oral Manifestations
• Onset and extent—it begins generally as a rapidly growing tumor mass of the jaws, destroying the bone with extension to involve maxillary, ethmoid and sphenoid sinus as well as orbit.
Symptoms—loosening or mobility of permanent teeth.There is gross distortion of the face due to swelling. Paresthesia and anesthesia of inferior alveolar canal or other sensory facial nerves are common.
Signs—gingiva and mucosa adjacent to the affected teeth become swollen, ulcerated and necrotic. As the tumor mass increases, the teeth are pushed out of their sockets. Swelling of the jaw occurs and it may cause facial asymmetry. They are capable of blocking nasal passages, displacing orbital contents and eroding through skin. There is derangement of arch and occlusion. There may be large quantity of mass protruding into the mouth, on the surface of which may be seen rootless, developing permanent teeth.
Spread—once the tumor perforate the bone, it is initially confined by the periosteum, but subsequently it spreads to the soft tissues of the oral cavity and face where rapid tumor growth soon obliterates the entire face and skin becomes tense and shiny.
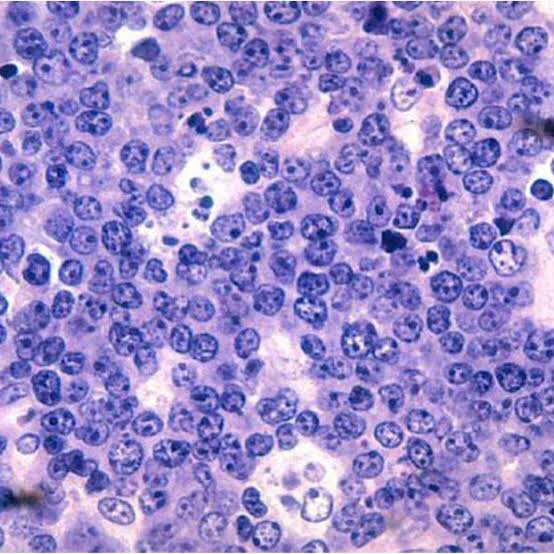
Histology
Shows characteristic starry sky appearance.
Radiographic Features
Motheatenappearance—small radiolucent foci scattered throughout the affected area. These small foci coalesce and form a multilocular moth eaten appearance.
Sunray appearance—if periosteum is elevated, it will produce sunray appearance.
Margins—margins are ill defined and non-corticated.
Shape—they expand rapidly and are ballooned shaped.
Teeth—Lesions are osteolytic with loss of lamina dura about the erupted teeth and crypts of developing teeth are enlarged.
Effect ons urrounding structures—they expand very rapidly and breach its outer cortical limits.
Diagnosis
• Clinical diagnosis—swelling of the jaw and abdomen with peripheral lymphadenopathy can give clue to the diagnosis.
• Radiological diagnosis—moth eaten appearance is seen with loss of lamina dura around the teeth.
• Laboratorydiagnosis—monotonous sea of un differentiated monomorphic lymphoreticular cells, usually showing abundant mitotic activity. There is also hyperchro- matosis and loss of cohesiveness. Characteristic ‘starry sky’ appearance is seen.
Management
• Cytotoxicdrugs—cytotoxicdrugs like cyclophosphamide 40 mg/kg in single IV administration and repeated about 2 weeks later. Vincristine and methotrexate have been successful in some cases.
• Multiagent chemotherapy—combination of drugs such as cyclophosphamide, vincristine and methotrexate give better results than any single drug. Majority of patients show dramatic response to the therapy. The swelling regresses and the displaced teeth return to their normal position within 1 to 2 weeks.
REFERENCE- SHAFER’S TEXTBOOK OF ORAL PATHOLOGY AND ANIL GHOM TEXTBOOK OF ORAL MEDICINE
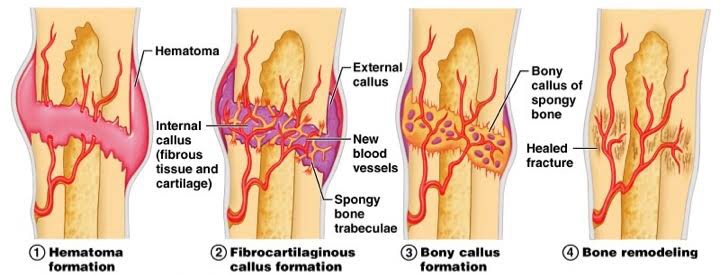
•Bone production begins when the clotted blood formed by inflammation is replaced with fibrous tissue and cartilage (known as soft callus). As healing progresses, the soft callus is replaced with hard bone (known as hard callus), which is visible on x-rays several weeks after the fracture.
🔅What foods heal bones faster?
•Iron helps your body make collagen to rebuild bone. It also plays a part in getting oxygen into your bones to help them heal. •Good sources: Red meat, dark-meat chicken or turkey, oily fish, eggs, dried fruits, leafy green veggies, whole-grain breads, and fortified cereals.
🔅How long does it take for a broken bone to fully heal?
•A broken bone and the surrounding soft tissue damage need a minimum of six to eight weeks to heal. However, depending on your general health and the condition of your bone and soft tissue, healing can take much longer.