Sinus
Latin: Hollow (or) a bay
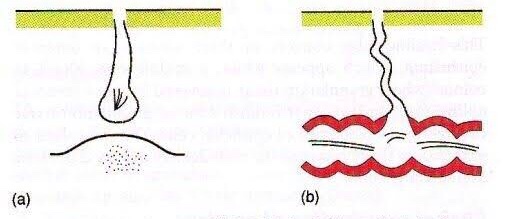
A sinus is a blind tract leading from the surface down to the tissue. There may be a cavity in the tissue which is connected to the surface through a sinus. The sinus is lined by granulation tissue which may be epithelized.
A sinus has one open draining end and the channel ends in a blind ending. An example would be a dental sinus draining from a dental abscess to either the inside of the mouth or the skin.

Fistula
Latin: flute(or) a pipe (or) a tube
It is a communicating tract between 2 epithelial surfaces commonly between hollow viscous & skin or between 2 hollow viscera. The tract is lined by granulation tissue which is subsequently epithelized. A fistula may be an abnormal communication between vessels.
An example would be from the mouth (oral cavity) to the skin surface, usually of the face or neck, and this specific type is called an orocutaneous fistula.


Fistulas and sinuses of the neck and face: classification
Fistulas and sinuses of the neck and face may be classified by cause.
Developmental
Fistulas and sinuses due to developmental causes are usually present at birth.
- Thyroglossal duct cyst – the most common developmental cyst in the neck. The cyst characteristically moves upwards when the tongue is poked out or with swallowing. It may burst to form a sinus which usually opens just below the hyoid bone in the midline of the neck. It drains mucus.
- Branchial cleft cyst – the most common developmental cyst of the side of the neck. A sinus may drain mucus or pus following rupture of an abscess. It usually opens on the side of the neck.
- Preauricular sinus

Cysts
Cysts are lumps in the skin containing fluctuant contents. They may have an opening to the skin surface.
- Dermoid cyst
- Epidermal cyst

Traumatic
- Accidental
- Radiotherapy
- Surgical
Infective
- Actinomycosis
- Bone infection
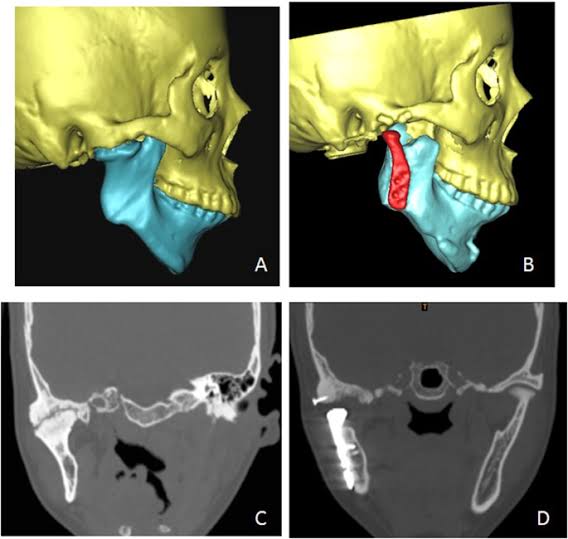
Chronic osteomyelitis – most commonly associated with poorly controlled diabetes mellitus or following radiotherapy to the jaw for cancer or Paget disease of the bone. It may also complicate a chronic dental infection. - Dental infection
- Chronic dentoalveolar abscess
- Dental implant
- Failed endodontic procedure
Lymph node
- Cat scratch disease
- Dental infection
- Tuberculosis (scrofuloderma)

Neoplastic
- Oral squamous cell carcinoma is the most common
- Benign tumours of the mouth rarely form a fistula
Causes for persistence of sinus/fistula
- Presence of a foreign body e.g. suture material
- Presence of a necrotic tissue underneath e.g. sequestrum
- Insufficient or non-dependent drainage. e.g. TB sinus
- Distal obstruction e.g. biliary fistula
- Persistant drainage like urine/faeces/CSF
- Lack of rest
- Epithelialisation of the tract e.g. AVF
- Malignancy
- Dense fibrosis
- Irradiation
- Malnutrition
- Specific causes e.g. TB, actinomycosis
- Ischemia
- Drugs e.g. steroids
- Interference by the patient
How is a fistula or sinus diagnosed?
In addition to careful history and examination, one or more of the following tests will usually be required to confirm the diagnosis and determine the cause:
- passing a probe into the channel
- radiology – may include plain x-rays, x-rays using contrast medium, CT or MRI scans
- microbiological assessment of swabs or biopsy material
- biopsy and pathology
Abscess
Collection of pus
Clinical Features & Diagnosis:
Features of acute inflammation; The four cardinal signs of inflammation are:
- redness (Latin rubor) – below localization of abscess
- heat (calor) – inflammed area is hot
- swelling (tumor) – pus present inside abscess cavity
- and pain (dolor) – throbbing type
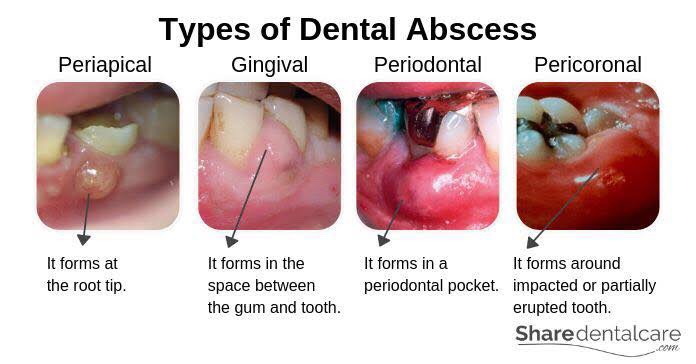
Diagnosis of Dental Abscess:
- The location of abscess will cause tenderness with palpation test
- The abscessed tooth will be very sensitive to percussion
- IOPA findings will suggest slight thickening of PDL space with radiolucency at apex
Dentowesome|@drmehnaz🖊
References:
- dermnetnz.org
- SlideShare
- Google.com
- Study Notes✍🏻