
https://www.instagram.com/s/aGlnaGxpZ2h0OjE4MTA3MTAwODIzMTUzMzU2?igshid=xo73gjk8yp0w
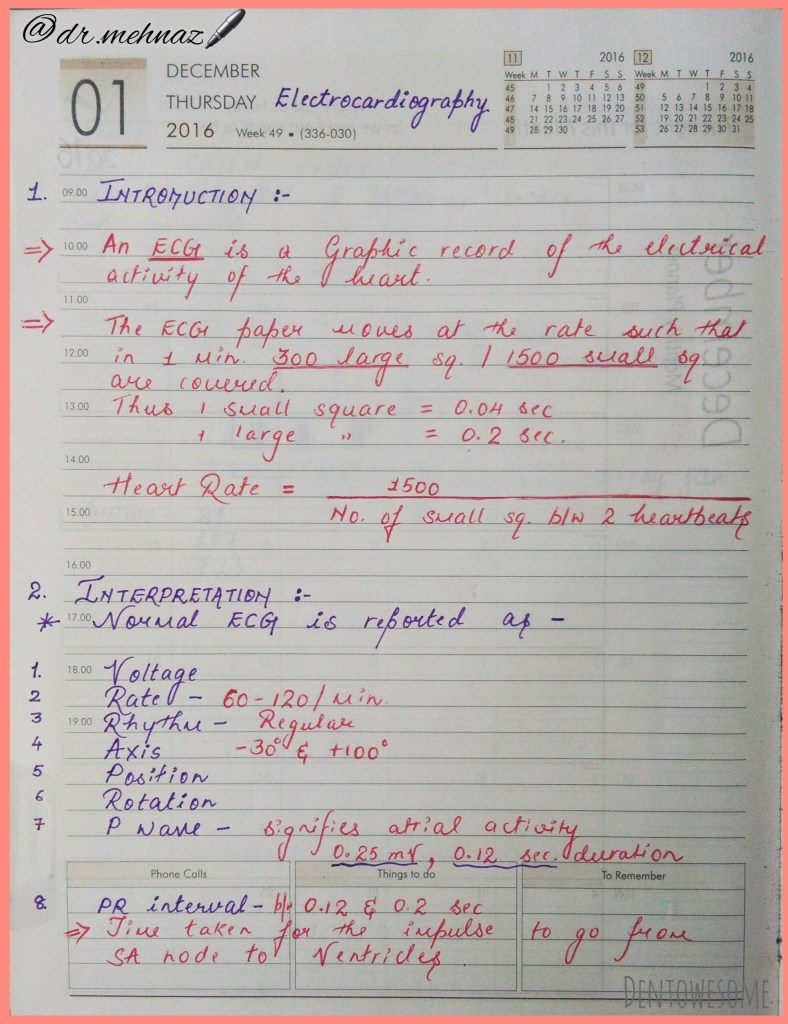
To access realistic looking recordings library which will help improve your ECG skills, head on to the next page!
https://www.instagram.com/s/aGlnaGxpZ2h0OjE4MTA3MTAwODIzMTUzMzU2?igshid=xo73gjk8yp0w
To access realistic looking recordings library which will help improve your ECG skills, head on to the next page!









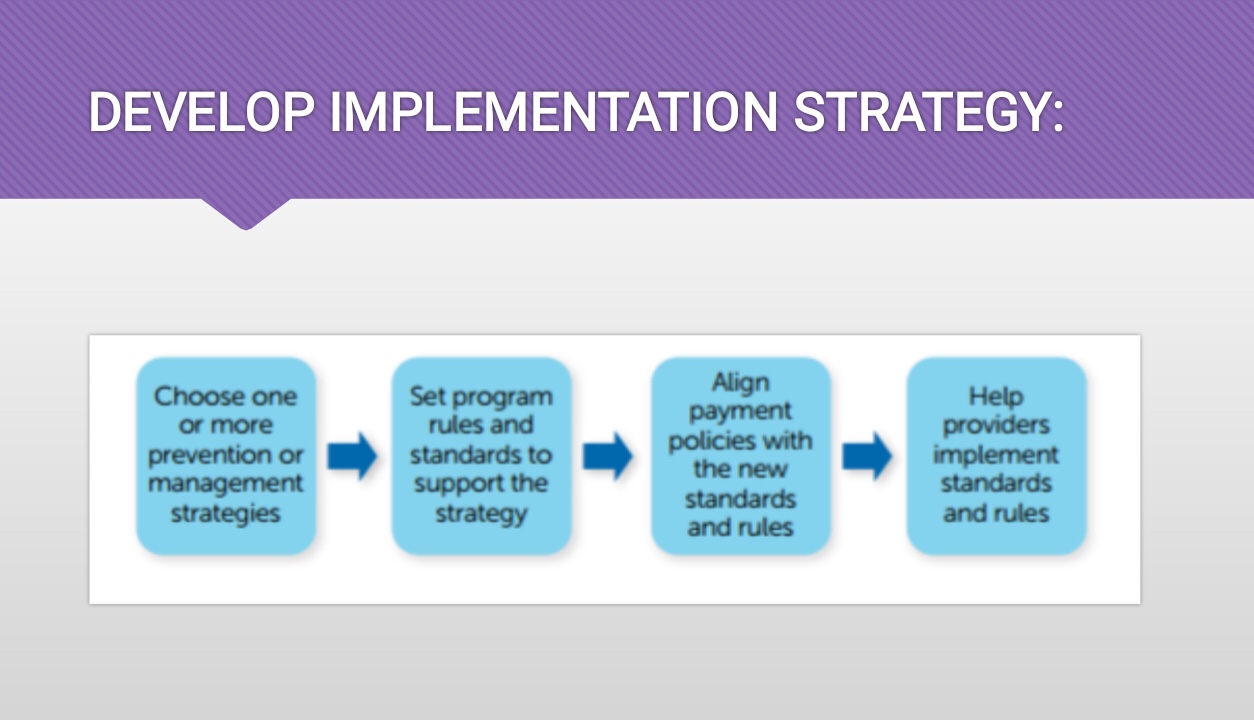






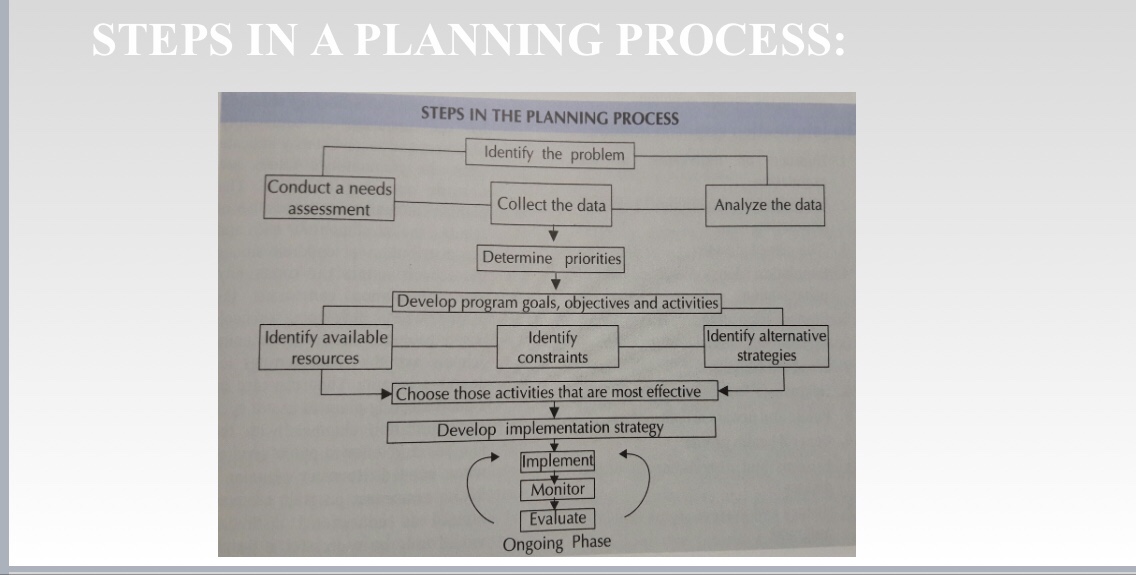
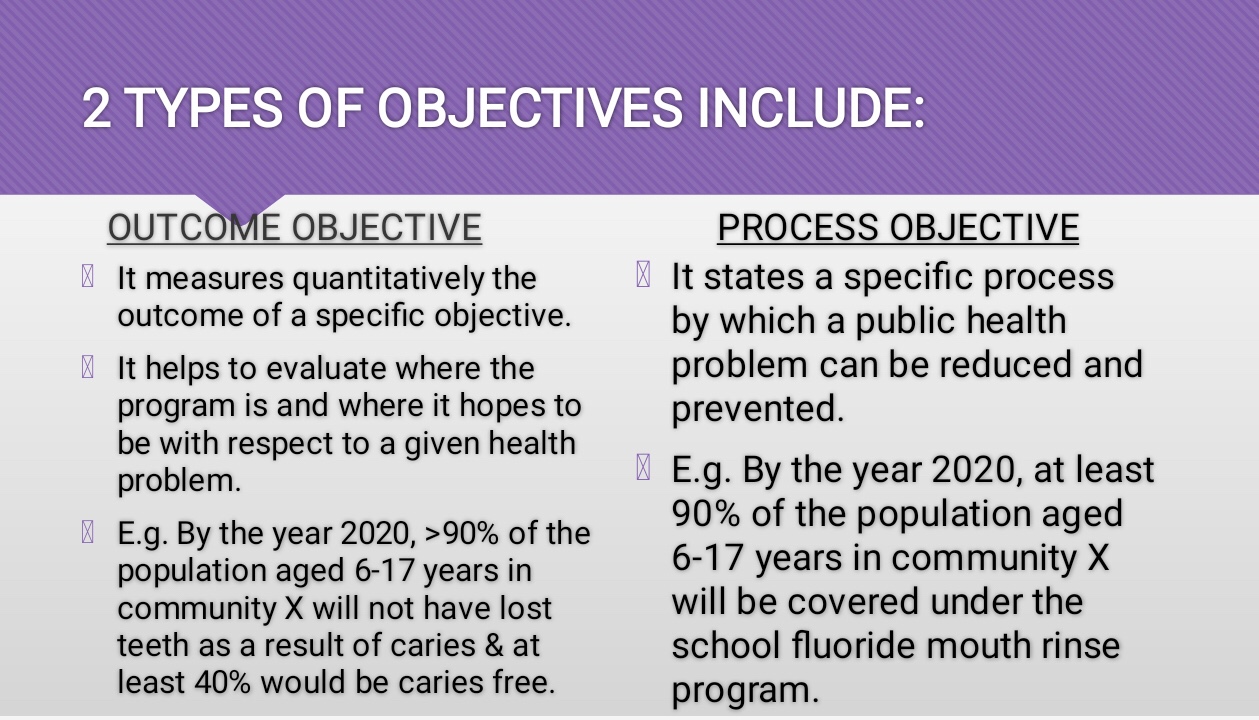
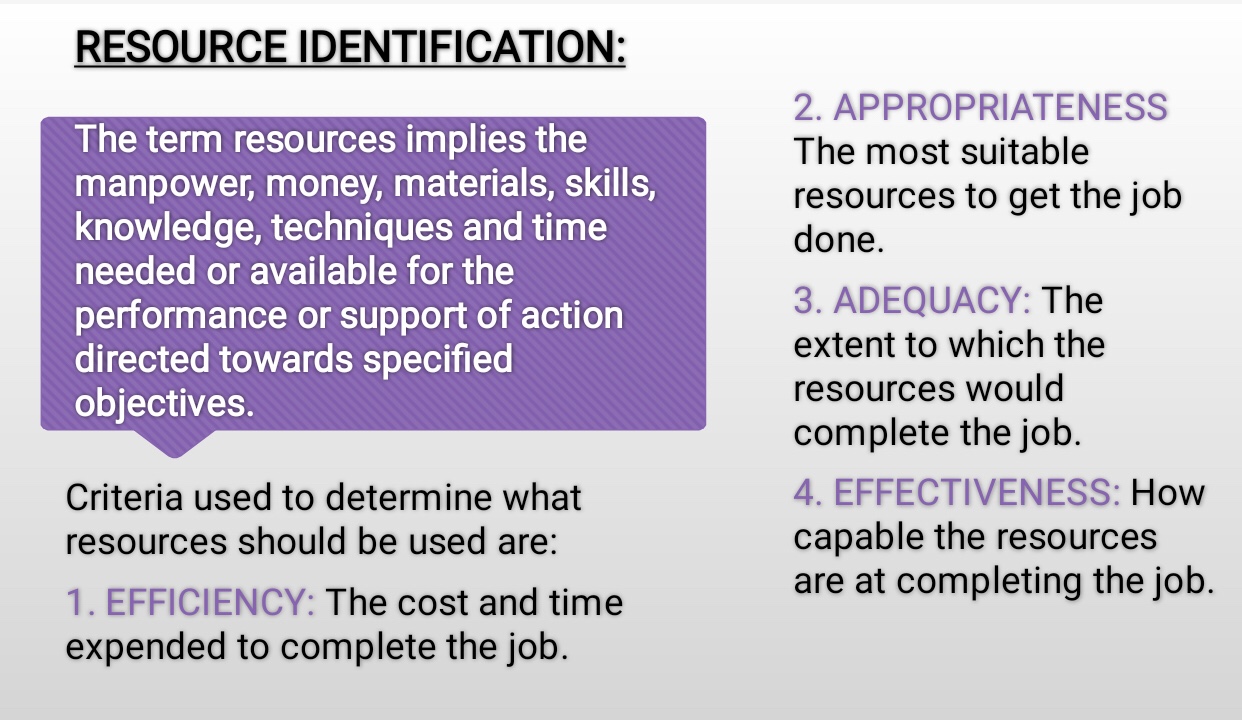
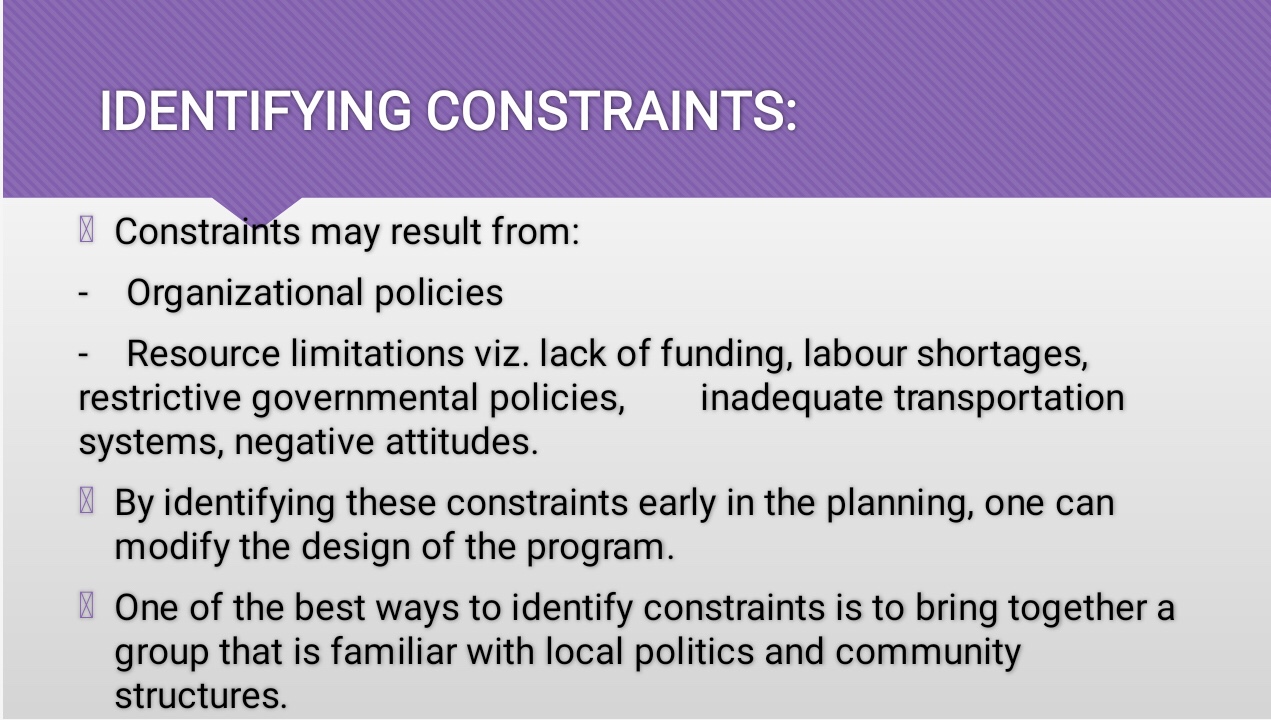
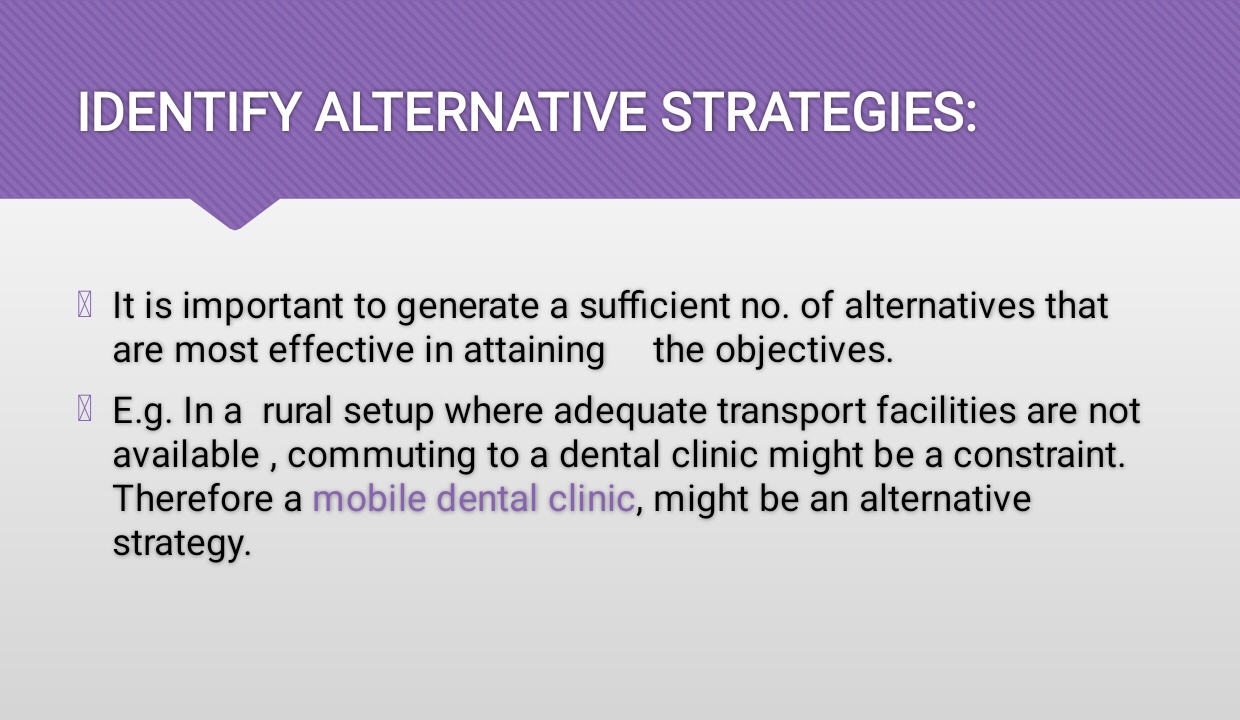
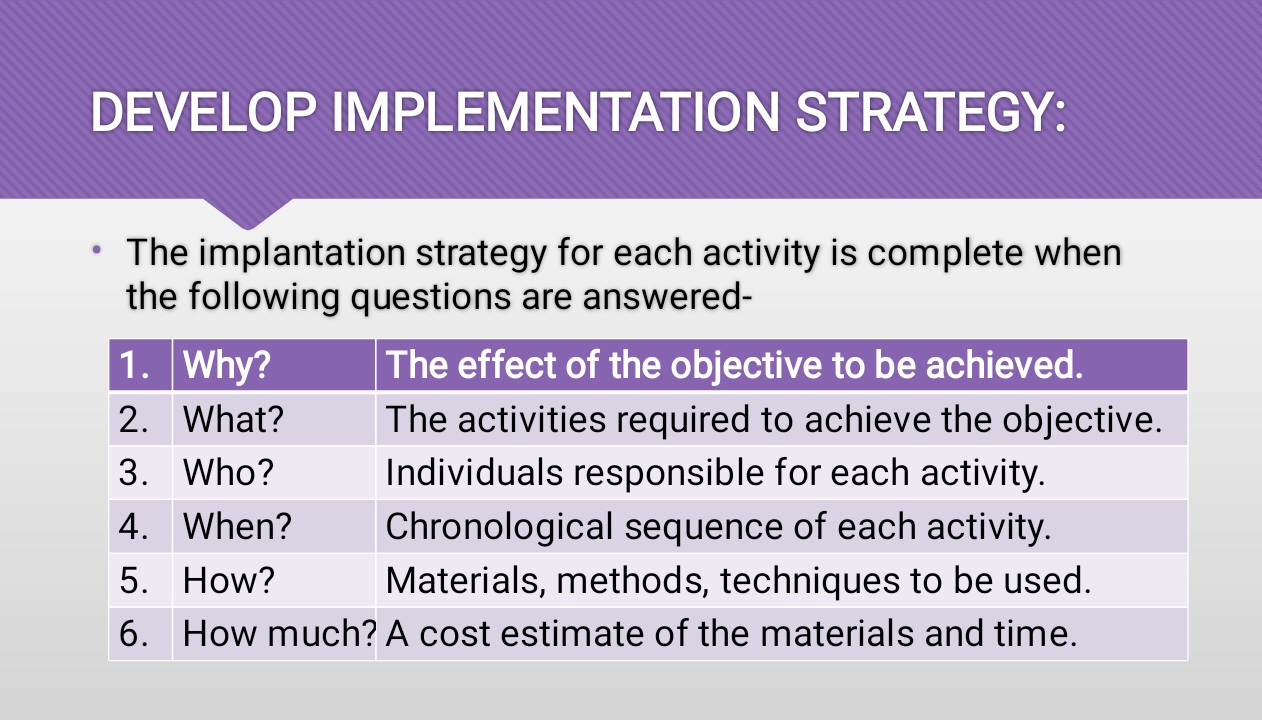
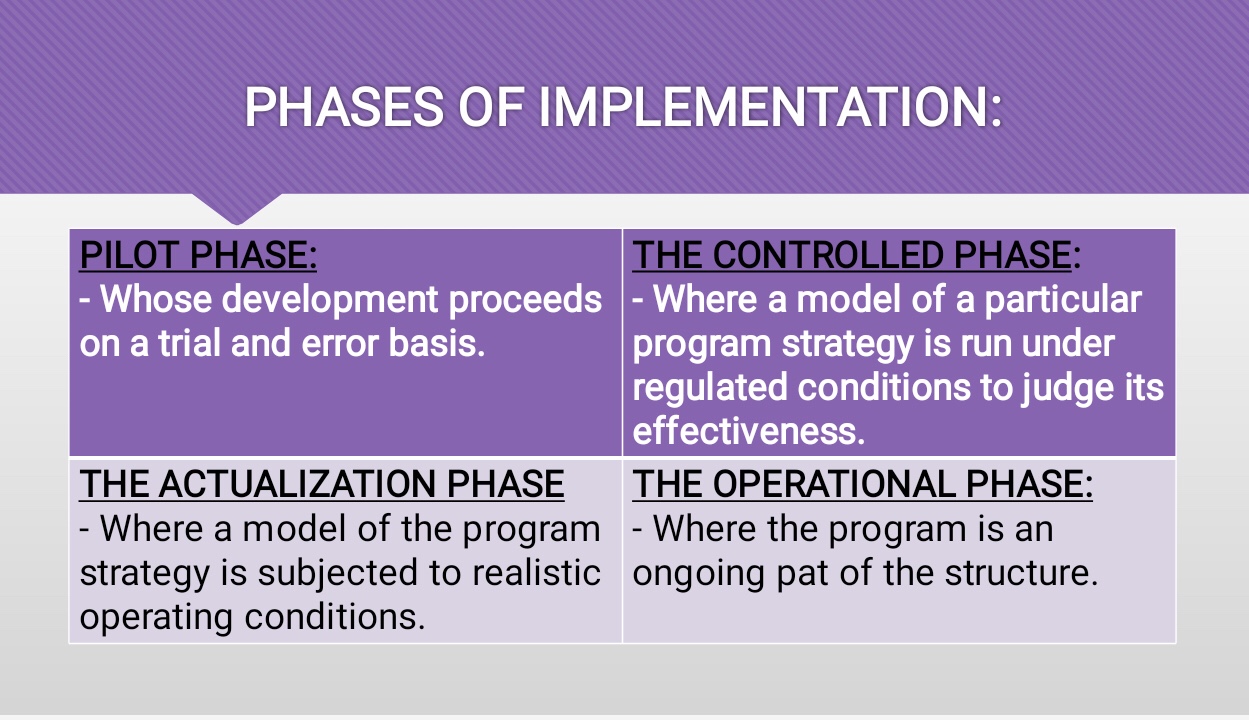
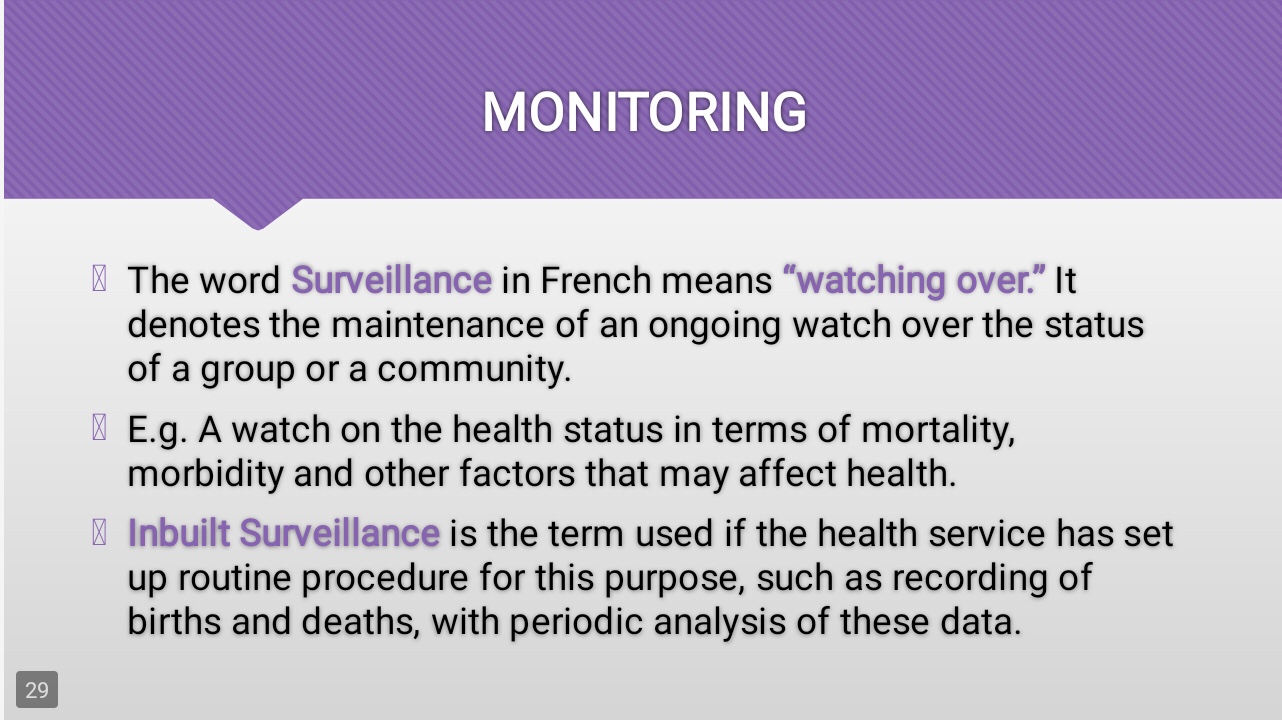
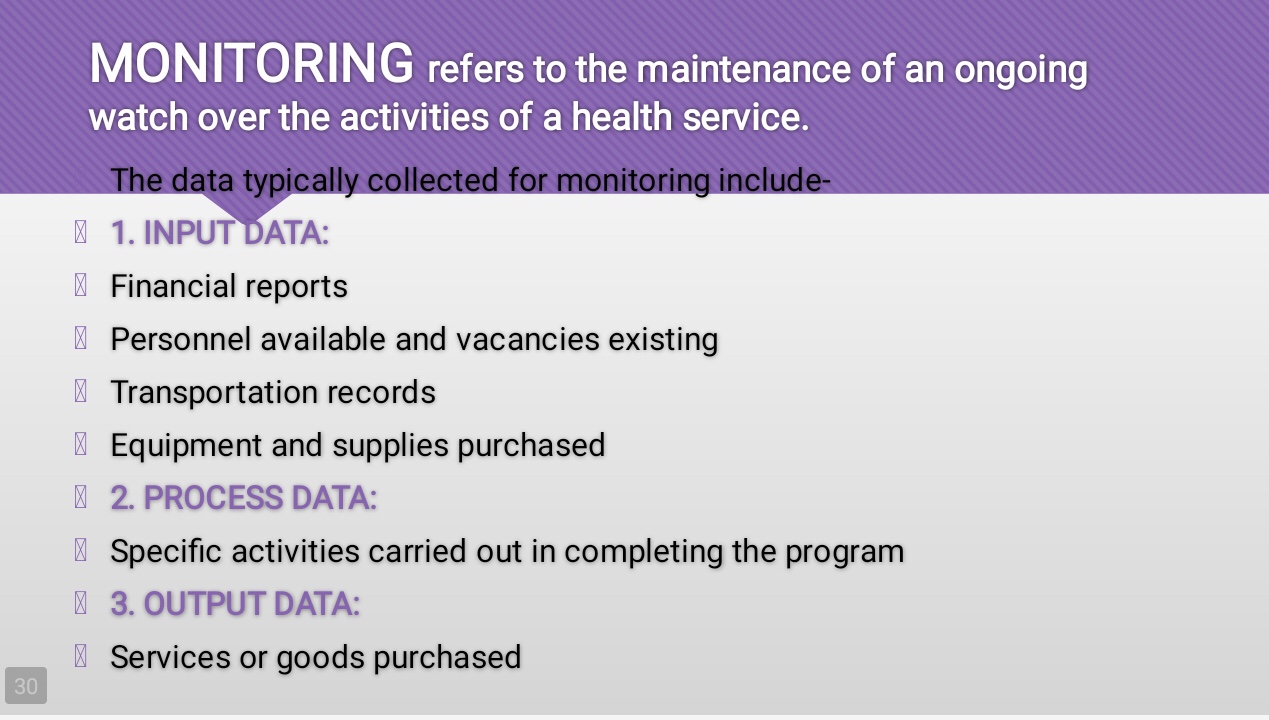
STEPS IN THE PLANNING PROCESS👇🏻
References: Textbook of Public Health Dentistry-Sober Peter(5th Edition)
References: Textbook of Public Health Dentistry-Sober Peter(5th Edition); Random google images

Source: Internet
A neoplasm of epidermal melanocytes and third most common cancer of skin.
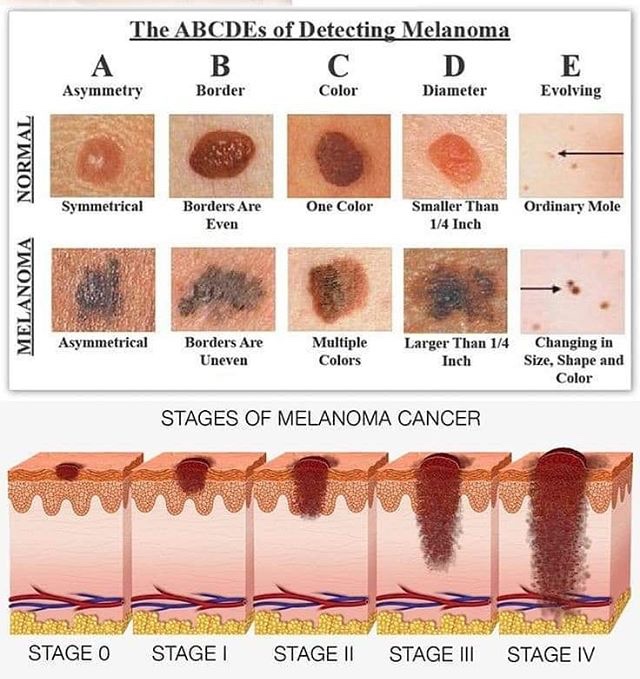
▪️Arises in preexisting mole. Appearance – Large, flat, spreading lesion; deeply pigmented Nodule
(i) Congenital Nevi
https://dentowesome.wordpress.com/2020/05/18/oral-nevi/
(ii) Dysplastic Nevi (Atypical Mole)
(iii) Lentigo Maligna: Also called as Hutchinson’s freckle, is a tan or black on the skin that looks like a freckle.
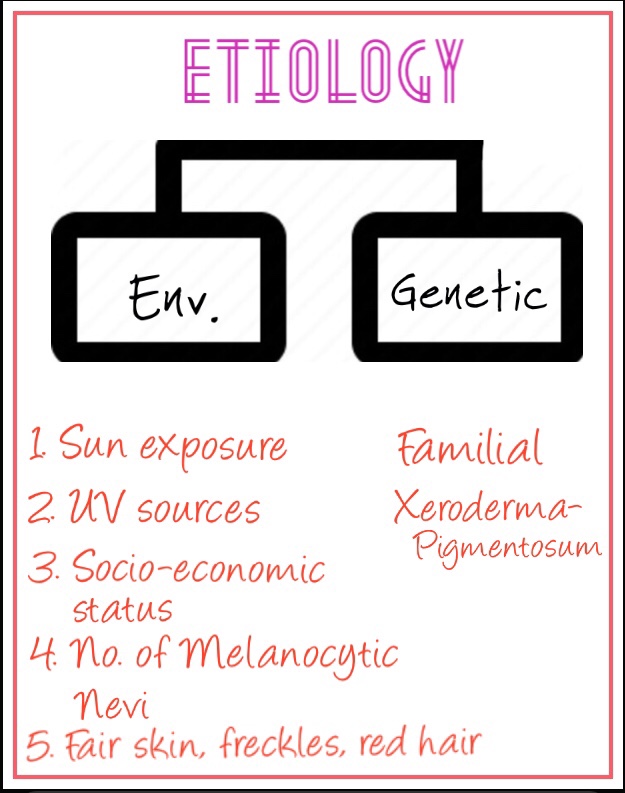
• Genes in the development of Melanoma:
• Phases in the growth of Melanoma:
1. Superficial spreading Melanoma:
2. Lentigo Maligna Melanoma:
3. Nodular Melanoma:
4. Acral Lentiginous:

➡️ Metastases that cause symptoms but cannot be removed may be treated with radiation, immunotherapy, targeted therapy, or chemotherapy.
Dr. Mehnaz Memon🖊
References: Shafer’sTextbook Of Oral Pathology; Textbook Of Surgery by S.Das
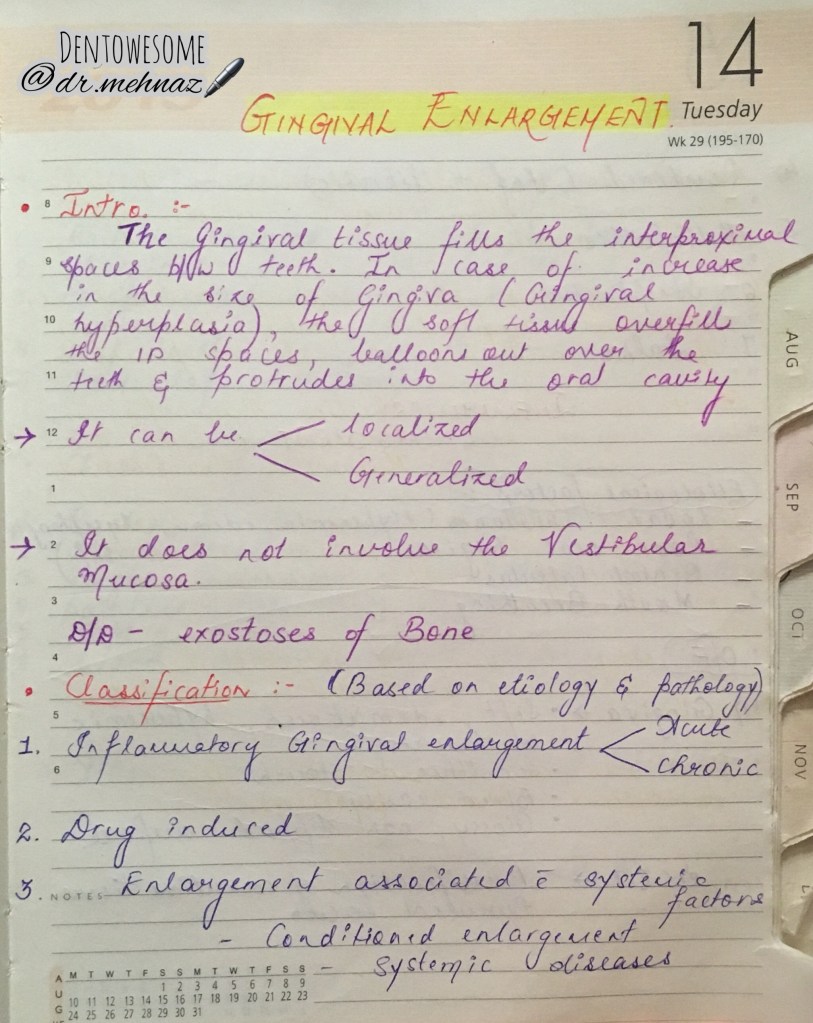





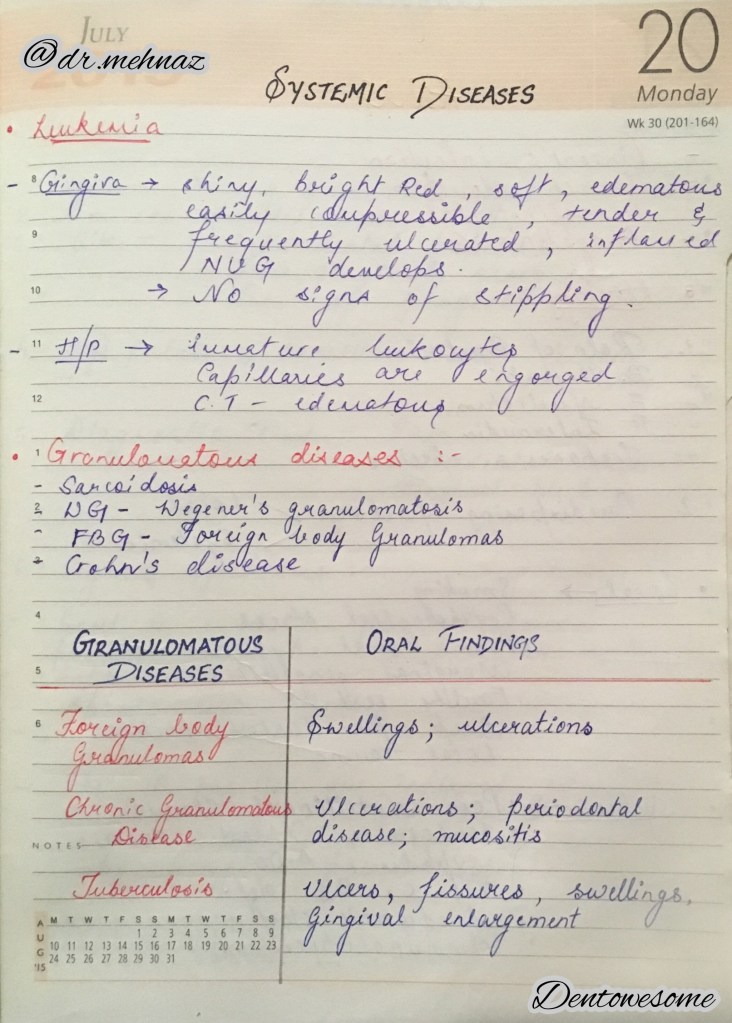

References: Essentials Of Periodontology by S Sahitya Reddy; Shafer’s Oral Pathology; Carranza’s clinical periodontology; Internet
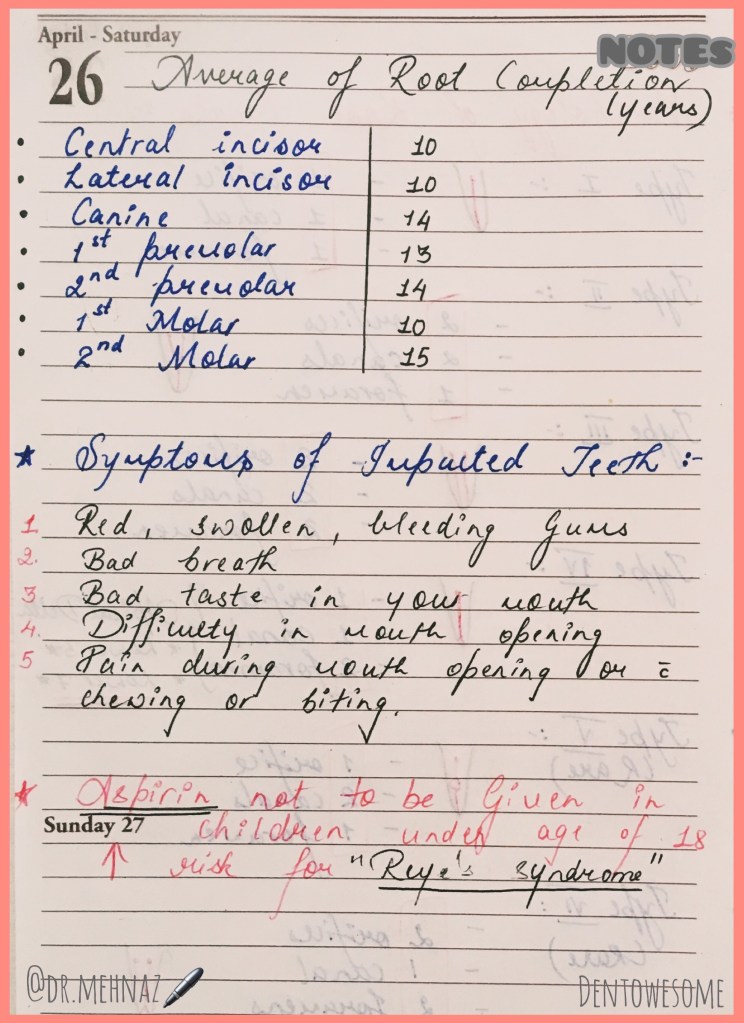
The term eruption is used to denote the tooth’s emergence through the gingiva but the occlusal definition is equal movement of tooth from the dental bud to occlusal contact.
Upper
Lower
Maxillary Teeth
Mandibular Teeth
Dentowesome 2020 @dr.mehnaz
References: Textbook-Pediatric-Dentistry-Nikhil-Marwah
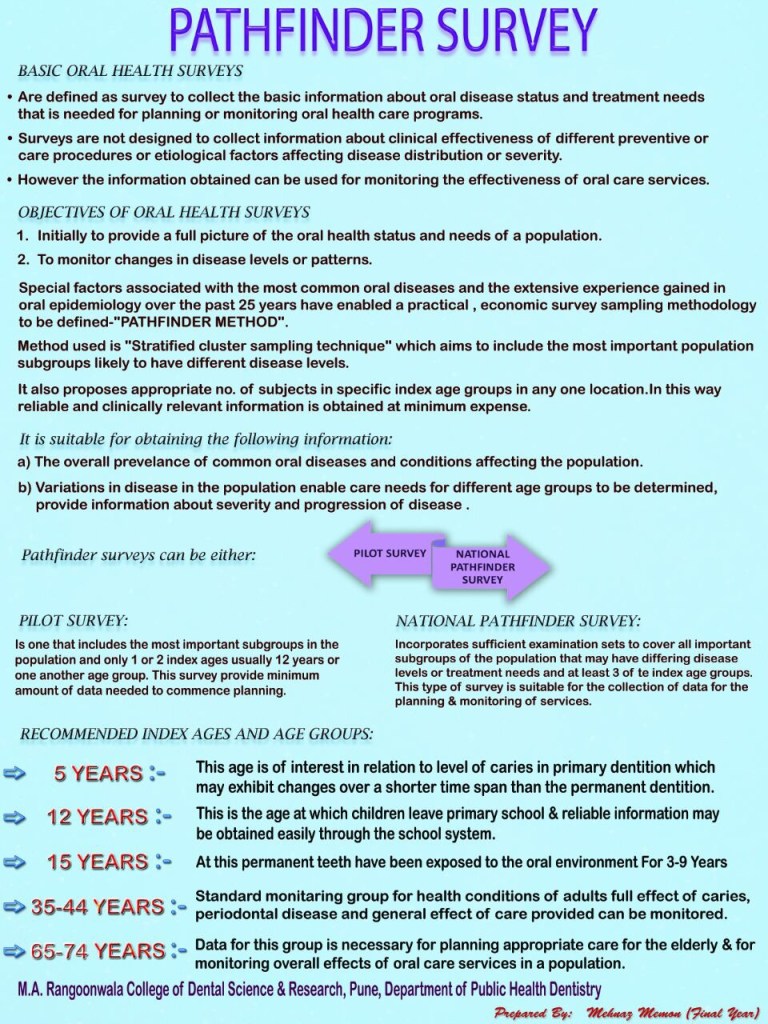
References: Textbook of Public Health Dentistry-Sober Peter(5th Edition)
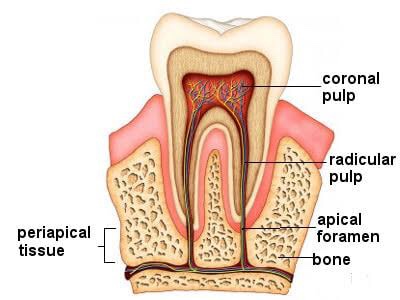
➡️ For all operative procedures, the shape of pulp chamber & its extensions into the cusps, pulpal horns is important.
➡️ In some developmental disturbances the pulpal horn projects high into the cusps & exposure of pulp can occur when it is least anticipated.
➡️ Pulpitis is the response of the traumatized pulp with trauma being the result of a bacterial infection as in dental caries or physical trauma to tooth structure.
➡️ Pulpitis in milder form could result in focal reversible pulpitis & may progress if left unchecked to acute & chronic forms of pulpitis.
➡️ Well vascularized pulpal tissue may at times in carious molar teeth of young adults & children with open apex exhibit a form of hyperplasia seen clinically in exposed pulp chamber as a protruding red mass of granulation tissue called pulp polyp or chronic hyperplastic pulpitis.
➡️ Inflammation within pulp may also sometimes result in a condition called pulp polyp, internal resorption or pink tooth.
➡️ Pulp infection can spread apically into PDL causing granuloma, abscess, cysts.
➡️ Pulp stones lying at the opening of the root canal may cause difficulty to locate the root canals.
➡️ A necrotic pulp can cause spread of disease to periodontium through an accessory canal.
➡️ Pulp capping is successful in non-infected or minimally infected accidentally exposed pulp in individuals of any age.
Source: Internet, Grossman’s Textbook of Endodontics
Dentowesome 2020 @ dr.mehnaz
