🔖 Acrocephalosyndactyly. The condition is autosomal dominant i.e, one copy (out of 2) of the defective gene is sufficient to cause the abnormality in the offspring.
🔹Characteristics:
- Craniosynostosis (premature fusion of the skull bones)
- Craniofacial anomalies
- Syndactyly (Fusion of fingers and toes)
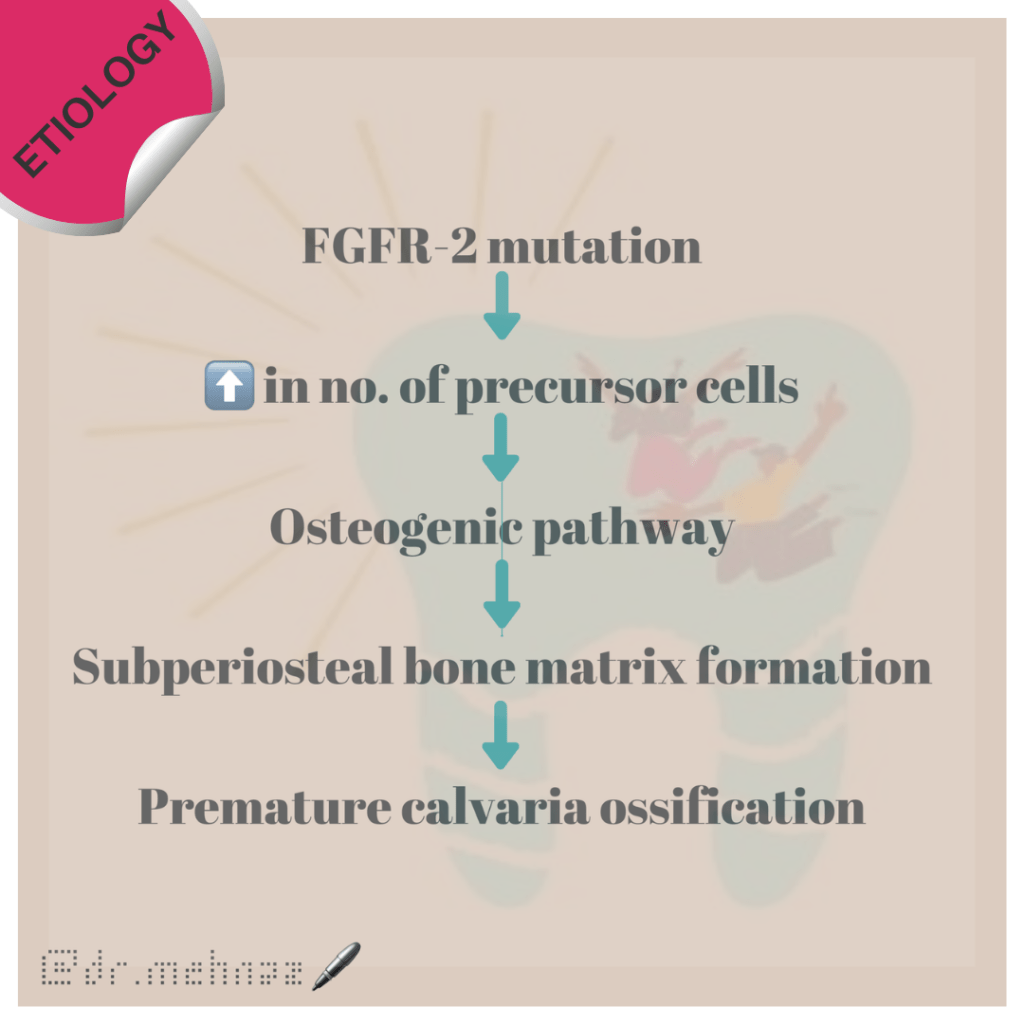
🔹Etiology:
🔹What are the Symptoms and Signs of Apert Syndrome?
The various clinical features include:

- Asians affected
- Acrocephaly, Brachycephaly, flat occiput & prominent forehead.
- Late closing fontanels
- Low set ears, hearing loss
- Eyes: Down slanting of palpebral fissures, Widely spaced eyes(Hypertelorism), Shallow orbits, Abnormally bulging eyes (Exophthalmos)
- Nose: Depressed Nasal bridge, short, wide with bulbous tip, Parrot beaked appearance, Atresia
- Jaw:
- Prominent Mandible
- Maxillary hypoplasia
- Drooping angles of mouth
- High arched palate
- Bifid uvula
- Cleft palate
- Crowded upper teeth
- Malocclusion
- Delayed & ectopic eruption
- Shovel shaped incisors
- Supernumerary teeth
- V-shaped maxillary dental arch
- Bulging alveolar ridges
8. Partial to complete fusion of digits: 2-4th digits – MITTEN HANDS & SOCK FEET; Sole – supinated
9. Intelligence – Normal
10. ⬆️ intracranial pressure – optic atrophy, papilledema
11. Hyperhidrosis
12. Cardiovascular system: Atrial Septal defect, Ventricular septal defect, Patent ductus Arteriosus
🔹How do you Treat Apert Syndrome?
Standard Therapies
The treatment of Apert syndrome aims at addressing the specific symptoms that may be present in the particular individual. Treatment is usually symptomatic and supportive.
- Craniosynostosis and associated hydrocephalus in some cases may give rise to an abnormally increased pressure within the skull (intracranial pressure) and on the brain. In these cases, early surgery (within 2 to 4 months after birth) becomes necessary to correct the defects in the skull and facial bones.
- Insertion of a tube (shunt) to drain excess cerebrospinal fluid (CSF) away from the brain and into another part of the body like the abdomen where the CSF can be absorbed can be done to relieve associated hydrocephalus (fluid accumulation in the brain).
- Early repair and reconstructive surgery may also be done in some infants with Apert syndrome to address craniofacial abnormalities.
- Other defects such as those of heart, eye and ear defects may also need correction.
Dr. Mehnaz Memon🖊
References:
- https://www.medindia.net/amp/patientinfo/apert-syndrome.htm
- Shafer’s textbook of Oral Pathology – 7th Ed.