




Dr. Mehnaz Memon🖊
References:



Dr. Mehnaz Memon🖊
References: Davidson’s Principles and Practice of Medicine Textbook





Indications for cardiac surgery in Infective Endocarditis:
🔅 Heart Failure due to valve damage
🔅 Failure of antibiotic therapy
🔅 Large vegetations
🔅 Abscess formation
Dr. Mehnaz Memon🖊
References: Davidson’s Principles and Practice of Medicine Textbook





Dr. Mehnaz Memon🖊
Dentowesome 2020
References: Davidson’s Principles and Practice of Medicine Textbook

(A)
(B)
5. Regular exercise: Jogging & swimming – ⬇️ Arterial pressure
• Objectives
🔅 To reduce the incidence of adverse cardiovascular events viz coronary heart disease, stroke & heart failure
• Benefits:
🔅Diuretics or β blockers have shown to reduce the risk of
🔅Most of the excess Morbidity & Mortality associated with HT is attributable to CAD. Total CVR = CAD risk x 4/3
🔅 Hypertension in old age:
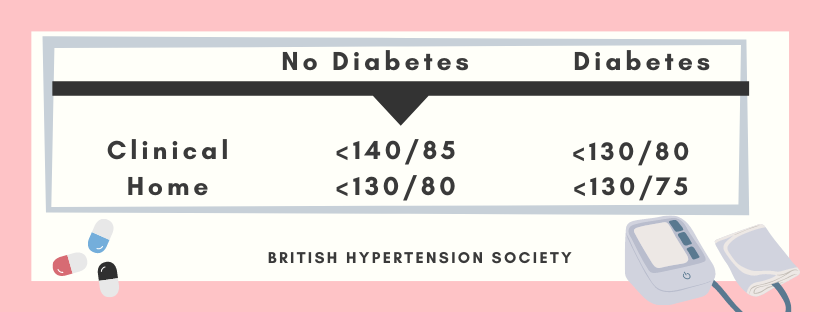
Target BP during AHT



A. ACE Inhibitors:
👉🏻Patients with renal artery stenosis/impaired Renal function (given with utmost care)
⬇️
Reduction of filteration pressure in the glomeruli
⬇️
Renal failure
👉🏻These agents also reduce the progression of Nephropathy in type II diabetes
👉🏻Level of electrolytes & creatinine should be checked before & after 1-2 weeks.
B. ARB’s
👉🏻Have lesser side effects of cough & angioedema than ACE inhibitors
C. Beta-blockers:
👉🏻These drugs are not used now as first line AHT; except in patient with Angina
👉🏻Labetalol & Carvedilol: Have better effect when combined. Labetalol is used as infusion in malignant phase HT.

D. CCB’s
👉🏻The dihydropyridines are effective, well-tolerated particularly in older people
👉🏻Rate–limiting CCB’s: HT with angina. Bradycardia may occur
E. Thiazides & other Diuretics:
👉🏻The loop diuretics have few A/D over thiazides unless there’s renal impairment.

Chart showing Mode of Action & Side effects of AHT’s☝🏻

The influence of comorbidity on the choice of antihypertensive drug therapy

Management of hypertension: British hypertension society guidelines
Criteria:
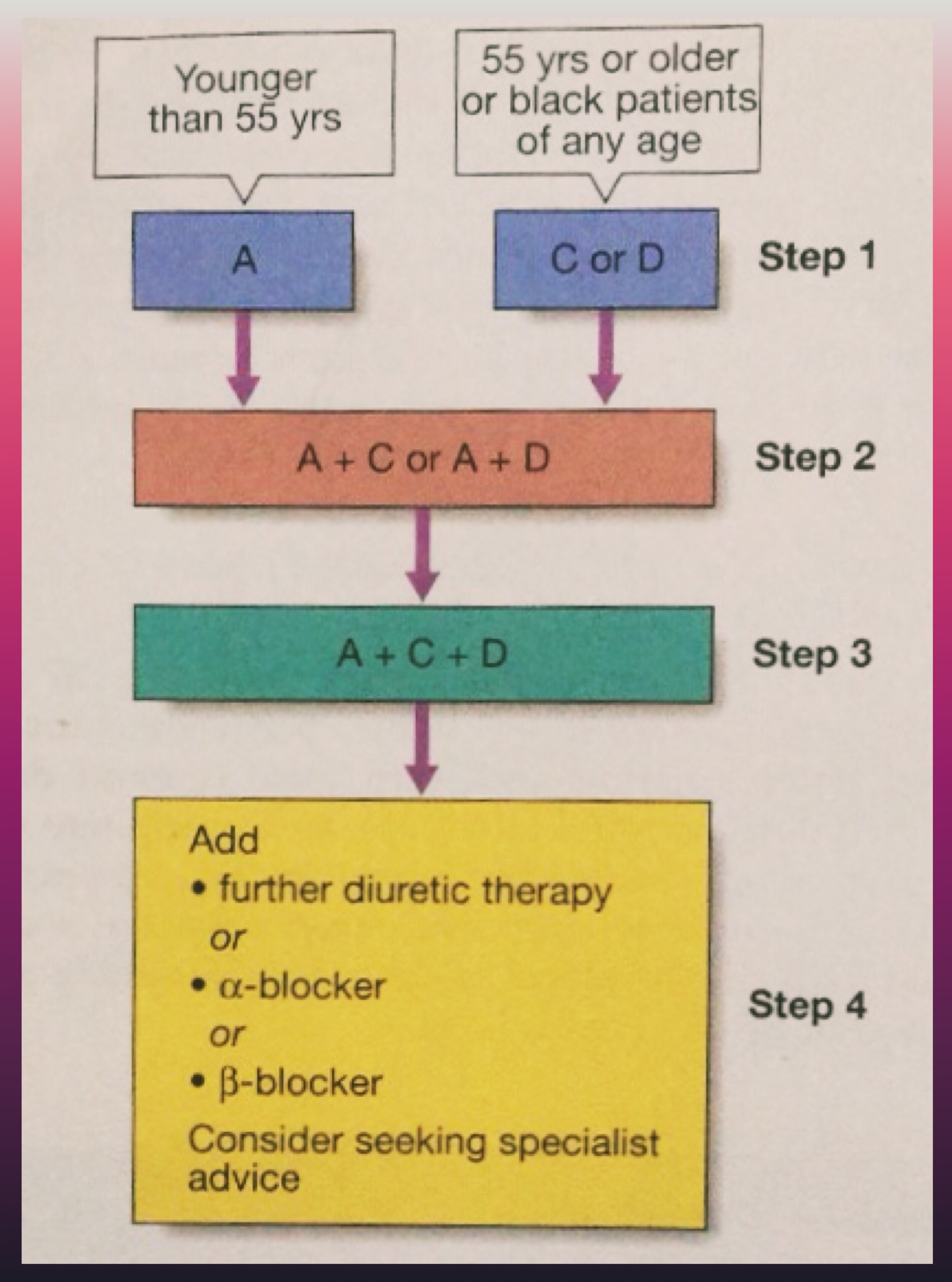
A = ACE inhibitor (consider AT-II receptor antagonist if ACE-intolerant); C = Calcium channel blocker; D = thiazide-type diuretic)
🔅 In accelerated phase HT, lowering BP too quickly may compromise tissue perfusion & can cause –
🔅150/90 mm Hg within 48 hours is ideal along with cardiac failure/hypertensive encephalopathy
🔅Avoid parenteral therapy
🔅Causes of treatment failure include:
📌Aspirin – Antiplatelet
📌Statins – Reduced risk by treating hyperlipidaemia
Dr. Mehnaz Memon🖊
References: Davidson’s Principles and Practice of Medicine Textbook

Hypertension
Definition
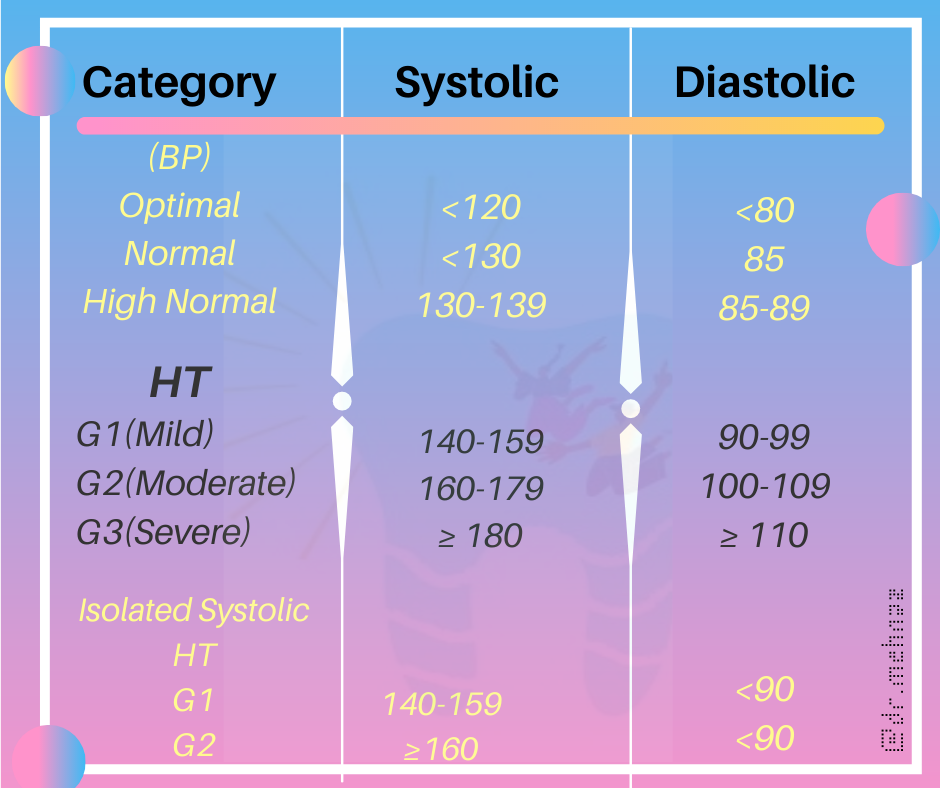
British Hypertension Society
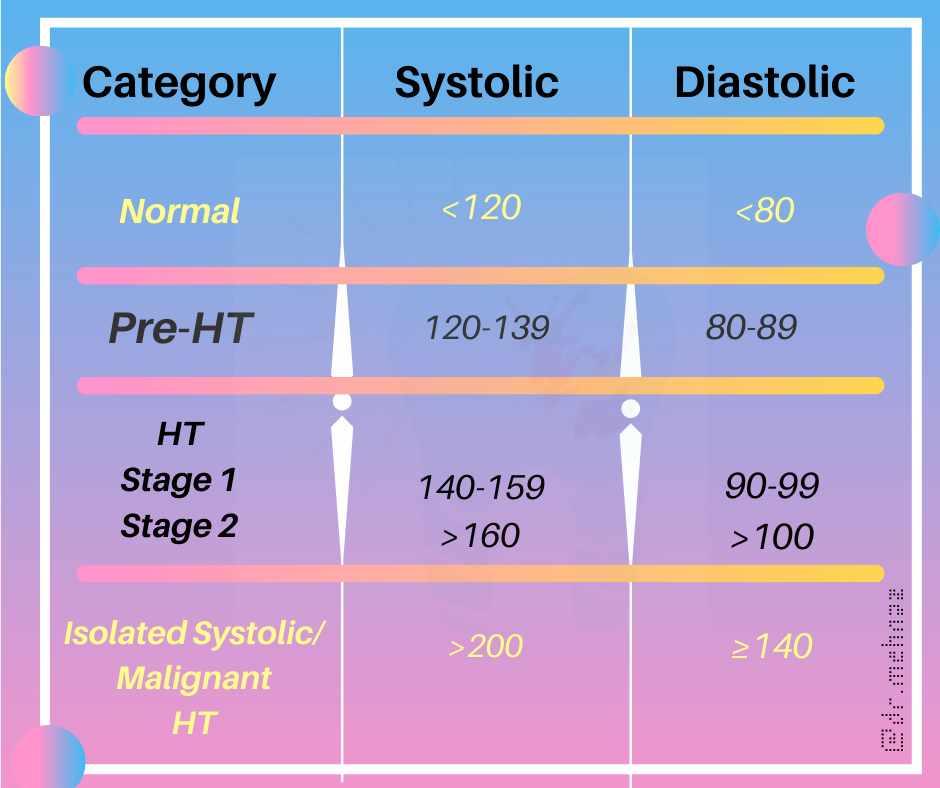
Clinical Classification
References:
Davidson’s Principles and Practice of Medicine Textbook






References:
Davidson’s Principles and Practice of Medicine Textbook


Step 1 – Choose the right equipment:
What you will need:
1. A quality stethoscope
2. An appropriately sized blood pressure cuff
3. A blood pressure measurement instrument such as an aneroid or mercury column sphygmomanometer or an automated device with a manual inflate mode.
Step 2 – Prepare the patient:Make sure the patient is relaxed by allowing 5 minutes to relax before the first reading. The patient should sit upright with their upper arm positioned so it is level with their heart and feet flat on the floor. Remove excess clothing that might interfere with the BP cuff or constrict blood flow in the arm. Be sure you and the patient refrain from talking during the reading.
Step 3 – Choose the proper BP cuff size: Most measurement errors occur by not taking the time to choose the proper cuff size. Wrap the cuff around the patient’s arm and use the INDEX line to determine if the patient’s arm circumference falls within the RANGE area. Otherwise, choose the appropriate smaller or larger cuff.
Step 4 – Place the BP cuff on the patient’s arm: Palpate/locate the brachial artery and position the BP cuff so that the ARTERY marker points to the brachial artery. Wrap the BP cuff snugly around the arm.
Step 5 – Position the stethoscope: On the same arm that you placed the BP cuff, palpate the arm at the antecubical fossa (crease of the arm) to locate the strongest pulse sounds and place the bell of the stethoscope over the brachial artery at this location.
Step 6 – Inflate the BP cuff:Begin pumping the cuff bulb as you listen to the pulse sounds. When the BP cuff has inflated enough to stop blood flow you should hear no sounds through the stethoscope. The gauge should read 30 to 40 mmHg above the person’s normal BP reading. If this value is unknown you can inflate the cuff to 160 – 180 mmHg. (If pulse sounds are heard right away, inflate to a higher pressure.)
Step 7 – Slowly Deflate the BP cuff: Begin deflation. The AHA recommends that the pressure should fall at 2 – 3 mmHg per second, anything faster may likely result in an inaccurate measurement.
Step 8 – Listen for the Systolic Reading: The first occurence of rhythmic sounds heard as blood begins to flow through the artery is the patient’s systolic pressure. This may resemble a tapping noise at first.
Step 9 – Listen for the Diastolic Reading: Continue to listen as the BP cuff pressure drops and the sounds fade. Note the gauge reading when the rhythmic sounds stop. This will be the diastolic reading.
Step 10 – Double Check for Accuracy: The AHA recommends taking a reading with both arms and averaging the readings. To check the pressure again for accuracy wait about five minutes between readings. Typically, blood pressure is higher in the mornings and lower in the evenings. If the blood pressure reading is a concern or masked or white coat hypertension is suspected, a 24 hour blood pressure study may be required to assess the patient’s overall blood pressure profile.
Further Reading/References:
https://www.suntechmed.com/support/product-training-tutorials/1692-how-to-measure-blood-pressure
