A swelling is a value term that denotes only enlargement or protuberance in body due to any cause.
According to the cause a swelling may be congenital, traumatic, inflammatory, Neoplastic or miscellaneous.
Examination of a swelling should be accompanied by a complete history of the patient. Following points should be noted:
• Duration: The clinician may ask ‘when was the swelling first
noticed’? Swellings that are painful and of shorter duration are mostly inflammatory (acute), whereas those with longer duration and without pain are chronic, e.g. a chronic periapical abscess.
• Mode of onset: The clinician may ask ‘how did the swelling start’? The history of any injury or trauma or any inflammation may contribute to the diagnosis and nature of the swelling.
• Progression: The clinician should ask ‘has the lump changed in size since it was first noticed? Benign growths such as bony swellings grow in size very slowly and may remain static for a long period of time. If the swelling decreases in size, this suggests of an inflammatory lesion.
• Site of swelling: The original site where it started must be assessed.
• Other symptoms: Pain, fever, difficulty in swallowing, difficulty in respiration, disfigurement, bleeding or pus discharge are the common symptoms associated with swellings in the orofacial region.
• Recurrence of the swelling: many swellings do recur after removal of the tissue, indicating the presence of precipitating factor, e.g. ranula.
LOCAL EXAMINATION🔍

(A) Inspection
- Situation: few swellings are peculiar in their position
- Color: Black – Naevus/Melanoma; Red/purple: Hematoma; Bluish: Ranula
- Shape: Ovoid, pear shaped, kidney shaped, spherical or irregular
- Size: Mention in cms. – the vertical horizontal dimension
- Surface: Cauliflower as in Squamous Cell Carcinoma; Filliform – Papilloma
- Edge: Sessile/pedunculated/indistinct
- Number: Multiple/diaphyseal
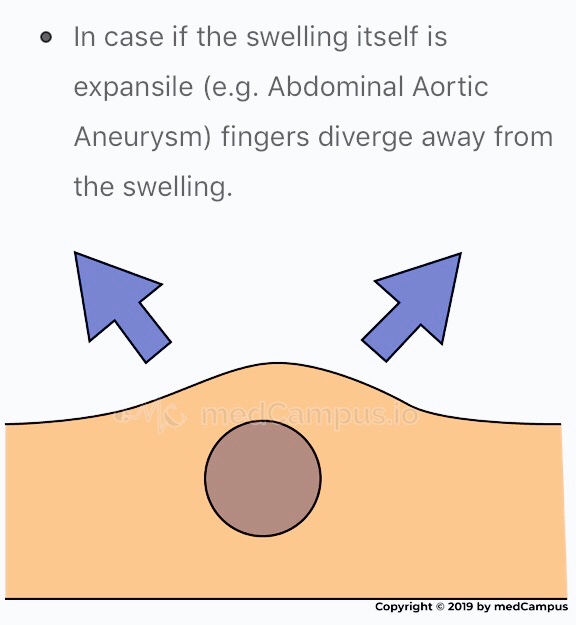
- Pulsation: The swelling which is superficial to artery, in close relation with it will be pulsatile. Pulsatile nature of swelling is assessed with 2 fingers on mass.


- Skin: Red & edematous. Pigmentation of skin is seen in moles or after repeated exposure to X-rays. Skin over a growth looks like the peel of an orange.
(B) Palpation
- Temperature: Local temperature is raised due to extensive vascularity of the swelling; best felt with back of fingers.
- Tenderness: Patient complains of pain due to pressure exerted by swelling.
- Size, shape & extent: Mention in cms. – the vertical horizontal dimension
- Fluctuation: If swelling contains liquid or gas it fluctuates.

- Translucency: contains clear fluid
- Compressibility: When pressure is applied to a swelling it decreases in size and when pressure is released swelling regains its size itself. Characteristic sign of VASCULAR HEMANGIOMA
- Reducibility: Swelling reduces and ultimately disappears when pressed upon.
Surface: Can be👇🏻
• Smooth (cystic swellings)
• Lobular with smooth lumps (lipoma)
• Nodular (multinodular goitre)
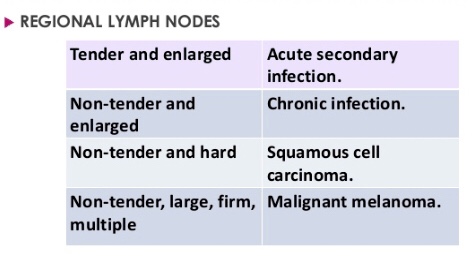
• Matted (lymph nodes)
• Irregular (carcinoma)
Margins: Well defined/indistinct👇🏻
• Malignant growth - irregular margin
• Acute inflammatory swelling - ill defined margin
• Benign tumor - swelling slips & is indistinct
Edge👇🏻
• Well defined & regular-Benign Neoplasms
• Well defined & irregular-Malignant Neoplasms
• Ill defined & diffuse - Inflammatory swellings
Consistency: 👇🏻
• Soft - lipoma
• Cystic - Cyst or chronic abscesses
• Firm - Fibroma
• Hard - Chondroma
• Bony hard - Osteoma
• Stony hard - Carcinoma
• Variable consistency - Malignancy
EXAMINATION OF ULCER:
An ulcer is break in continuity of epithelium, skin or mucous membrane. A proper
history must be taken in case of an ulcer:

• Mode of onset: The clinician may ask ‘how has the ulcer developed’? The patient may provide significant information about the nature and etiology of the ulcer such as any trauma or spontaneously.
• Duration: The clinician may ask ‘how long is the ulcer present here’? It determines the chronicity of the ulcer. For example, traumatic ulcers in oral cavity are acute (occurring for a short period), but if the agent persists; it may become a chronic ulcer.
• Pain: The clinician may ask ‘is the ulcer painful’? Most of the ulcers, being inflammatory in nature, produce pain. Painless ulcers usually suggest nerve diseases (such as peripheral neuritis, syphilis, etc).
• Discharge: Any blood, pus or serum discharge must be noted.
• Associated disease: Any associated generalized systemic problem may be associated with the ulcers of oral cavity (such as
tuberculosis, squamous cell carcinoma, etc).
LOCAL EXAMINATION🔍
(A) Inspection
Size & Shape:
• Tuberculous ulcer - oval with irregular border
• Varicose ulcer - vertical & oval in shape
• Carcinomatous ulcer - irregular
Number: Tuberculous, inflammatory ulcer may be more than one in number
Position:
• Arterial ulcer: Tip of the toes, dorsum of the foot
• Varicose ulcer: lower limb
• Perforating ulcers: over the sole at pressure points
• Non-healing ulcers: over the shin
• Rodent ulcer: upper part of face
Edge: An area between margin & floor. In spreading ulcer, edge is inflamed. Undermined edges destroy subcutaneous tissue faster than skin.


Floor: This is the part of the ulcer which is exposed or seen.
• Red granulation tissue - Healing ulcer
• Necrotic tissue, slough - spreading ulcer
• Pale, scanty granulation tissue - tuberculous ulcer
• Wash-leather slough - Gummatous ulcer
Discharge:
• Serous discharge - Healing ulcer
• Purulent discharge - Spreading ulcer
• Bloody discharge - Malignant ulcer
• Discharge with bony spicules - Osteomyelitis
• Greenish diacharge - Pseudomonas infection
(B) Palpation
Tenderness: Characteristic of infected ulcers and arterial ulcers.
Induration: The edge, base and the surrounding area should be examined for induration
• Maximum induration - Squamous cell carcinoma
• Minimal induration - Malignant melanoma
• Brawny induration - Abscess
• Cyanotic induration - Chronic venous congestion as in varicose ulcer
Mobility: Malignant ulcers are usually fixed, benign ulcers are not.
Bleeding: Malignant ulcer is friable like a cauliflower. On gentle palpation, it bleeds. Granulation tissue as in a healing ulcer also causes bleeding.
Surrounding Area:
- Thickening and induration is found in squamous cell carcinoma.
- Tenderness and pitting on pressure indicates spreading inflammation surrounding the ulcer.
Relevant Clinical Examination:
Dentowesome|@drmehnaz🖊
References:
- A Practical Manual of Public Health Dentistry by CM Marya
- Slideshare.net
- https://www.medcampus.io/mnotes/examination-of-a-swelling-transmitted-vs-expansile-pulsations-
- medinaz.com, http://www.rxpg.com
- Study Notes✍🏻