Gingivectomy means excision of the gingiva. By removing the pocket wall, gingivectomy provides visibility and accessibility for complete calculus removal and thorough smoothing of the roots, creating a favorable enviornment for gingival healing and restoration of a physiologic gingival contour.
Indications:
Elimination of suprabony pockets, regardless of their depth, if the pocket wall is fibrous & firm.
Elimination of gingival enlargements
Elimination of suprabony periodontal abscesses.
Contraindications:
The need for bone surgery
Situations in which the bottom of the pocket is apical to the mucogingival junction.
Esthetic consiserations, particularly in the anterior maxilla.
SURGICAL GINGIVECTOMY
Armamentarium:
Mouth mirror, probe
Pocket markers, Kirkland and orban interdental gingivectomy knives
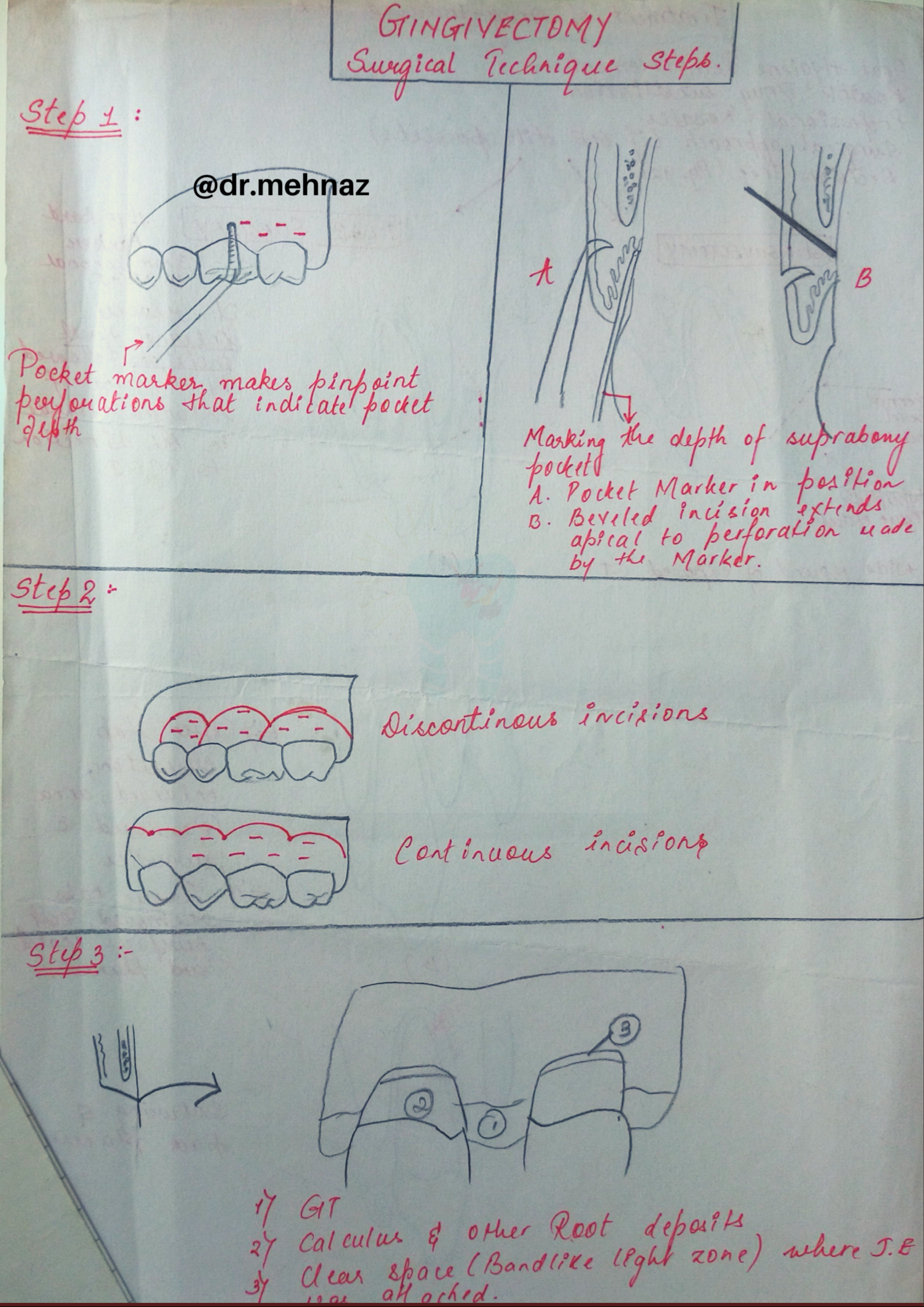
Step 1: The pockets on each surface are explored with a periodontal probe and marked with a pocket marker.
Step 2: The incision is started apical to the points marking the course of the pockets and is directed coronally to a point between the base of the pocket and the crest of the bone.
Step 3: Remove the excised pocket wall, clean the area, and closely examine the root surface.
Step 4: Carefully curette the granulation tissue, and remove any remaining calculus and necrotic cementum so as to leave a smooth & clean surface.
Presentation Tip💡: Try to present your answers with flowcharts & diagrams rather than long paragraphs!! It will definitely have more impact & help you score well in exams..👍👇🏻
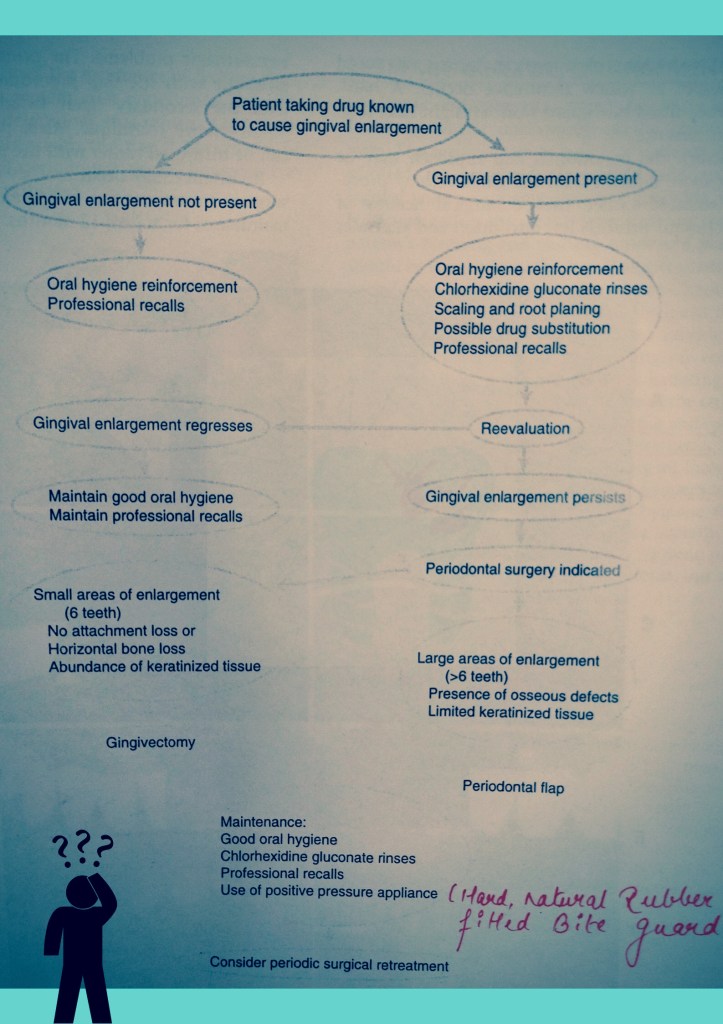
Surgical Approach (Diagrammatic View); MGJ: Muco-gingival junction; BL: Bucco-lingual; CT: Connective TissueDecision Tree fortreatment of Drug-Associated Gingival Enlargement
Source: Carranza’s Clinical Periodontolgy, 10th Ed
• Types of giant cells - grossly classified into 2 types. – • The giant cells which exist in normal tissue (physiological) e.g osteoclasts in bones, trophoblasts in placenta, odontoclast, straited muscle.
• The giant cells which exist pathological -eg. Foreign body giant cells Langhan's giant cells Touton giant cells Aschoff giant cells Anaplastic cancer giant cells Reed-Sternberg giant cells
Curated by: Dr. Tabassum Sayyad (Dental Intern – MARDC)
PA radiolucencies identification made easy! Happy learning..😀📖
Periapical radiolucencies are most commonly odontogenic. Nonodontogenic radiolucencies tend to be not localized and span across the mandible or maxilla within the alveolus and sometimes extend inter-radicularly.
The most common PA pathologies can be diagnosed based on the vitality responses from the teeth. Ruling out the tooth associated pathologies is an important step in securing a diagnosis from differential diagnosis panel of PA radiolucencies.
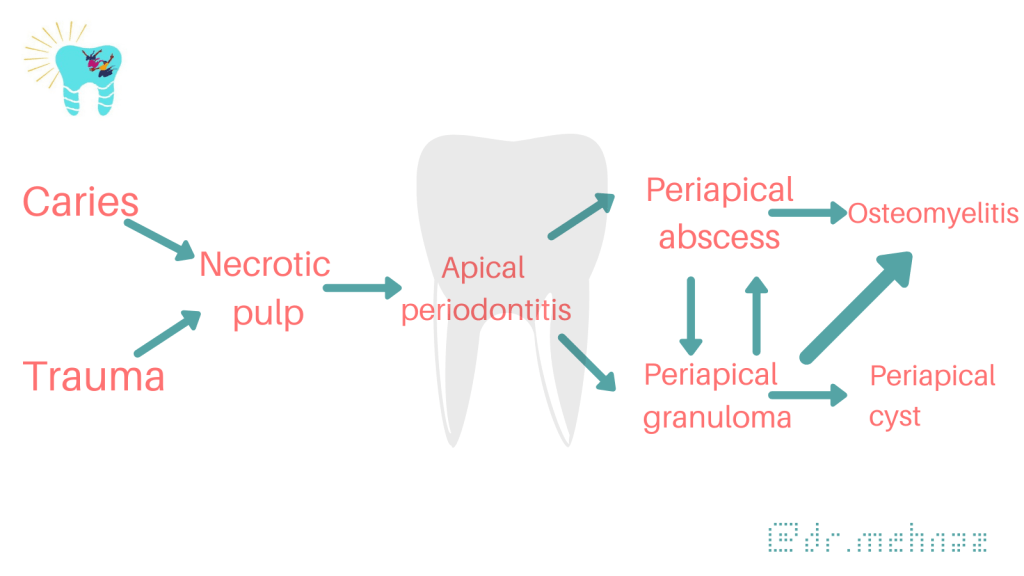
Inter-relationship of possible results of periapical inflammation:
When formulating radiological differential diagnosis, features should be evaluated carefully, such as
location
locularity
relation to dentition
density of lesion
margin
type of radiological change (radiolucent/radiopaque/mixed)
periosteal reaction
cortical integrity, and
clinical presentation.
🌫 General Radiographic features:
• Location: With periapical inflammatory lesions, which are pathological conditions of the pulp, the epicenter typically is located at the apex of a tooth.
• Periphery: Ill defined
• Effects on surrounding structures: Periapical lesions cause widening of PDL space at apical region of the root.
PA Radiolucencies: (Classification)
PERIAPICAL RADIOLUCENCIES
Developmental
Lateral periodontal cyst
Definition: lateral periodontal cysts are cystic lesions that tend to occur on the lateral aspect of vital teeth. Epidemiology: lateral periodontal cysts account for fewer than 1% of the reported cases of odontogenic cysts.
Clinical findings: most lateral periodontal cysts area located in the mandibular incisor-canine-premolar area.
Radiographic findings: radiographically, lateral periodontal cysts present as a unilocular radiolucent lesion between the roots of teeth or associated with the lateral aspect of a tooth.
Management: surgical enucleation with preservation of involved teeth is an appropriate treatment of lateral periodontal cysts. Recurrence is rare. The multiloculated variant called botryoid odontogenic cysts has been reported to demonstrate a higher recurrence rate than its unilocular counterpart.
Inflammatory Lesions
Apical periodontitis, periapical abscess
Definition: spectrum of inflammation involving the PA area of teeth that results from pulpal infection by microorganisms.
Epidemiology: apical periodontitis is the most frequent inflammatory lesion related to teeth in the jaws.
Clinical findings: apical periodontitis can be classified as either asymptomatic or symptomatic; clinical examination of percussion and palpation of the tooth yields negative results in the former and usually positive results in the latter. The results of pulp sensitivity tests for both conditions, however, are negative. In the early stage of PA inflammation, the PA PDL can exhibit acute inflammation without abscess formation. This localized alteration may or may not proceed to abscess formation.
Radiographic findings: in apical periodontitis, radiographs may show a thickened PDL space. If an abscess develops after a long-standing apical periodontitis, radiographs reveal a radiolucent area around the root apex.
Management: apical periodontitis is an inflammatory disease caused by a persistent infection of the root canal system. The recommended treatment is the removal of the dead nerve and bacteria either through extraction of the tooth or root canal treatment. Antibiotics are recommended only when there is severe infection that has spread from the tooth into the surrounding tissues.
Mandibular left molar PA radiograph showing the initial apical changes in relation to the first molar secondary to a symptomatic gross carious lesion. If the offending causes remain, this will continue to an apical osteitis, resulting in loss of trabecular bone and possibly even cortical bone before it shows up radiographically.Cropped panoramic radiograph showing localized osteomyelitis secondary to PA infection in relation to the mandibular left first and second molars (arrows).
Cystic Lesions
Periapical (radicular) cyst
Definition: radicular cyst is a cyst of inflammatory origin associated with a nonvital tooth.
Epidemiology: radicular cysts represent the most common odontogenic cyst. Radicular cysts are most commonly associated with at the tooth apex, but a lateral radicular cyst can be associated with a lateral root canal.
Clinical findings: radicular cysts are always associated with a nonvital tooth, and this is an important criterion for diagnosis.
Radiographic findings: radiographs often show a well-defined radiolucent lesion at the apex of a tooth. Radicular cysts can displace or resorb the roots of adjacent teeth.
Management: the treatment of radicular cysts can include nonsurgical root canal therapy to surgical treatment, such as apicoectomy.
Odontogenic keratocyst
CBCT panoramic reconstruction of maxilla showing a large well-defined lytic area coronal to the impacted right canine. Histologically confirmed as an odontogenic keratocyst.
Definition: an odontogenic cystic lesion with distinctive histologic features. Recently reclassified back into a cystic category in the recent 2017 WHO Classification of Head and Neck Tumours. Current evidence seemed lacking to justify the continuation of classifying it as a tumor.
Epidemiology: odontogenic keratocysts are the third most common cyst of the jaws.
Clinical findings: most common location of odontogenic keratocysts is the mandibular molar region.
Radiographic findings: odontogenic keratocyst size can be variable, ranging from a unilocular radiolucent lesion surrounding the crown of an unerupted tooth, resembling a dentigerous cyst, to a large size that results in facial deformity and destruction of surrounding structures. Lesions tend to grow in a posteroanterior direction, however, that results in a lack of cortical expansion.
Management: odontogenic keratocysts tend to be more aggressive in its growth pattern with a higher recurrence rate than other odontogenic cysts. Recurrence may be due, however, to incomplete removal or the presence of satellite (daughter) cysts. Treatment includes enucleation (with or without peripheral ostectomy, treatment with Carnoy solution), marsupialization, or resection.
Glandular odontogenic cyst
Definition: a developmental cyst with features that resemble glandular differentiation.
Epidemiology: glandular odontogenic cysts represent less than 1% of odontogenic cysts.
Clinical findings: there is a predilection for the mandible.But in the maxilla, the canine seems commonly involved. Swelling and expansion were the most common presenting complaints.
Radiographic findings: radiographically, glandular odontogenic cysts present as a well-defined unilocular or multilocular radiolucency associated with the roots of teeth; association with impacted teeth is rare.
Management: glandular odontogenic cysts have a tendency to recur especially when lesions are removed with simple enucleation.
Benign Tumors
Ameloblastoma
Definition: benign, slow-growing epithelial odontogenic neoplasm with unmitigated growth potential.
Epidemiology: ameloblastomas are the most common odontogenic tumors, excluding odontomas.89 In the United States, African Americans seem to have an overall 5-fold increase risk of disease compared with whites.
Clinical findings: tumor often presents as an asymptomatic swelling of the posterior mandible and can be associated with an unerupted tooth. Buccal and lingual expansion often is observed.
Radiographic findings: radiographs commonly show corticated multilocular (soap- bubble) radiolucency.
Management: the unmitigated growth potential and tendency to recur require operative management involving segmental or marginal resection. When treated by enucleation alone, much higher rates of recurrence are reported.
Panoramic radiograph showing a large well-defined, multilocular radiolucency extending from the area of first molar on the left into the ramus area. Note the expansion and thinning of the cortices. Ameloblastoma was confirmed histologically.
Malignant Tumors
Ameloblastic carcinoma
Definition: a rare, malignant counterpart for ameloblastoma. Not to be confused with metastasizing ameloblastoma, this is a histologically benign ameloblastoma metastasizing to distant sites. In the recent WHO Classification of Head and Neck Tumours, metastasizing ameloblastoma has been separated from ameloblastic carcinoma and included as a type of conventional ameloblastoma.
Epidemiology: incidence rate was 1.79 per 10 million person/year with male and black population predominance. The overall survival is 17.6 years.
Clinical findings: the most common site is the posterior mandible. Often, pain and expansion are the first clinical manifestations. Most cases arise de novo, but some arise in preexisting ameloblastomas.
Radiographic findings: radiographically, ameloblastic carcinomas can present as poorly defined, irregular radiolucencies consistent with a malignancy, or indistinguish- able from a benign radiolucency.
Management: generally considered radio-resistant tumor, radical surgical resection is the first line of treatment.
Differential Diagnosis: 🔍
The 2 type of lesions that most often must be differentiated from periapical inflammatory lesions are Periapicalcemental dysplasia & enostosis (dense bone island, osteosclerosis) at the apex of the tooth.
In the early radiolucent phase of Periapical cemental dysplasia, the D/D rely solely on clinical examination and a test of tooth vitality.
With long standing periapical inflammatory lesions, the pulp chamber of involved tooth may be wider than adjacent tooth.
More mature PCD show radio-opaque mass within radiolucent area which helps in D/D.
Also the common site for PCD is mandibular anterior region. External root resorption is more common with periapical inflammatory lesions than PCD.
When enostosis is centered on the root apex, it may mimic inflammatory lesion but the PDL space has normal width. Also the periphery of enostosis is well defined and does not blend with surrounding trabaculae.
Small radiolucent periapical lesions with well-defined periphery may be either granulomas/cysts.
Differentiation may not be possible unless other characteristics of cyst such as displacement and expansion of surrounding structure is not present.
Larger lesions >1cm are usually radicular cysts.
If the patient has had endodontic treatment or apical surgery, a periapical radiolucency may remain that resemble periapical rarefying osteitis.
Metastatic lesions such as leukemia may grow in periapical segment of PDL space with malignant bone destruction.
Periapical radiographs of case showing Enostosis (see arrows) in the mandibular left quadrant, in close proximity with the roots of the adjacent teeth
Enostosis are common findings that seldom require treatment; however, caution should be exercised when undertaking orthodontic movement in the area of a DBI due to a potential risk of root resorption. Accurate identification and multidisciplinary management are of utmost importance. Monitoring size changes is recommended until completion of patient’s growth.
The extraction of a tooth requires the separation of its attachment to the alveolar bone via the crestal and principal fibers of the periodontal ligament. Also involved is a process of expanding the alveolar socket.
After the tooth has been removed, the form of alveolar process is restored by finger pressure. Bleeding is arrested by means of a pressure pack placed between the jaws, and the wound is allowed to fill with a blood clot.
EXODONTIC PROCEDURES:
The following techniques may be used for tooth removal:
Odontotomy can be used to facilitate any of these three procedures.
ODONTOTOMY
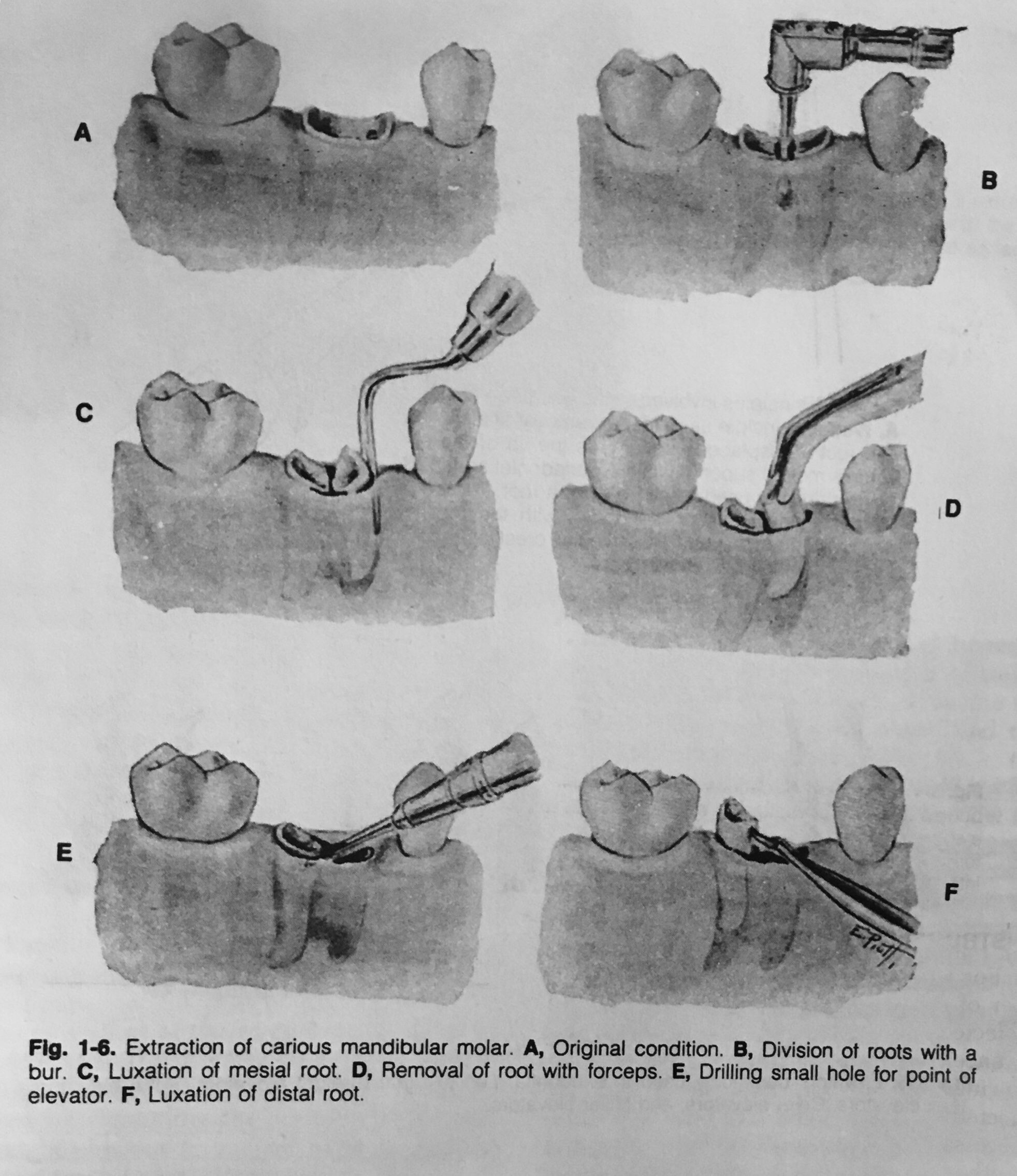
In some instances the extraction may be simplified by cutting a tooth apart. This is especially desirable in the case of multi-rooted deciduous or permanent teeth with severely divergent roots.
It is also useful in cases where the crown is so decayed that only a shell remains. (As shown in the figure👇🏻)
Extraction of carious molar by odontotomy
If the roots are divergent, the bur cut, instead of being vertical, may be made parallel with one of the roots, and this part of the tooth then is extracted first.
The other roots may be removed either with forceps or an elevator.
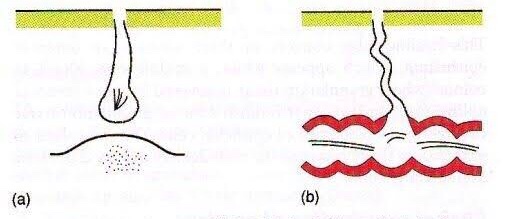
A sinus is a blind tract leading from the surface down to the tissue. There may be a cavity in the tissue which is connected to the surface through a sinus. The sinus is lined by granulation tissue which may be epithelized.
A sinus has one open draining end and the channel ends in a blind ending. An example would be a dental sinus draining from a dental abscess to either the inside of the mouth or the skin.
Clinical Tip – 💡The Sinus tract will lead you to the cause!
Fistula
Latin: flute(or) a pipe (or) a tube
It is a communicating tract between 2 epithelial surfaces commonly between hollow viscous & skin or between 2 hollow viscera. The tract is lined by granulation tissue which is subsequently epithelized. A fistula may be an abnormal communication between vessels.
An example would be from the mouth (oral cavity) to the skin surface, usually of the face or neck, and this specific type is called an orocutaneous fistula.
These defects can cause aesthetic and functional problems due to the continuous leakage of saliva.It is an abnormal epithelized communcation between maxillary sinus and oral cavity through perforation in the sinus wall
Fistulas and sinuses of the neck and face: classification
Fistulas and sinuses of the neck and face may be classified by cause.
Developmental
Fistulas and sinuses due to developmental causes are usually present at birth.
Thyroglossal duct cyst – the most common developmental cyst in the neck. The cyst characteristically moves upwards when the tongue is poked out or with swallowing. It may burst to form a sinus which usually opens just below the hyoid bone in the midline of the neck. It drains mucus.
Branchial cleft cyst – the most common developmental cyst of the side of the neck. A sinus may drain mucus or pus following rupture of an abscess. It usually opens on the side of the neck.
Preauricular sinus
Cysts
Cysts are lumps in the skin containing fluctuant contents. They may have an opening to the skin surface.
Dermoid cyst
Epidermal cyst
Traumatic
Accidental
Radiotherapy
Surgical
Infective
Actinomycosis
Bone infection Chronic osteomyelitis – most commonly associated with poorly controlled diabetes mellitus or following radiotherapy to the jaw for cancer or Paget disease of the bone. It may also complicate a chronic dental infection.
Dental infection
Chronic dentoalveolar abscess
Dental implant
Failed endodontic procedure
Lymph node
Cat scratch disease
Dental infection
Tuberculosis (scrofuloderma)
Neoplastic
Oral squamous cell carcinoma is the most common
Benign tumours of the mouth rarely form a fistula
Causes for persistence of sinus/fistula
Presence of a foreign body e.g. suture material
Presence of a necrotic tissue underneath e.g. sequestrum
Insufficient or non-dependent drainage. e.g. TB sinus
Distal obstruction e.g. biliary fistula
Persistant drainage like urine/faeces/CSF
Lack of rest
Epithelialisation of the tract e.g. AVF
Malignancy
Dense fibrosis
Irradiation
Malnutrition
Specific causes e.g. TB, actinomycosis
Ischemia
Drugs e.g. steroids
Interference by the patient
How is a fistula or sinus diagnosed?
In addition to careful history and examination, one or more of the following tests will usually be required to confirm the diagnosis and determine the cause:
passing a probe into the channel
radiology – may include plain x-rays, x-rays using contrast medium, CT or MRI scans
microbiological assessment of swabs or biopsy material
biopsy and pathology
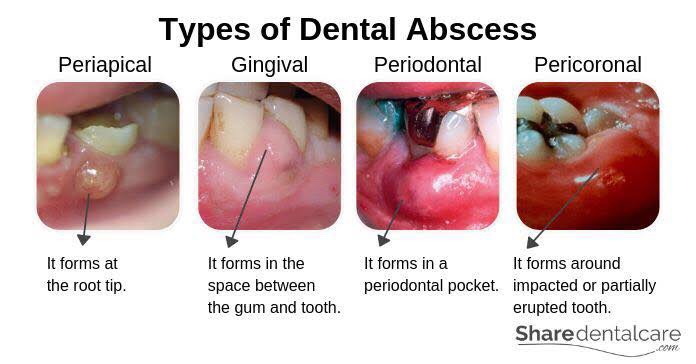
Abscess
Collection of pus
Clinical Features & Diagnosis:
Features of acute inflammation; The four cardinal signs of inflammation are:
redness (Latin rubor) – below localization of abscess
heat (calor) – inflammed area is hot
swelling (tumor) – pus present inside abscess cavity
and pain (dolor) – throbbing type
Diagnosis of Dental Abscess:
The location of abscess will cause tenderness with palpation test
The abscessed tooth will be very sensitive to percussion
IOPA findings will suggest slight thickening of PDL space with radiolucency at apex