
Osteogenesis Imperfecta(Types)






References: Shafer’sTextbook Of Oral Pathology
Source: KD Tripathi textbook




References: Shafer’sTextbook Of Oral Pathology; Image source: Google
• Composed of proliferating odontogenic epithelium in a cellular ectomesenchyme resembling the dental papilla.
• Odontomas are composed of all mature components of dental hard & soft tissues: Enamel, dentin & pulp.
• Because of their limited slow growth and well differentiation – considered hamartomas rather than true neoplasms
Clinical Features:
1. Interfere with eruption of permanent teeth.
2. No sex predilection
3. Age: 2nd decades
4. Asymptomatic in nature
5. Associated with impacted, malpositioned teeth.
6. Cause malformation and displacement of adjacent teeth

• Location: Posterior region of either Jaw. (70% – Mandibular Molars)
• Composed of haphazardly arranged dental hard and soft tissue with no resemblance to normal tooth.
• Arises from normal tooth follicle.
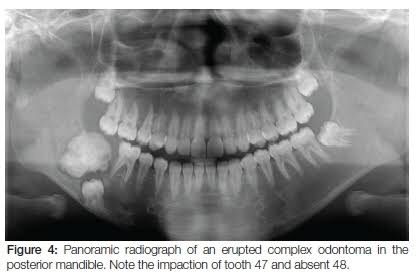
• Radiographically, Sunburst opacities with thin uniform radiolucent rim.
• Location: Anterior maxilla (62% – unerupted canine)

• Collection of small radio-opaque masses, some/all may be tooth like structures “denticles“
• Formed by exuberant growth of dental lamina or proliferation of enamel organ
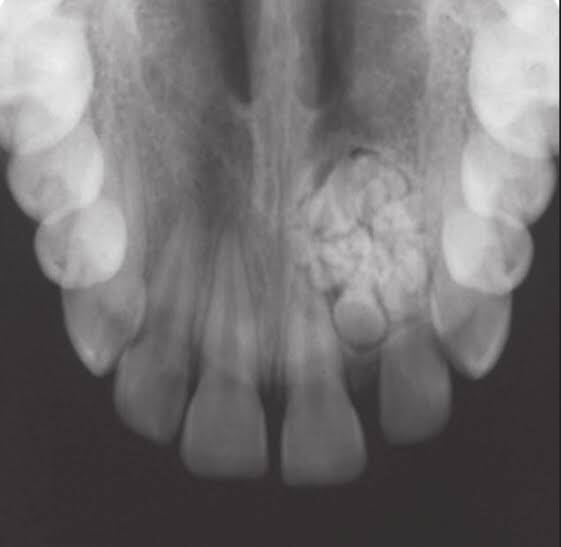
• Radiographically, cluster of multiple tiny toothlike structure within a fine radiolucent rim.

• Connective tissue capsule around odontoma is similar in all aspects to follicle surrounding normal tooth.
• Presence of ghost cells also found.
Treatment: Surgical Removal
References: Shafer’sTextbook Of Oral Pathology; Random google images


References: Shafer’sTextbook Of Oral Pathology; Random google images
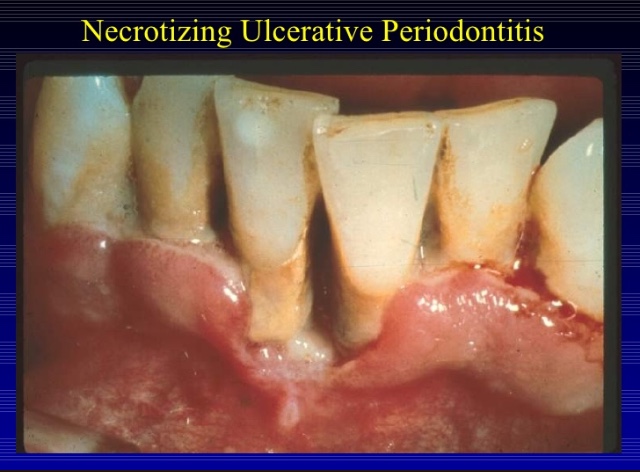
⦿ Necrotizing ulcerative periodontitis may be an extension of necrotizing ulcerative gingivitis into the periodontal structures, leading to periodontal attachment and bone loss.
⦿ It is characterized by soft tissue necrosis, rapid periodontal destruction, and inter-proximal bone loss.
RISK FACTORS:
CLINICAL PRESENTATION:
POPULATION:
⦿ Usually: young adults(age 18-30); sometimes: malnourished children or immunocompromised individuals.
Symptoms: Intense, excruciating pain
SIGNS:
⦿ Similar to NUG, clinical cases of NUP are defined by necrosis and ulceration of the coronal portion of the interdental papilla and gingival margin, with a painful bright red marginal gingiva that bleeds easily.
⦿ Severe loss of periodontal attachment.
⦿ Deep interdental osseous craters typify periodontal lesions of NUP.
⦿ Deep pocket formation is not evident because the ulcerative and necrotizing nature of the gingival lesion destroys the marginal epithelium and connective tissue, resulting in gingival rescession.
⦿ Advanced lesions lead to severe bone loss, tooth mobility and ultimately tooth loss.
⦿ Oral malodor, fever, malaise or lymphadenopathy may occur.
⦿ Characteristic microbiota: fusiform bacteria, P Internedia, P gingivalis, Treponema sp., and C.Albicans.
HIV/AIDS Patient:
⦿ Linear gingival erythema, NUG and NUP are the most common HIV- associated periodontal conditions.
⦿ NUP lesions in AIDS patients can be much more destructive and frequently result in complicatons that are extremely rare in non AIDS patient.

HIV POSITIVE NUP:
⦿ PRESENTATION:
⦿ Periodontal attachment and bone loss may be extremely rapid.
⦿ Progression of the lesions to involve large areas of soft tissue necrosis, with exposure of bone and sequestration of bone fragments.
⦿ This type of severe, progressive lesion with extension into the vestibular area and the palate is referred to as necrotizing ulcerative stomatitis.
INVESTIGATION:
⦿ Obtain a detailed M/H, including nutrition and health habits.
⦿ Medical consult to rule out any immunosuppressive disease may be necessary. NUP has been associated with HIV+ve and AIDS patient.
⦿ Obtain a dental history: previous history of NUG/periodontal disease., foul metallic taste, pasty saliva, intense excruciating pain.
⦿ Perform an extraoral examination: check for lymphadenopathy in the head and neck, facial asymmetry.
⦿ Perform an intraoral examination: look for C/F of NUP.
DIFFERENTIAL DIAGNOSIS:
TREATMENT:
⦿ Common initial treatments:
FOLLOW UP
References: Essentials Of Periodontology by S Sahitya Reddy; Carranza’s clinical periodontology; Internet images
Also termed:
Etiology:
1. Role of bacteria:
2. Predisposing factors:
| LOCAL | SYSTEMIC |
| Smoking | Poor nutritional status |
| Psychological stress | Leukemia, AIDS |
| Poor oral hygiene | Syphilis |
| Marginal gingivitis | Aplastic Anemia |
| Faulty restoration | Vitamin C, B2 deficiency |
| Deep periodontal pockets | Inadequate sleep |
| Local trauma | Immunosuppressant |
Clinical Features:
1. Age: Young & Middle-aged
2. No sex predilection
3. Site:
a. Interdental papillae
b. Free gingival margin
c. Crest of gingiva
d. Soft palate & tonsillar areas-Vincent’s Angina
4. Diagnostic Triad –
| Pain |
| Interdental ulceration |
| Gingival bleeding |

5. Signs & Symptoms:
a. Onset is sudden with pain, tenderness, profuse salivation & peculiar metallic taste.
b. Spontaneous bleeding
c. Fetid Odor
d. The interdental papillae are blunted, inflamed, edematous and hemorrhagic. Show Punched out crater like necrotic areas covered by grayish pseudo membrane
e. Lymphadenopathy, fever & malaise
f. Involvement of PDL leads to NUP
g. Cancrum oris (Noma)
h. Gingiva is stained and teeth seem slightly to be extruded & moveable
i. Patient is unable to eat properly


• Histopathology:
– Interdental papillae show surface ulceration covered by a fibrinopurulent membrane.
– Underlying connective tissue shows acute/mixed inflammatory infiltrate along with extensive hyperemia.
• Treatment:
ANUG results from impaired host response to a potentially pathogenic microflora. Compared to other PDL diseases, ANUG resolves quickly after removal of bacterial infection.
1. Alleviation of acute inflammation by reducing the microbial load and removal of necrotic tissue.
2. Treatment of underlying chronic disease.
3. Alleviation of generalized symptoms.
4. Correction of systemic conditions or factors that contribute to the initiation and progression of gingival changes.
Sequence of treatment:
First Visit:
– Evaluation
– Comprehensive medical history
– H/O acute disease its onset and duration
– Examination of the patient’s oral cavity
Treatment of acutely involved areas:
– Isolate with cotton rolls. Apply topical anesthetic and after 2-3 min. the area are gently swabbed with moistened cotton pellet to remove pseudo membrane and surface debris.
– Cleanse the area with warm water and remove superficial calculus with ultrasonics.
– Contraindication:
• Subgingival scaling & curretage.
• Extractions & surgery
– 4 weeks: Waiting Period
– Patient with severe cases, lymphadenopathy/other systemic conditions – Antibiotic regimen (Amoxycillin, erythromycin & Metronidazole) & NSAID’s.
Patient Instructions:
1. Avoid tobacco, alcohol
2. Rinse with a glassful of an equal mixture of 3% H2O2 and warm water every 2 hours or twice daily with 0.12% chlorhexidine solution.
3. Get adequate rest. Avoid exertion
4. Brushing with ultrasoft brush with a bland dentifrice for removal of surface debris only.
5. Follow-up after 1-2 days.
• Second visit:
– Evaluate the condition
– Pain usually subsides but the gingival margins are still erythematous.
– Scaling can be done
– Follow-up after 5 days
• Third visit:
– Plan for the management of patient’s periodontal conditions.
– Plaque control procedures
– Nutrition
– Cessation of habit
– Chlorhexidine rinses for 2-3 weeks
– Recall after a month.
References: Essentials Of Periodontology by S Sahitya Reddy; Carranza’s clinical periodontology; Internet images
HABIT– It’s a tendency towards an act that has become a repeated performance either fixed, consistent and easy to perform by an individual.HABITS which do not apply a direct force on the teeth or its supporting structures are termed non-pressure habits. An example of a non-pressure habit is mouth breathing.
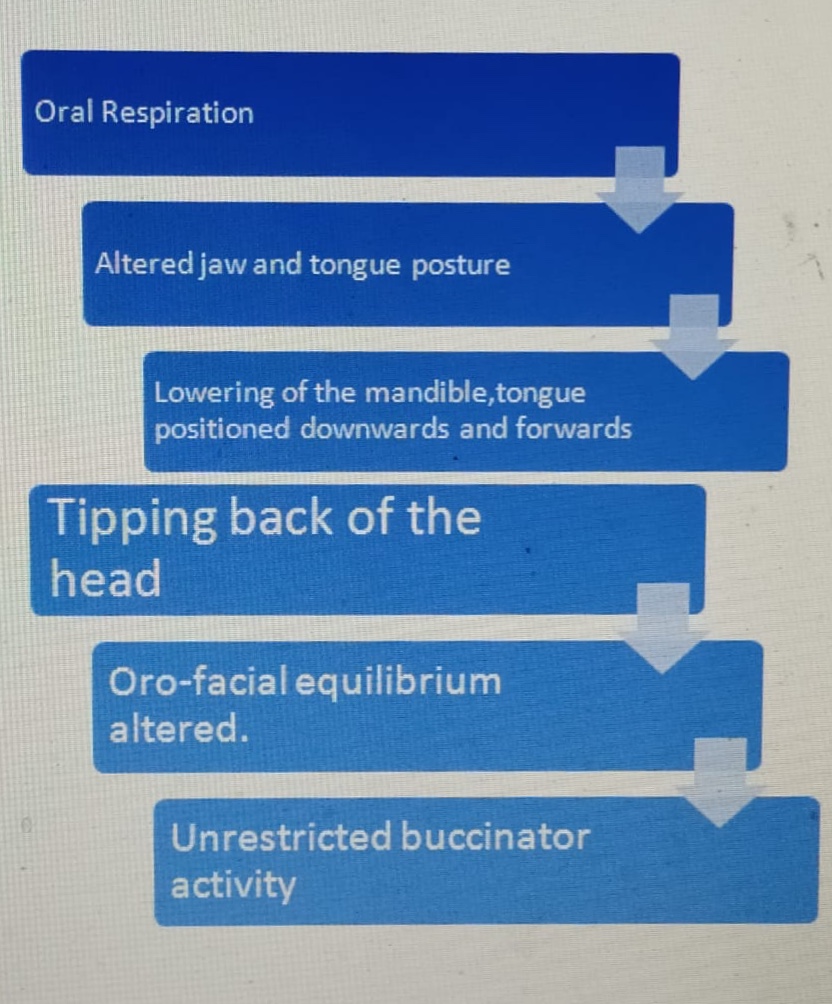
MOUTH BREATHING HABIT– Habitual respiration through the mouth instead of the nose. It’s a possible etiological factor for malocclusion. The mode of respiration influences the posture of the jaw, the tongue and to a lesser extent the head. Thus mouth breathing could alter the oro-facial equilibrium thereby leading to malocclusion. Most normal people indulge in mouth breathing when they are under physical exertion such as during strenuous exercise or sports activity.
Classification based on etiology of Mouth breathing:
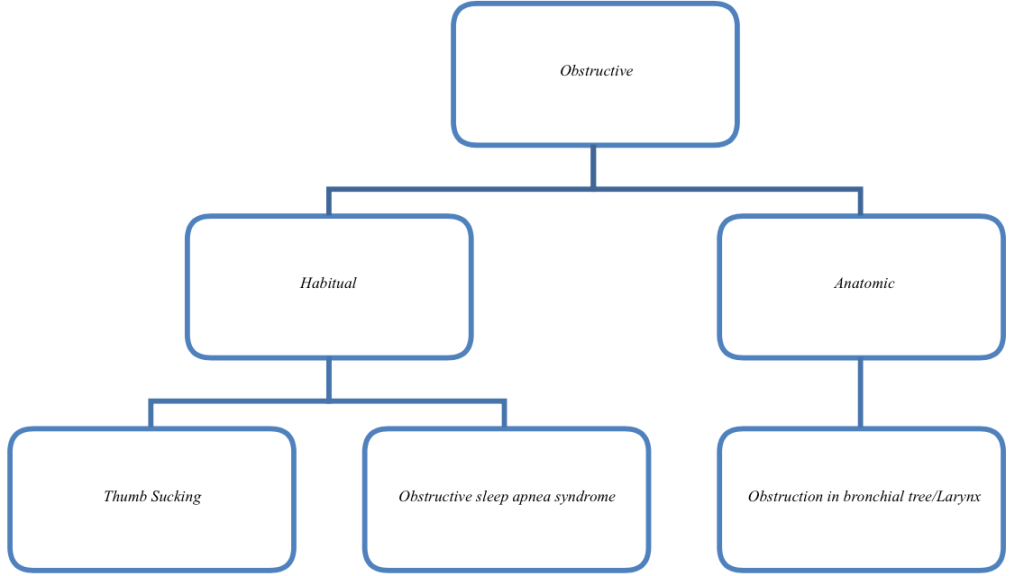
Mouth breathers can be classified into 3 types:
a. OBSTRUCTIVE–Causes of nasal obstruction:
-Enlarged Turbinates
-Enlarged Adenoids
-Deviated Nasal Septum
-Nasal polyps
-Allergic Rhinitis
-Chronic inflammation of nasal mucosa
-Benign tumors.
Ectomorphic children with tapering face and nasopharynx-Genetics-prone to develop nasal obstruction.
b. HABITUAL: A habitual mouth breather is one who continues to breathe through his mouth even though the nasal obstruction is removed. It becomes a deep rooted habit that is performed unconsciously.
c. ANATOMIC: Abnormally short upper lip preventing proper lip seal.
PATHOPHYSIOLOGY:
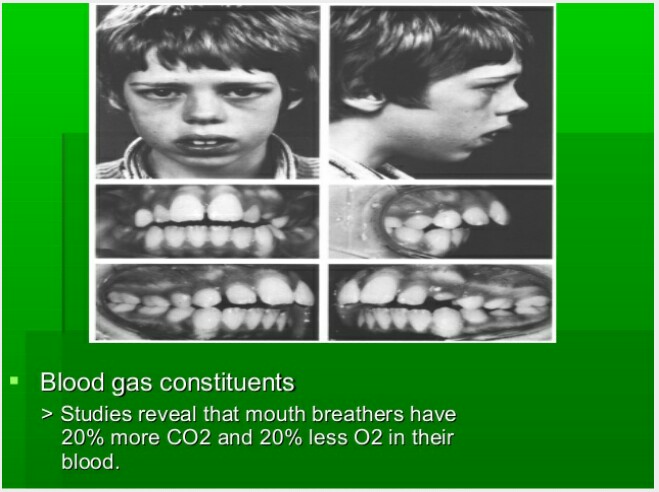
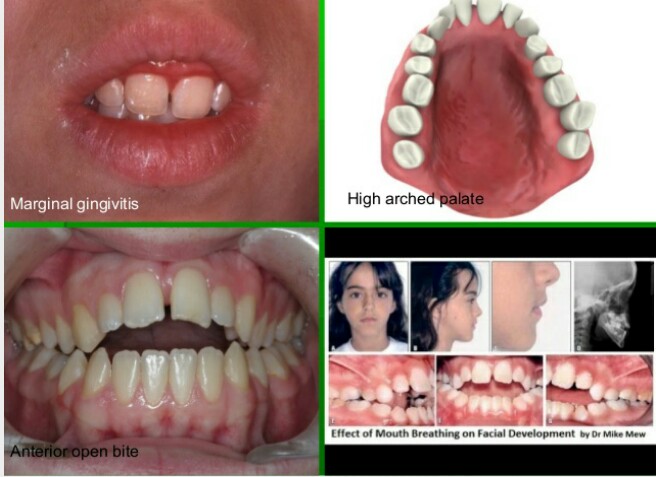
CLINICAL FEATURES OF MOUTH BREATHING: The type of malocclusion most often associated with mouth breathing is called long face syndrome or the classic adenoid facies. These patients exhibit the following features:
a. Long and narrow face.
b.Narrow nose and nasal passage.
c. Short and flaccid upper lipd.
d. Contracted upper arch with possibility of posterior cross bite
e. An expressionless face
f. Increased overjet as a result of flaring of the incisors.
g. Anterior marginal gingivitis can occur due to drying of the gingiva.
h. The dryness of the mouth predisposes to caries.
i. Anterior open bite can occur
DIAGNOSIS OF MOUTH BREATHING:
History: A good history should be recorded from the patient as well as parents.
Clinical examination: Look out for its various clinical features. A number of simple tests can be carried out to diagnose mouth breathing such as mirror test, water test etc.
a. Mirror test: Also called as fog test. A double sided mirror is held between the nose and mouth. Fogging on the nasal side indicates nasal breath while fogging on oral side-mouth breathing.
b. Massler’s water holding test: Patient is asked to hold the mouth full of water.


Cephalometrics: Cephalometric examination helps in establishing the amount of nasopharyngeal space, size of adenoids and also helps in diagnosing long face associated with mouth breathing.
Rhinomanometry: It is the study of nasal airflow characteristics using devices consisting of flow meters and pressure gauges. These devices help in estimation of airflow through the nasal passage and nasal resistance.
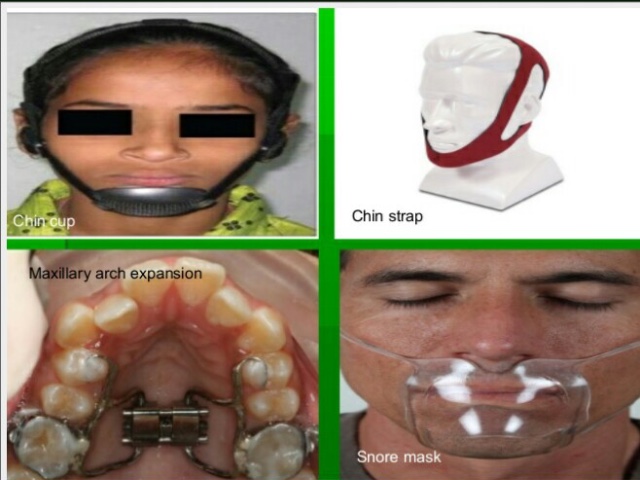
MANAGEMENT:
1. Removal of nasal or pharyngeal obstruction: Any nasal or pharyngeal obstruction should be removed by referring the patient to the E.N.T surgeon.
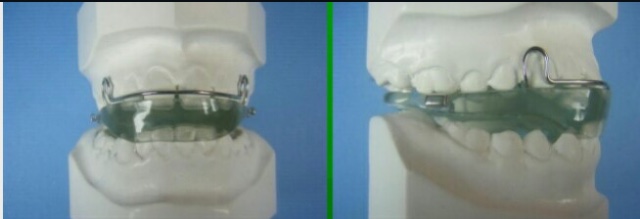
2. Interception of the habit:
3. Rapid Maxillary Expansion:
Patients with narrow, constricted maxillary arches benefit from rapid palatal expansion procedures aimed at widening the arch.RME has been found to increase the nasal airflow and decrease the nasal air resistance.
4. Correction of malocclusion:


References: Textbook of Orthodontics The Art and Science 6th Edition By Bhalajhi! Random google images.
Source: Internet
