🔷 Local Complications:
- Needle breakage
- Persistant anesthesia or paresthesia
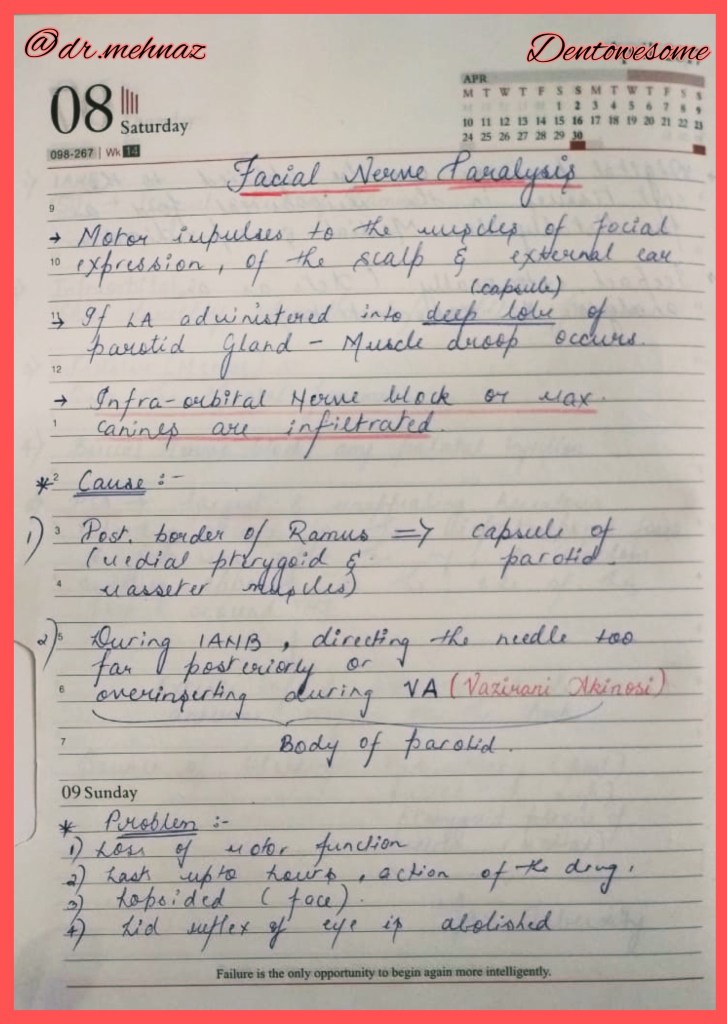
- Facial Nerve Paralysis
- Trismus
- Soft-tissue injury
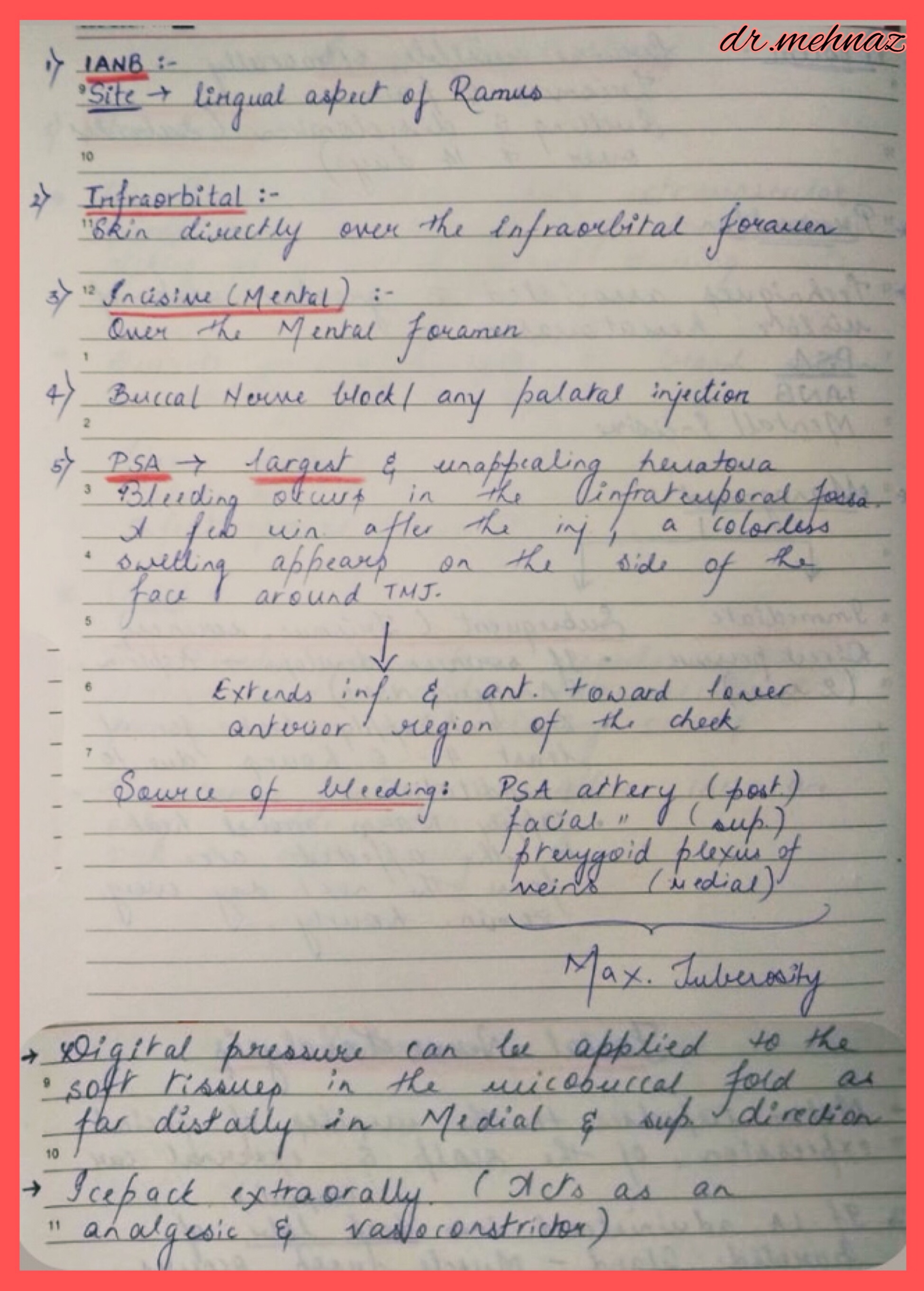
- Hematoma
- Pain on injection
- Burning on injection
- Infection
- Edema
- Sloughing of tissues
- Post-anesthetic intraoral lesions
🔷 Systemic Complications:
- Vasodepressor syncope
- Over dosage (toxic reaction)
- Allergy
- Psychogenic reactions
Clinical Tip💡
👉🏻Several preventive measures can be followed:📝
1) Select a local anesthetic with a duration of action that is appropriate for the length of the planned procedure.
2) Advise the patient and accompanying adult about the possibility of injury if the patient bites, sucks or chews on the lips, tongue and cheek. They should delay eating and avoid hot drinks until the effects of the anesthesia are totally dissipated.
3) Reinforce the warning with patient stickers and by placing a cotton roll or rolled up gauze (“Bite on the ghost”) in the mucobuccal fold if anesthesia symptoms persist.
4) The management of soft tissue trauma involves reassuring the patient and parent (it’s okay if the tissue turns white), allowing up to a week for the injury to heal, and lubricating the area with petroleum jelly or antibiotic ointment to prevent drying, cracking and pain.
References: Internet; Handbook of LA, 6e by Stanley F Malamed
Dr. Mehnaz Memon🖊