Specific biochemical signature (ex. phosphatidylserine “flips” to outer surface of plasma membrane)
Does not induce inflammation
Important in a Variety of Processes
Organism development
Cell number and organ size
Quality control during development
Removal of damaged cells
Cellular Changes
Cytoplasm condenses
Nucleus becomes misshapen
Chromatin condenses along the nuclear envelope
Cell eventually fragments into blebs
Phosphatidylserine on the blebs indicates to phagocytic cells that apoptosis is occurring
Phagocytic cells clear the cellular debris
Two Paths of Apoptosis
Extrinsic Pathway (using the Fas pathway as an example)
a) Trimeric Fas ligand on another cell binds to Fas death receptor b) Intracellular domain of Fas receptor recruits and activates FADD (Fas associated death domain) c) Activated FADD recruits initiator procaspases such as procaspase-8 or -10 (complex is referred to as death-inducing signaling complex or DISC) d) Complex formation activates the procaspases which then activate executioner caspases e) Executioner caspase activation leads to apoptosis
Intrinsic Pathway
a) Apoptotic stimulus activates BH3-only protein b) BH3-only protein blocks the activity of Bcl-2 protein c) Without Bcl-2 activity, BH123 proteins are able to oligomerize and cytochrome c is released from the intermembrane space of mitochondria d) Cytochrome c in the cytoplasm activates Apaf1 proteins which form a heptameric complex e) Apaf1 complex recruits initiator procaspase-9 f) Activated caspase-9 activates executioner caspase g) Executioner caspase activation leads to apoptosis
Bcl-2 Family of Proteins
Based on which specific domains are present in the protein
Anti-apoptotic Bcl-2 proteins (ex. Bcl-2 or Bcl-XL)
Separates cell from external environment; controls the flow of material into and out of it.
CYTOSOL
Aqueous solution that bathes organelles and contains a variety of molecules
Portion of cytoplasm not contained within organelles
Free ribosomes
ENDOMEMBRANE SYSTEM
Select group of membranous organelles that regulate protein trafficking and metabolism
NUCLEUS
Nuclear envelope with pores (double-membrane)
Site of DNA replication and RNA synthesis (transcription)
Contains: chromatin, nucleolus (rRNA and ribosomal proteins)
ENDOPLASMIC RETICULUM
Continuous with nuclear envelope
Cisternae enclose a space called the ER lumen
Rough ER: with bound ribosomes; site of protein synthesis, processing and secretion
Smooth ER: no ribosomes; lipid synthesis, carbohydrate metabolism, detoxification
TRANSPORT VESICLE
Keeps secretory proteins separate from proteins synthesized in the cytosol
GOLGI APPARATUS
cis side faces the nucleus, trans side where cargo exits
Modifies, stores and secretes molecules that it receives from the ER
Synthesizes its own macromolecules
LYSOSOME
Vesicle that contains hydrolytic enzymes; digests endosomal cargo
ENDOSOME
Forms when cell engulfs nutrients or other particles via endocytosis
RIBOSOMES
Two subunits: one large and one small
Synthesize proteins via translation
Can be bound to rough ER or free (suspended in cytosol)
MITOCHONDRION
Double-membrane bound: inner membrane invaginates to form cristae
Space within cristae: matrix (contains free ribosomes)
Space between inner and outer membranes: intermembrane space
Synthesizes ATP via citric acid cycle and oxidative phosphorylation (couples oxidation of nutrients with ADP phosphorylation)
PEROXISOME
Single-membrane bound vesicle
Produce hydrogen peroxide from detoxification of substances (i.e. alcohol)
CYTOSKELETON
Microfilaments, intermediate filaments and microtubules
Anchors organelles and provides structural framework
CENTROSOME
Where microtubules nucleate
Contains two small structure called centrioles
Functions in cell division
DOUBLE MEMBRANE BOUND ORGANELLES
Nucleus
Mitochondria
CLINICAL CORRELATIONS
Rough ER Network and Pancreatic beta cells – Specialize in synthesizing and secreting the peptide hormone insulin; large rough ER network proportional to their secretory activity
Smooth ER and Hepatic cells – Drugs and/or alcohol can induce the proliferation of smooth ER, which accelerates detoxification
Lysosomes and Tay-Sachs disease – Lysosomal storage disease that presents when lysosomes are missing a lipid-digesting enzyme (or its active form) – Lipids accumulate in cells because lysosomes cannot digest them; impair brain function
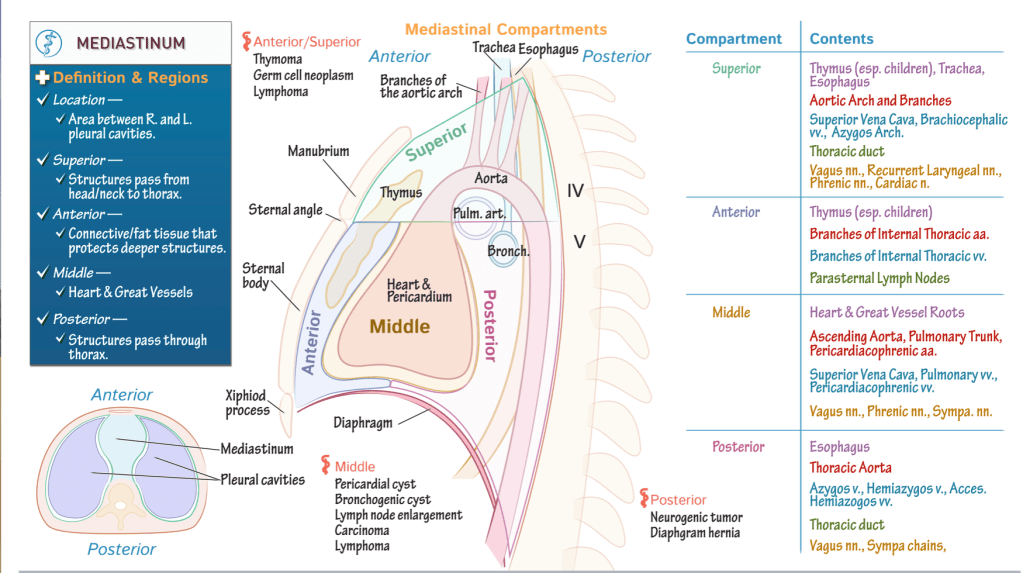
Middle compartment has a sac-like shape; it houses the pericardium, heart, and roots of the great vessels. Anterior compartment lies anterior to this, and extends from the sternal angle, superiorly, to the diaphragm, inferiorly. Posterior compartment lies posterior to the middle mediastinum, and, like the anterior mediastinum, extends from the sternal angle to the diaphragm. Superior mediastinum fills the space between the superior thoracic opening to the sternal angle.
Key anatomical structures
The thymus lies within the superior and anterior regions; recall that this structure regresses after childhood.
Then, return to where the root and ascending portion of the aorta arise in the middle mediastinum, and show that the aorta continues through the superior and posterior compartments. We’ve also shown the branches of the aortic arch as they extend through the superior mediastinum.
Next, posterior to the heart, show the opening of the left pulmonary artery as it passes to the left lung;
The opening of the left bronchus; indicate that the trachea extends through the superior and posterior compartments of the mediastinum.
The esophagus also passes through these compartments.
Pathology
Let’s indicate some key masses that can develop in the mediastinum; we’ll broadly categorize these by region of the mediastinum, but beware of overlap.
Anterior/superior mediastinum: thymoma, germ cell neoplasm, and lymphoma.
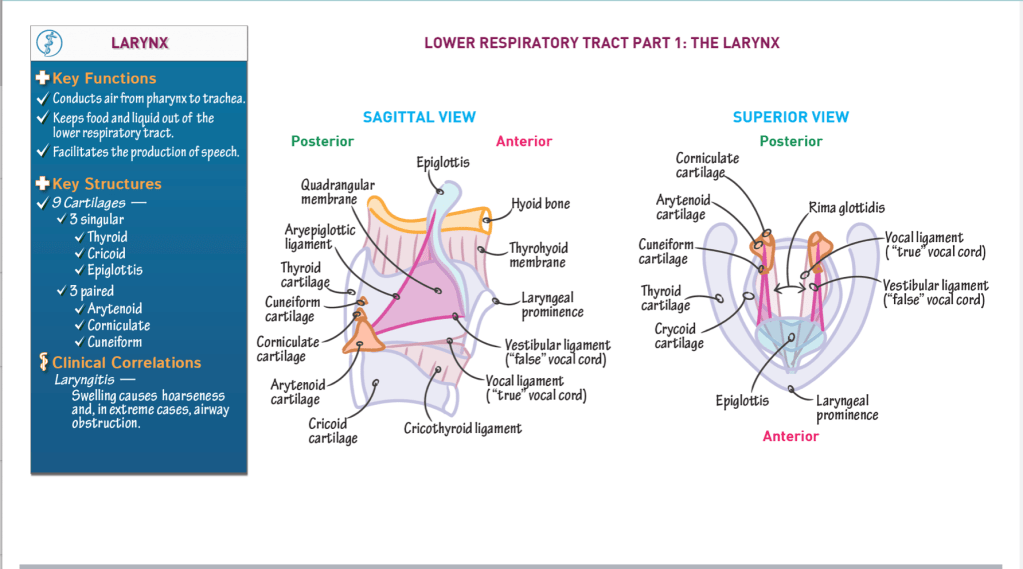
The larynx is the start of the lower respiratory tract.
Superiorly, the larynx is attached to the hyoid bone via connective tissues.
Three key functions of the larynx:
It conducts air from the pharynx to the trachea.
It prevents food and liquid from entering the lower respiratory tract.
It facilitates the production of speech.
Key anatomical structures:
Three larger, singular cartilages:
Thyroid cartilage – forms anterior and lateral walls; features the laryngeal prominence.
Cricoid cartilage – circular, forms base of larynx.
Epiglottis – “flap” that attaches to the internal surface of the thyroid cartilage, anteriorly, and projects posteriorly and superiorly over the opening of the larynx.
Upon swallowing, the flap closes off the entryway to the larynx, which prevents foods and liquids from entering the lower respiratory tract.
Three paired sets of smaller cartilages:
Arytenoid cartilage – articulates with cricoid cartilage posteriorly.
Corniculate cartilage – sits on arytenoid cartilages.
Cuneiform cartilage – sits anterior to corniculate cartilages; very small, wedge-shaped.
Membranes and connective tissues:
Thyrohyoid membrane – connects the thyroid cartilage and hyoid bone.
Cricothyroid ligament – extends superiorly from the cricoid cartilage to the thyroid and arytenoid cartilages.
Vocal ligament – thickened superior edge of the cricothyroid ligament comprises the vocal ligament; known as the “true” vocal cord because it facilitates sound production.
Rima glottides – opening between the vocal cords. During sound production, laryngeal muscles contract to rotate the arytenoid cartilages and alter the opening between the true vocal cords.
Quadrangular membrane – connects the lateral sides of the epiglottis to the arytenoid cartilages.
Free edges of the quadrangular membrane thicken to form the: Aryepiglottic ligament, superiorly The vestibular ligament, inferiorly
The vestibular ligament and its mucosal covering are often referred to as the “false vocal cord”; it does not participate in sound production.
Clinical correlations:
Laryngitis is inflammation of the vocal cords, which can stem from infectious or non-infectious causes (such as over-use). It typically results in hoarseness but severe swelling can block the airways.
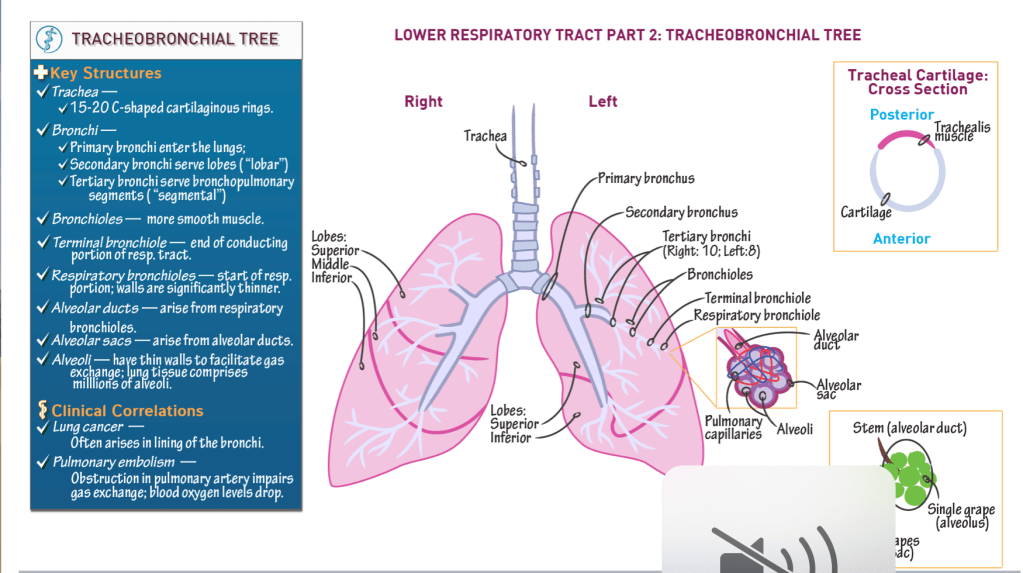
Comprises 15 – 20 C-shaped cartilaginous rings, are stacked vertically and connected via anular rings.
Trachealis posterior forms posterior wall of trachea; moves to accommodate foods passing posteriorly through the esophagus.
Bronchi:
Primary bronchi enter the lungs.
Secondary bronchi serve lobes of lung (“lobar” bronchi).
Tertiary bronchi serve bronchopulmonary segments (“segmental” bronchi); 10 on the right, 8-10 on the left.
Bronchioles:
Numerous, and narrow as they branch.
Have more smooth muscles in their walls, but still have cartilage in their walls.
Terminal bronchiole is the final passageway of the conduction portion of the respiratory system.
Respiratory bronchioles:
Demarcate the respiratory portion of the respiratory tract.
Thin walls allow some gas exchange.
Alveolar ducts:
Arise from respiratory bronchioles.
Alveolar sacs:
Terminal ends of the alveolar ducts.
Alveoli:
Thin-walled out-pockets of the alveolar sacs.
Surrounded by pulmonary capillaries.
Facilitate gas exchange between the respiratory and cardiovascular systems.
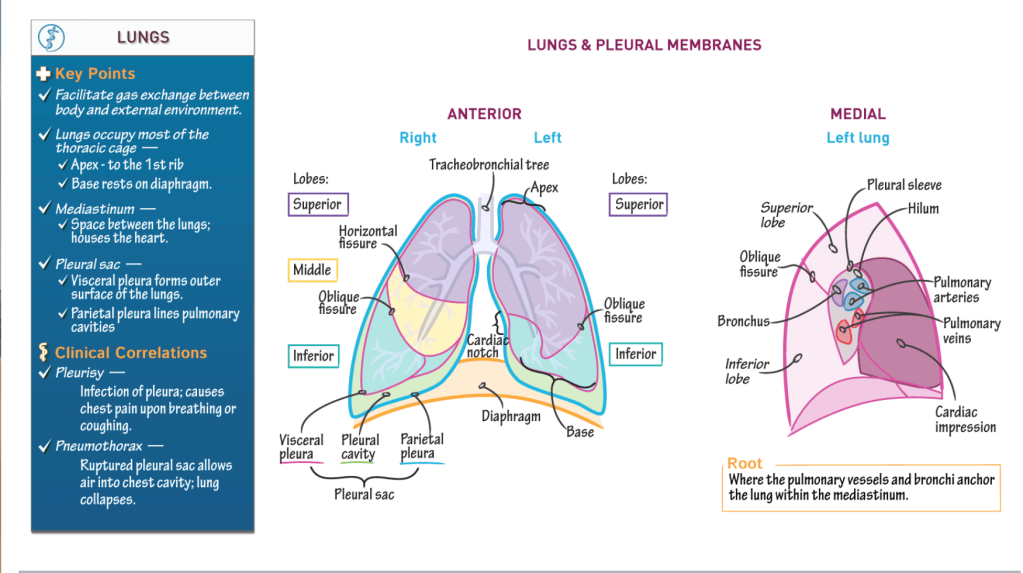
Lungs:
Hundreds of millions of alveoli.
Left lung = superior and inferior lobes; heart nestles into medial left lobe.
Right lung = superior, middle, and inferior lobes.
Clinical Correlations:
Lung cancer often originates in the bronchi. Pulmonary embolism (aka PE) obstructs arterial supply. In a PE, gas exchange is reduced, and blood oxygen levels drop.
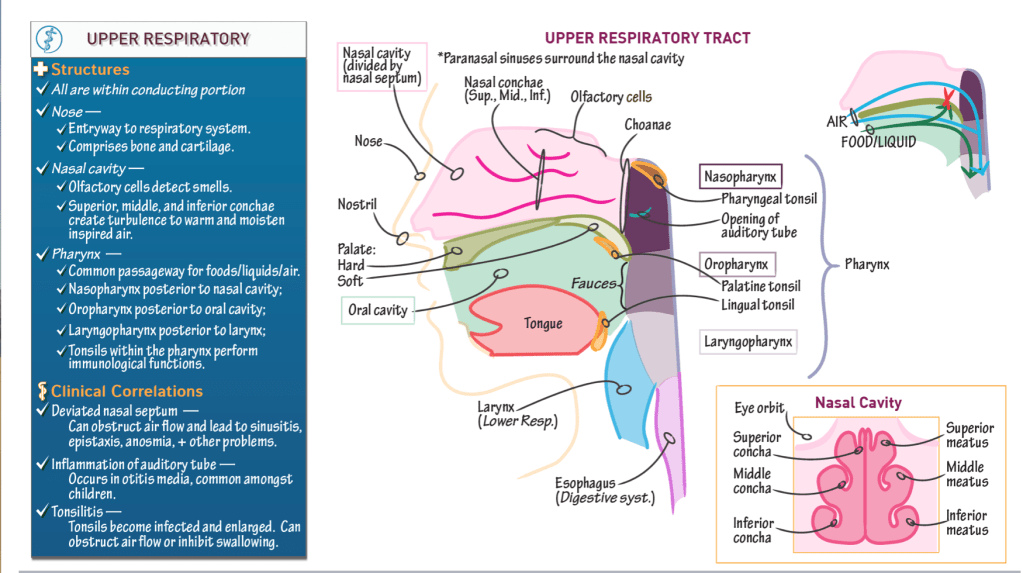
Opens the respiratory system to the external environment via the nostrils (aka, nares).
Comprises bone and cartilage.
Nasal cavity:
Posterior to the nose.
Separated from the oral cavity by the hard and soft palates:
The hard palate comprises the maxillary and palatine bones.
The soft palate comprises soft tissues.
Olfactory cells line the superior part of the nasal cavity
The nasal septum divides the cavity into right and left sides.
It comprises two vertical bony structures: the perpendicular plate of the ethmoid bone superiorly and the vomer, inferiorly.
A deviated nasal septum can obstruct airflow and cause sinusitis (sinus infection), epistaxis (nose bleeds), anosmia (inability to smell), and other health problems.
3 nasal conchae: superior, middle, and inferior.
Bony projections that arise on the lateral walls of the nasal cavity.
The nasal conchae create meatuses (superior, middle, and inferior), which are small tunnels.
Movement of air around the conchae and through the meatuses creates turbulence, which helps to warm and humidify the air. Hence, the conchae are sometimes referred to as the “turbinate” bones.
Paranasal sinuses
Spaces within the bones surrounding the nasal cavity.
Pharynx:
Descends posterior to the nasal cavity, oral cavity, and larynx, and is open to each of these structures.
Common passageway foods/liquid and air: it serves both the respiratory and digestive systems.
3 subdivisions:
Nasopharynx: posterior to the nasal cavity (and receives air from the nasal cavity). The choanae are the openings between the nasal cavity and the nasopharynx. Oropharynx: posterior to the oral cavity (and receives foods and liquids from the oral cavity). The fauces is the opening between the oral cavity and the oropharynx.
Laryngopharynx: posterior to the larynx (it is the final common passageway for air and food/liquid).
The auditory tube (aka, Eustachian or pharyngotympanic tubes) opens into the nasopharynx
Connects the ears and throat, which allows infection to pass between them.
Auditory tube inflammation occurs in otitis media (aka, ear infection), which is common amongst children.
Tonsils
Collections of lymphoid tissues that participate in immunological defense against bacterial and viral infections.
3 pairs of extrinsic tonsils:
Pharyngeal tonsils reside in the superior wall of the nasopharynx.
Palatine tonsils are near the palate (hence, their name).
Lingual tonsils are at the back of the tongue (“lingual” refers to the tongue).
As part of an aggressive immune response, the tonsils can swell and block airflow through the nose or inhibit swallowing.