The pterygoid response manifests in a sequential timeline beginning the moment a functional appliance is placed, with the full clinical response becoming evident within approximately 2 weeks, though some sources cite 6–8 weeks for it to be clearly obvious.
Timeline of Manifestation
The sequence unfolds in stages:
Immediately upon appliance placement — The neuromuscular balance is altered; lateral pterygoid muscle activity increases significantly right after insertion as the mandible is held in a protruded positionmeridian.allenpress+1
Within ~2 weeks — The mandible adapts to its new protruded position; retraction back to the original position becomes effortful and painful — this is the classic pterygoid response as described by Clark (1988) [pmc.ncbi.nlm.nih]
6–8 weeks — The successful clinical pterygoid response becomes clearly obvious and is used as a clinical checkpoint to confirm Twin Block therapy is working [pmc.ncbi.nlm.nih]
4–6 months — Lateral pterygoid muscle activity gradually decreases as neuromuscular adaptation stabilizes, preceding the longer-term skeletal and condylar morphological changesjdat+1
Mechanism Behind It
When the mandible postures downward and forward (as directed by the Twin Block inclined planes), a tension zone forms above and behind the condyle. This area is rapidly invaded by proliferating blood vessels and connective tissue. A new pattern of muscle behavior is established, making it difficult — and ultimately painful — for the patient to retract the mandible to its former retruded position. McNamara and Petrovic (1980) attributed this to altered muscular activity of the lateral pterygoid and retractor muscles, followed by condylar adaptation. [journalijar]
Clinical Significance
The pterygoid response serves as a key clinical indicator that the Twin Block appliance is functioning correctly. If a patient can still comfortably retract their mandible after 6–8 weeks, it suggests the bite registration may not have adequately engaged the functional inclined planes or the appliance wear compliance is poor. [pmc.ncbi.nlm.nih]
Reference: Clark WJ. The twin block technique. A functional orthopedic appliance system. Am J Orthod Dentofacial Orthop. 1988 Jan;93(1):1–18.
🎬 WHY THIS PAPER EXISTS (The “So What” in 30 Seconds)
Orthodontics always taught: “Functional crossbite = symmetric mandible, just positioned wrong. Fix the maxilla, mandible self-corrects.” Clean. Simple. Reassuring.
Santos Pinto said: Not so fast.
In growing children, a mandible that’s been displaced for months to years actually remodels and becomes structurally asymmetric — especially at the ramus. This paper is the first to prove both morphological AND positional asymmetry exist simultaneously, and that early RPE can reverse both.
🔴 Examiner hook: “Functional crossbite means symmetric mandible.” — TRUE for adults, NOT fully true for growing children. This paper is your evidence.
LAYER 1 — POSITIONAL (Where is the mandible sitting?)
→ Whole mandible shifted LATERALLY + POSTERIORLY to crossbite side
→ Midline deviation = 1.6 mm toward crossbite side
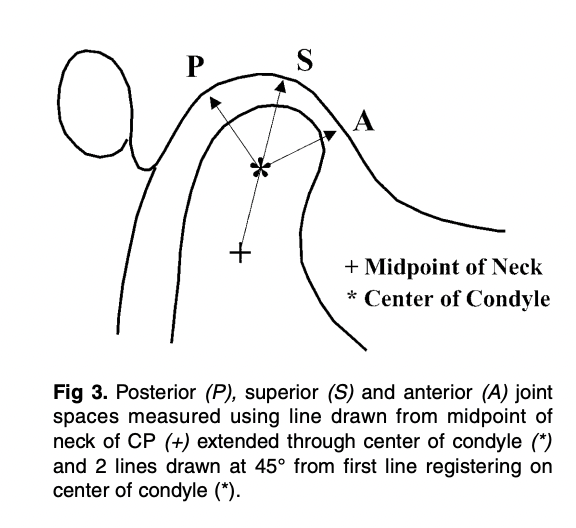
LAYER 2 — JOINT SPACE (Where is the condyle in the fossa?)
→ Noncrossbite condyle = more anterior on articular eminence
→ Superior joint space: 4.0 mm (non-XB) vs 3.2 mm (XB) ← SIGNIFICANT
→ Posterior: larger on non-XB (not significant)
→ Anterior: EQUAL on both sides ← MCQ TRAP
LAYER 3 — MORPHOLOGICAL (Has the bone actually changed shape?)
→ Yes! Ramus is SHORTER on crossbite side
→ Co–Sy: 75.5 mm (non-XB) vs 73.9 mm (XB) — 1.6 mm difference
→ Asymmetry in RAMUS (condyle + coronoid) but NOT in body (L6–L1 equal)
⚡ THE NUMBERS BANK — Memorise These 10 Numbers
Value
What It Represents
5.9–9.4%
Incidence of UPXB
67–79%
Proportion of UPXB that are functional
1.6 mm
Midline deviation + Co–Sy difference
~3 mm
L6 and coronoid horizontal offset (crossbite side more lateral)
4.0 vs 3.2 mm
Superior joint space (non-XB vs XB) — only SIGNIFICANT TMJ finding
8.8 yrs
Mean age of subjects
15
Sample size
1 month
RPE activation phase
6 months
Retention phase
11
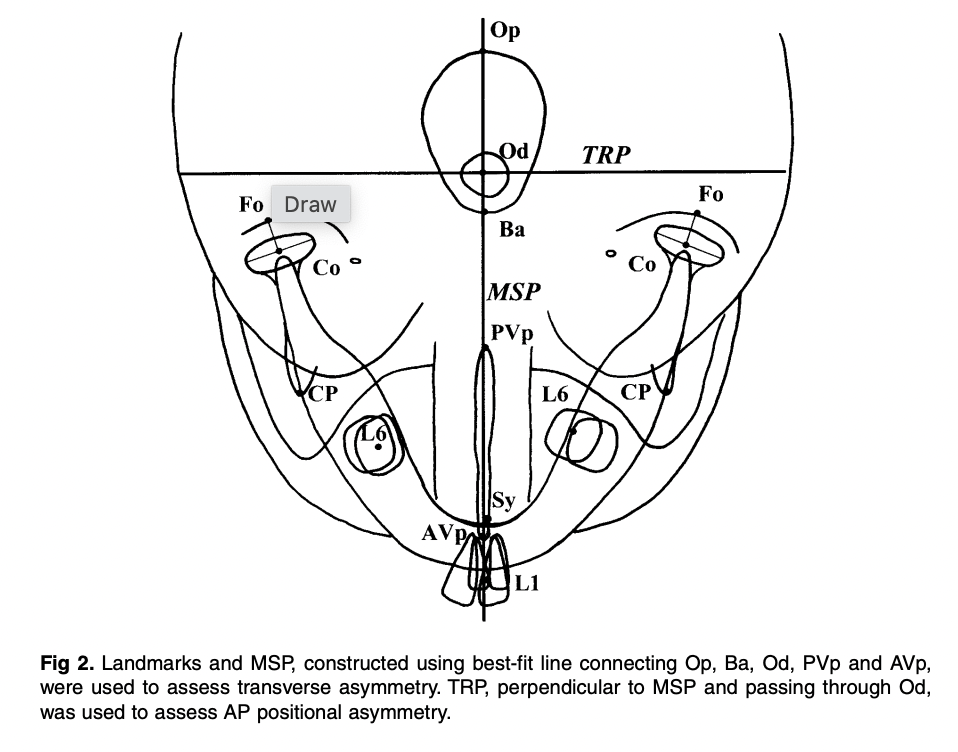
Total SMV landmarks digitized
🔥 MECHANISM CHAIN — Viva Storytelling Version
Examiner: “Walk me through how FUPXB causes skeletal asymmetry.”
YOUR ANSWER:
Narrow maxilla creates a dental interference → mandible must shift from CR to ICP, deviating laterally and anteroposteriorly toward the crossbite side → this asymmetric posture alters condylar loading: noncrossbite condyle rides higher on the articular eminence → muscle compensation: anterior temporalis fires more on the noncrossbite side; posterior temporalis fires more on the crossbite side → sustained asymmetric forces trigger adaptive bone remodeling → the ramus on the crossbite side becomes shorter (both condylar and coronoid processes affected) → result: a functionally crossbited child now has a morphologically asymmetric mandible
🎯 EXAMINER TRAPS — Don’t Fall For These
Trap Statement
The Truth
“All joint spaces are asymmetric in FUPXB”
❌ Only superior space is significant; anterior joint spaces are EQUAL
“RPE doesn’t affect morphological asymmetry”
❌ RPE + retention eliminated morphological asymmetry — crossbite side grew MORE
“The mandibular body is asymmetric”
❌ L6–L1 distance is EQUAL — asymmetry is in the ramus only
“Glenoid fossa is asymmetric too”
❌ Fossa position showed little/no transverse or AP asymmetry
“Chewing patterns normalize after RPE”
❌ Reverse chewing sequencing persists even after correction
“Functional crossbite = symmetric mandible”
⚠️ Only in adults — in growing children, morphological change occurs
🧠 MUSCLE MNEMONIC — Never Mix This Up
“At the PARTY, Non-Cross goes FORWARD, Cross goes BACK”
ANTERIOR temporalis (forward-pulling) → fires more on NON-crossbite side
POSTERIOR temporalis (backward-pulling) → fires more on CROSSBITE side
📊 Pre vs. Post Treatment — What Changed?
Measurement
Pre-Treatment
Post-Retention
Verdict
Co–Sy side difference
Significant
Not significant
✅ Resolved
L6 lateral offset
~3 mm
~0 mm
✅ Resolved
Midline deviation (L1)
1.6 mm
Not significant
✅ Resolved
Superior joint space gap
Significant
Not significant
✅ Resolved
Glenoid fossa position
Not significant
Not significant
➡️ Unchanged (already symmetric)
Chewing pattern (reverse)
Abnormal
Still abnormal
❌ NOT resolved
🔑 Key insight on growth: Crossbite-side ramus grew MORE than noncrossbite side during treatment — compensatory catch-up growth. The mandible also rotated forward and medially on the crossbite side, and backward and laterally on the noncrossbite side.
🏛️ LANDMARKS MNEMONIC (All 11 SMV Landmarks)
“Old Baboons Often Play Violins — Conducting Fine Concerts, Like Symphony”
❓ SELF-TEST — Rapid Fire (Cover answers, test yourself)
Question
Answer
Which ramus is LONGER in FUPXB?
Noncrossbite side
Which joint space is EQUAL on both sides?
Anterior
Which is the ONLY significantly different joint space?
Superior
Where does the asymmetry occur in the mandible?
Ramus (not body)
What persists even after successful RPE?
Reverse chewing sequencing
What muscle is more active on the noncrossbite side?
Anterior temporalis
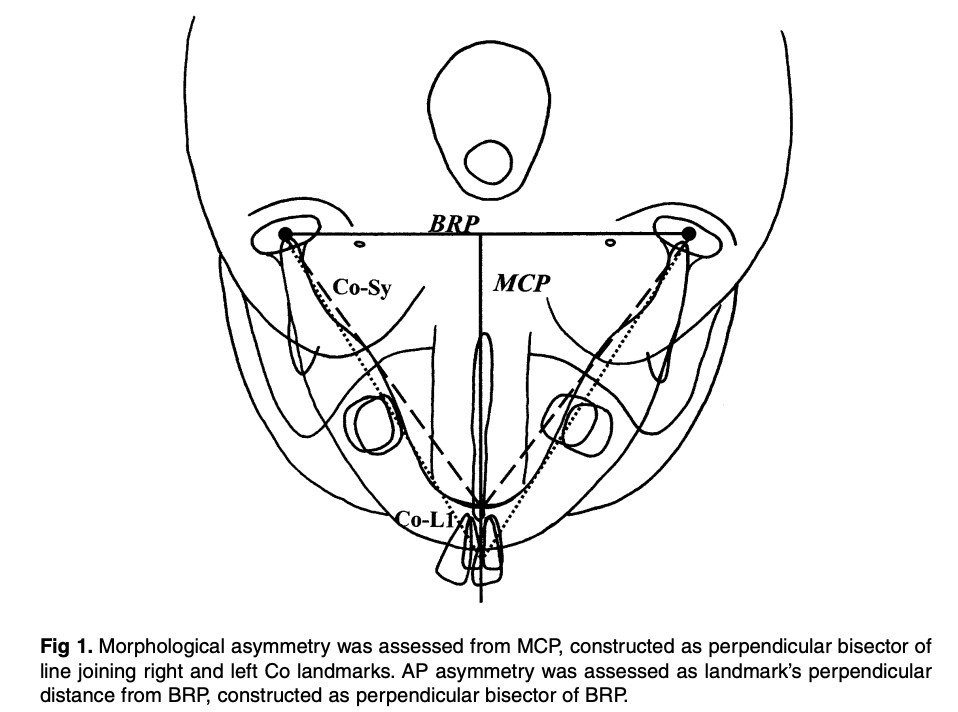
What does the MCP stand for and how is it constructed?
Midcondylar reference plane — ⊥ bisector of Co-Co line
What was the midline deviation pre-treatment?
1.6 mm toward crossbite side
Which radiograph assessed TMJ spaces?
Zonograms (4-turn spiral tomography)
What is the key conclusion that overturns classic teaching?
Functional crossbites cause morphological (structural) mandibular asymmetry in growing children
🩺 VIVA CLINCHER — The One Paragraph Examiners Love
“Santos Pinto et al. demonstrated that the classic view of functional crossbite as purely a positional problem is incomplete in growing children. Their prospective study showed the mandible is both positionally displaced and morphologically asymmetric — with the ramus shorter on the crossbite side due to adaptive remodeling. Crucially, the asymmetry is ramus-specific; the mandibular body remains symmetric. Early bonded RPE successfully resolved both layers of asymmetry through compensatory growth, though abnormal chewing patterns persisted, highlighting the need for functional rehabilitation post-treatment.”
Picture this exam scenario: A 7-year-old child sits in your chair. Her mom says “her jaw looks crooked.” You notice her teeth bite on the right side but her chin shifts left. Is this dental? Skeletal? Functional? Do you treat now or wait?
Every answer in this review solves THAT case.
⚡ The “Know This Or Fail” Numbers
Stat
Value
Why It Matters
Posterior crossbite prevalence
7–23%
Most common transverse malocclusion
FXB = unilateral with shift
80–97% of all PXB
Nearly all UPXBs are functional!
Self-correction rate
0–9%
Never justify waiting
Deciduous dentition prevalence
8.4% → 7.2% mixed
Slight spontaneous decrease
Spontaneous new crossbite development
7%
Equals self-correction rate — net zero
Equilibration success (< 5 yrs)
27–64%
Only in very young, limited use
Arch perimeter gain
4 mm (85% stable long-term)
Bonus benefit of expansion
🔥 EXAM TRAP: “Posterior crossbite is self-correcting” → FALSE. Only 0–9%. Never a valid clinical justification.
🧩 Etiology: The BIG Picture First
Think in 3 layers — Genetic → Environmental → Habit
NARROWED MAXILLA ↑ ┌─────────────────────────────────┐ │ SKELETAL: Small Max/Mand ratio │ ← Genetic + mouth breathing │ + Increased lower face height │ └─────────────────────────────────┘ ↑ ┌───────────────────────────────────────┐ │ AIRWAY: Adenoids / Tonsils / Rhinitis│ → Mouth breathing → narrow maxilla │ + Neonatal intubation │ → Direct palatal deformation └───────────────────────────────────────┘ ↑ ┌─────────────────────────────────────────────┐ │ HABIT: Pacifier / Digit sucking >4 yrs age │ → ↓ Max intercanine + ↑ Mand intercanine └─────────────────────────────────────────────┘
🧠 Mnemonic: “GANH”(say it like “Gain” — because early treatment = gain!)
🔍 Differential Diagnosis — The Most Examined Section
The 3-Type Framework
Feature
✅ FXB (Functional)
Single Tooth XB
True Skeletal Bilateral XB
CO vs CR
Discrepancy (mandatory finding)
Coincident
Coincident
Mandibular midline
Deviated to crossbite side
Midline OK
Midline OK
Maxillary arch shape
Symmetrical (key!)
Asymmetrical
Symmetrical
Crowding pattern
More in maxilla (not mandible)
Localized
—-
Crossbite side molar
Class II (partial/full)
Varies
Bilateral Class II
Non-crossbite side molar
Class I
Normal
Bilateral Class II
Condyle position (tomogram)
Non-XB side: down & forward in fossa
Symmetric
Symmetric
Cause
Transverse maxillary deficiency
Overretained teeth / arch length
Severe skeletal discrepancy
🧠 Mnemonic: “SMACK-D” (What FXB gives you clinically)
Shift of mandible → toward crossbite side Midline mandibular deviation → toward crossbite side Arch — maxillary is symmetrical (despite appearing unilateral!) CO–CR discrepancy — the defining diagnostic feature Klass II on crossbite side / Class I on non-crossbite side (K for klass 😄) Deficiency maxillary arch → more crowding in upper than lower
🔥 EXAM TRAP: The maxillary arch in FXB is SYMMETRICAL. The unilateral appearance is caused by the mandibular shift — not by asymmetric maxillary constriction. Examiners love asking this!
⏰ Treatment Timing — The Golden Window
Think of the Midpalatal Suture as a WINDOW that closes with age:
Age: 2–5 yrs 6–8 yrs 9–11 yrs 12+ yrs Adult Suture: Wide open [BEST WINDOW] Narrowing Almost fused Fused Force: Minimal Small forces Moderate RME needed SURGERY Recommend: Equilibration ✅ IDEAL ⚠️ Difficult ⚠️ RME only ❌ Ortho+Surg
Late deciduous / early mixed dentition = IDEAL → small forces open suture, permanent incisors get space before eruption
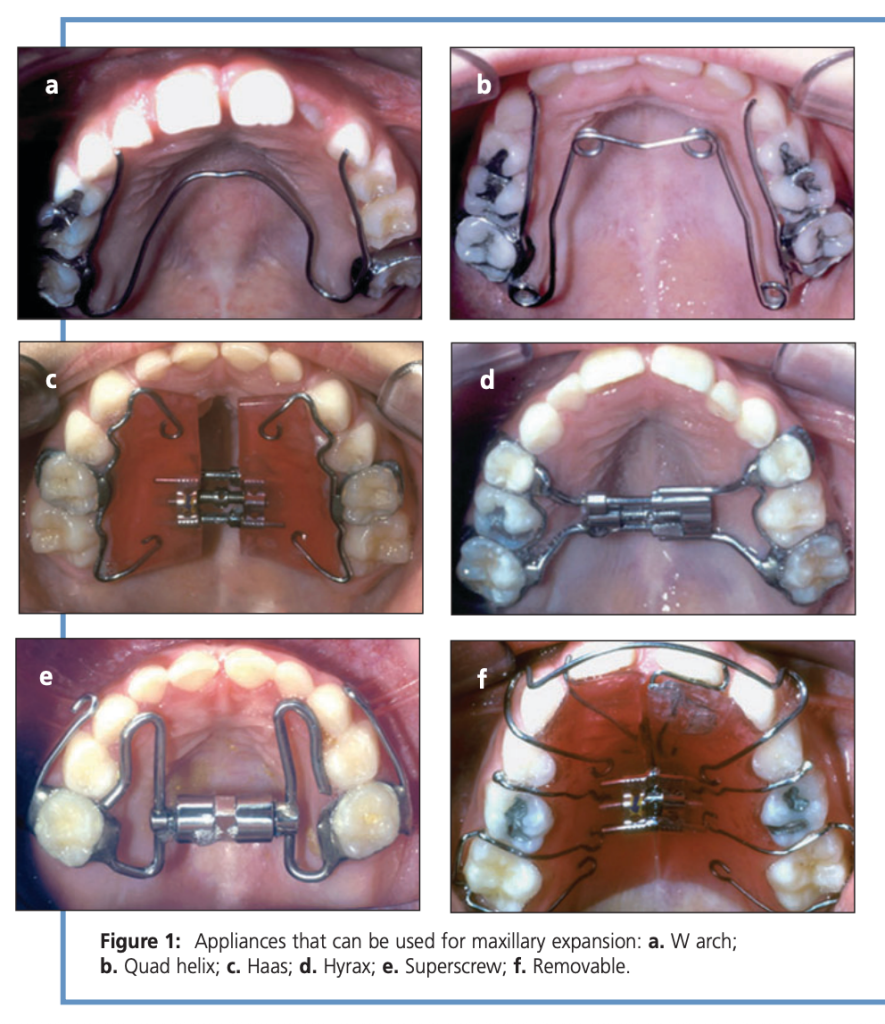
🏆 Gold standard — 1/3 cost of removable, 1/5 treatment time
W-Arch
Slow
¼ turn / 2–3 days
6–12 wks
✅ Good alternative
Haas
RME
1–2 × ¼ turn/day
2–6 wks
✅ Tissue-borne, most skeletal effect
Hyrax
RME
1–2 × ¼ turn/day
2–6 wks
✅ Tooth-borne, hygienic
Superscrew
RME
1–2 × ¼ turn/day
2–6 wks
✅ Comparable to Haas/Hyrax
Removable plate
Slow
¼ turn / 5–7 days
Longest
❌ NOT recommended — compliance failure, relapse, lost appliances
📋 Retention Protocol — “SOLAR”
Stabilize screw with ligature wire or composite Overexpand — lingual cusps of upper contact buccal cusps of lower Leave appliance in place for retention OR make removable retainer At least 4–6 months retention minimum Rule: Retention period ≥ active treatment duration
⚠️ Side Effects of RME — “DEMO”
Diastema (midline maxillary — transient! closes via transeptal fibers) → warn patient/parent Expansion of mandibular intercanine width (spontaneous — actually a bonus in crowded cases) Maxillary protraction (forward movement of maxilla — useful in Class III patients!) Open bite (anterior) — especially if 2nd permanent molars present; control molar eruption carefully
🧬 The Adaptation Argument (Why You MUST Treat Early)
This is the biological rationale section — examiners love conceptual questions here.
If left untreated, 3 irreversible adaptations occur:
Condylar asymmetry → glenoid fossa and condyle remodel asymmetrically during growth
Mandibular rotation → mandible rotates relative to cranial base (submentovertex X-ray shows this in adults)
Muscle adaptation → masticatory cycle becomes asymmetric (Throckmorton et al.)
After early treatment: condyle symmetry restored, mandibular rotation corrected, masticatory symmetry re-established
Adult with untreated FXB: mandible is rotated relative to cranial base but symmetric within the fossa — adaptation has already “locked in” the asymmetry
🔥 EXAM TRAP: In adults with untreated posterior crossbite, condyles ARE symmetric within the fossa (adaptation is complete) but mandible IS asymmetric relative to the cranial base. Don’t confuse this!
AGAINST causation: Sari et al., Keeling et al. found no causal link
Safe conclusion:“Crossbite may be a cofactor in TMD identification, but its role should not be overstated”
🎯 The Selective Grinding Rule (< 5 Years Only)
Age limit: strictly < 5 years
Success rate: 27–64% (Lindner: 50% in 4-year-olds)
The magic number: maxillary intercanine width must be ≥ 3.3 mm greater than mandibular for best results
Beyond age 5 → expansion appliances required, not grinding
🏁 Master Flash Summary — “FEED-SOLAR”
(Treatment protocol in one phrase)
Functional shift eliminated by symmetric maxillary expansion Early treatment — late deciduous / early mixed dentition Expand symmetrically (even for unilateral presentation!) Don’t use removable appliances — Stabilize screw, Overexpand, Leave appliance in, At least 4–6 months, Retention ≥ treatment time
🔥 5 Rapid-Fire Viva Questions
Q1. Why do we expand the maxilla symmetrically for a unilateral crossbite? → Because the maxilla is bilaterally constricted; the unilateral appearance is due to the mandibular shift
Q2. What is the single most important diagnostic feature of FXB? → CO–CR discrepancy (centric occlusion ≠ centric relation)
Q3. Why is the Quad Helix preferred over removable plates? → 1/3 cost, 1/5 treatment time, no compliance issues
Q4. What happens to the midpalatal diastema created during RME? → Closes spontaneously via transeptal fiber pull and dental tipping
Q5. Name two studies supporting crossbite–TMD correlation. → Alamoudi (2000) and Egermark-Eriksson et al. (1990)
The angulation of the Twin Block appliance’s inclined planes underwent three distinct stages of development, each driven by clinical observations and biomechanical reasoning.
Stage 1 — 90° (Initial Design)
The earliest Twin Block appliances, developed by W.J. Clark, featured bite blocks angulated at 90° to the occlusal plane. Patients were required to consciously posture the mandible forward to occlude the blocks. However, many patients struggled to maintain this forward position and habitually returned to their original distal occlusal position, causing the flat-surfaced blocks to stack on top of each other. This resulted in a significant posterior open bite, a complication seen in approximately 30% of early Twin Block cases.
Stage 2 — 45° (Functional Correction)
To resolve the compliance problem, the angulation was modified to 45° to the occlusal plane. This immediately guided the mandible forward more passively, eliminating the stacking issue. A 45° angle provides an equal downward and forward force component to the lower dentition, promoting both vertical and sagittal growth stimuli. Clark continued using this angulation clinically for approximately 8 years before the next modification.
Stage 3 — 70° (Current Standard)
After the prolonged use of the 45° design, the angulation was increased to 70° to the occlusal plane — the current standard configuration. This steeper angle introduces a more horizontal force component, theoretically encouraging greater forward (sagittal) mandibular growth rather than a combined downward-forward stimulus. The 70° angle is now incorporated into the standard Twin Block design with maxillary and mandibular acrylic base plates.
Angulation at a Glance
Angulation
Rationale
Limitation
Angulation
Rationale
Limitation
90°
Original design; edge-to-edge block contact
~30% posterior open bite; poor compliance
45°
Equal forward + downward force vector
Used for 8 years; less horizontal growth stimulus
70°
More horizontal force; greater forward mandibular growth
May reduce mandibular postural guidance
Clinically, if a patient struggles to maintain the forward mandibular posture with a 70° design, it is advisable to revert to a 45° angulation to facilitate easier maintenance of the protruded position.
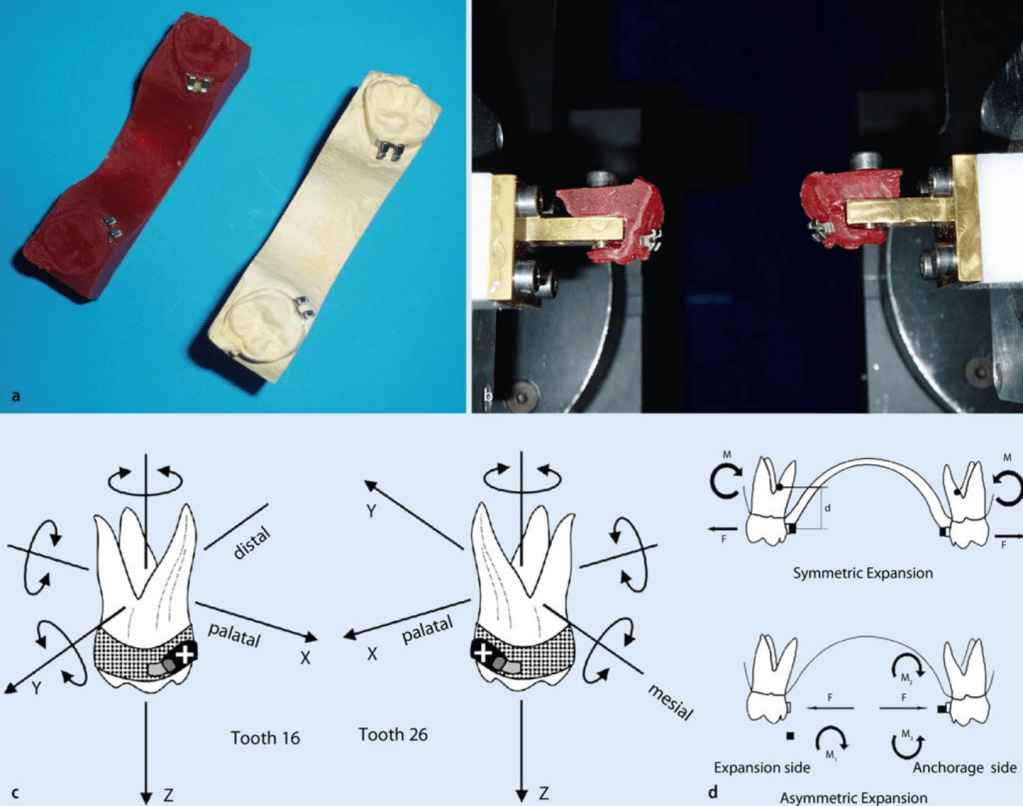
Posterior crossbite is one of the most common transverse discrepancies encountered in orthodontic practice. A transpalatal arch (TPA) is a deceptively simple appliance — but when activated using Burstone biomechanics, it becomes a powerful tool capable of producing controlled symmetric or asymmetric molar expansion.
Understanding force systems, moment-to-force ratios, and side effects is essential if one wants to use this appliance predictably.
This article walks through the biomechanics, clinical application, and outcomes of a Burstone-type TMA transpalatal arch.
1. Why Molar Transverse Position Matters
Correct positioning of maxillary first molars is critical for:
Functional occlusion
Arch coordination
Midline stability
TMJ health
Untreated transverse maxillary deficiency may cause:
Posterior crossbite
Functional mandibular shift
Midline deviation
TMJ strain
Posterior crossbite prevalence:
Unilateral: ~9%
Bilateral: ~4%
Quick Viva Pause
Q: Why is unilateral crossbite more problematic than bilateral crossbite?
A: Because it frequently causes functional mandibular shift, leading to asymmetry and midline deviation.
2. What is a Burstone-Type Transpalatal Arch?
A transpalatal arch (TPA) connects the maxillary first molars across the palate.
It can be used in two modes:
Mode
Purpose
Passive
Anchorage reinforcement / stabilization
Active
Tooth movement
The Burstone system differs from traditional TPA systems.
Key Differences
Feature
Burstone TPA
Goshgarian TPA
Attachment
Lingual bracket
Lingual sheath
Wire material
TMA
Stainless steel
Force magnitude
Lower
Higher
Control
High precision
Less controlled
TMA wires produce ~60% lower force compared to stainless steel, improving control and reducing unwanted side effects.
Viva Pause
Q: Why is TMA preferred over stainless steel in Burstone TPA?
Answer
Lower load-deflection rate
Greater formability
More controlled force delivery
Reduced risk of excessive tipping
3. Recommended Activation
Typical parameters reported:
Parameter
Value
Activation
3–10 mm
Expansive force
1.5–4 N
Wire dimension
0.032 × 0.032 TMA
A 10 mm activation produces approximately 4 N expansion force.
However, force depends on:
Wire length
Loop configuration
Height of arch
Patient anatomy
Viva Pause
Q: What happens if the TPA height increases?
Answer
The moment-to-force ratio changes, altering the type of tooth movement.
4. Types of Expansion Using TPA
1. Symmetric Expansion
Both molars move buccally.
Used for:
Bilateral posterior crossbite
Narrow maxilla
2. Asymmetric Expansion
One side expands more than the other.
Used for:
Unilateral crossbite
This is achieved by creating moment differential between molars.
Biomechanical Principle
Side
Force System
Crossbite side
Force → tipping movement
Anchorage side
Force + counter-torque
This allows unilateral expansion without significant movement of the anchorage molar.
Viva Pause
Q: Why is tipping used on the crossbite side?
Answer
Because tipping requires less force than bodily movement, making unilateral correction easier.
5. Biomechanics of Burstone TPA
The appliance generates:
Force component
Effect
Expansive force
Buccal movement
Moment
Crown tipping
Vertical force
Minor extrusion/intrusion
The center of resistance of molars lies approximately:
7 mm apical to the bracket level in the furcation region.
Viva Pause
Q: Why does TPA cause buccal crown tipping?
Answer
Because the force is applied away from the center of resistance, creating a moment that tips the crown buccally.
6. Clinical Outcomes (Study Findings)
Symmetric Expansion
Parameter
Result
Mean expansion
~4.5 mm
Buccal tipping
~10°
Treatment time
12 weeks
Vertical side effects
Minimal
Expansion occurred primarily due to buccally directed forces acting at the crown level.
Viva Pause
Q: What is the main disadvantage of symmetric TPA expansion?
Answer
Buccal crown tipping of molars, which may require later torque correction.
7. Asymmetric Expansion Outcomes
For unilateral crossbite:
Parameter
Crossbite Side
Anchorage Side
Tooth movement
~2.5 mm
~0.8 mm
Torque
Higher
Lower
Vertical movement
Minimal
Minimal
Thus effective unilateral expansion was achieved in all patients.
Viva Pause
Q: Why does the anchorage side show less movement?
Answer
Because counter-torque increases moment-to-force ratio, resisting tipping.
8. Side Effects
Vertical Effects
Movement
Magnitude
Intrusion
~0.6 mm
Extrusion
~0.8 mm
These are considered clinically insignificant.
Sagittal Effects
Minor:
Mesial rotation of molars
Minimal sagittal displacement
Viva Pause
Q: What is the most common rotational side effect?
Answer
Mesial rotation of molars
9. Why Simulation Systems Were Used
The study used Orthodontic Measurement and Simulation System (OMSS).
Purpose:
Measure force systems
Predict tooth movement
Compare simulation vs clinical outcomes
Findings:
Simulated movements were highly consistent with clinical results.
Viva Pause
Q: Why can’t simulation fully replicate real orthodontic tooth movement?
Answer
Because it cannot account for:
Mastication
Occlusal contacts
Soft tissue forces
Material fatigue
Biological variability
10. Clinical Pearls for Orthodontists
1. TPA is not just an anchorage appliance
It can produce controlled molar movement.
2. Shape matters
Force depends on:
Height
Length
Configuration
3. Perfect force systems are difficult
Even identical activation may produce different forces due to anatomical variation.
4. Tipping is expected
Crossbite correction usually occurs by molar tipping rather than bodily movement.
5. Torque correction may be needed later
After expansion, clinicians may need to:
Add counter-torque
Use archwire adjustments
Rapid Revision Table
Feature
Symmetric Expansion
Asymmetric Expansion
Indication
Bilateral crossbite
Unilateral crossbite
Force system
Equal bilateral forces
Differential moment
Mean expansion
~4.5 mm
~2.5 mm on affected side
Crown tipping
Present
Controlled
Side effects
Minimal
Minimal
Ultimate Viva Questions (PG Level)
Basic
1. What is the function of a transpalatal arch?
Anchorage control
Molar rotation control
Transverse expansion
Intermediate
2. Why is TMA preferred in Burstone TPA?
Lower load-deflection rate
Better formability
More controlled forces
Advanced
3. How does asymmetric TPA correct unilateral crossbite?
By generating different moment-to-force ratios on each molar.
Clinical
4. What is the most common side effect of TPA expansion?
Buccal crown tipping.
Biomechanics
5. Why does tipping occur with TPA?
Force acts away from center of resistance, generating a moment.
Final Takeaway
The Burstone-type TPA is a biomechanically sophisticated appliance capable of producing:
Controlled symmetric molar expansion
Targeted asymmetric correction of unilateral crossbite
Minimal side effects
When understood biomechanically, it transforms from a simple wire into a precise orthodontic force delivery system.
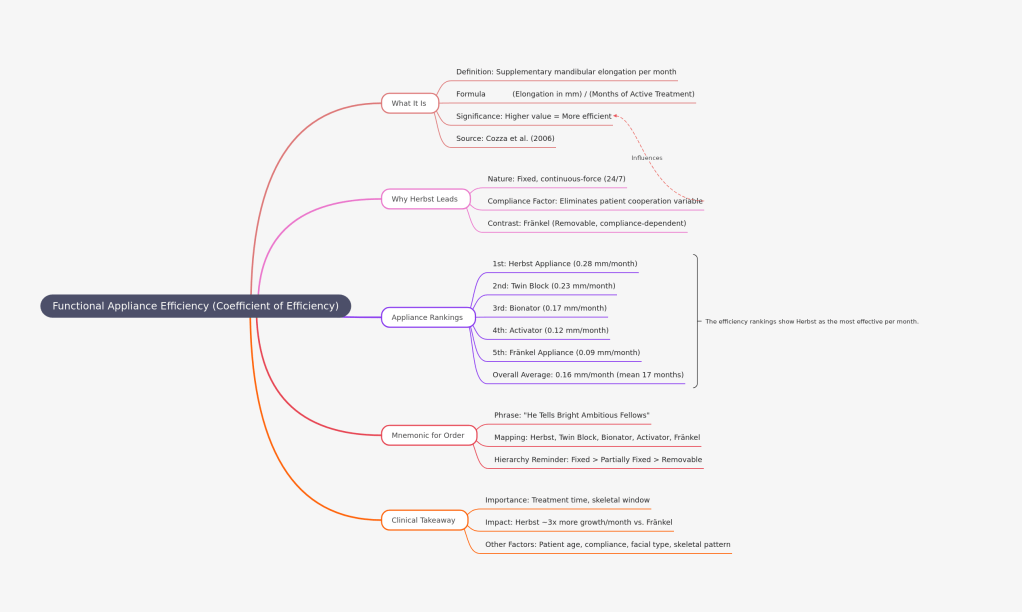
If you’ve ever wondered why one functional appliance seems to “work better” than another — or why your supervisor prefers the Herbst over the Activator — the answer might lie in a single, elegant metric: the coefficient of efficiency.
What Is the Coefficient of Efficiency?
Imagine two appliances, both claiming to stimulate mandibular growth. One achieves 6 mm of supplementary elongation in 12 months. Another achieves the same 6 mm, but takes 24 months. Are they equally effective? Technically yes — but practically, no.
This is exactly the problem that Cozza, Baccetti, Franchi, De Toffol, and McNamara Jr. sought to address in their landmark 2006 systematic review published in the American Journal of Orthodontics and Dentofacial Orthopedics. They proposed a simple but powerful formula:
Coefficient of Efficiency=Months of active treatmentSupplementary mandibular elongation (mm)
In plain terms — how many millimetres of extra jaw growth does the appliance produce per month of wear? The higher the number, the more efficient the appliance.
The Rankings: Who Wins?
Cozza et al. analyzed 22 studies (4 RCTs + 18 CCTs) spanning literature from 1966 to 2005. Here’s how the five major functional appliances stacked up:
Rank
Appliance
Coefficient of Efficiency
🥇 1st
Herbst Appliance
0.28 mm/month
🥈 2nd
Twin Block
0.23 mm/month
🥉 3rd
Bionator
0.17 mm/month
4th
Activator
0.12 mm/month
5th
Fränkel Appliance
0.09 mm/month
The overall average across all appliances was 0.16 mm/month, with a mean active treatment duration of approximately 17 months.
Why Does the Herbst Appliance Lead?
The Herbst appliance is a fixed, continuous-force device — it works 24/7, regardless of patient cooperation. This relentless, round-the-clock mandibular advancement is the primary reason it tops the efficiency chart at 0.28 mm/month.
In contrast, the Fränkel appliance sits at the bottom (0.09 mm/month) — not because it’s biologically inferior, but because it is a tissue-borne, removable appliance heavily dependent on patient compliance. Worn only part of the day, its per-month output naturally dilutes.
The lesson? Compliance is a hidden variable in efficiency. Fixed appliances eliminate this variable; removable ones are at its mercy.
Think: “He Tells Bright Ambitious Fellows” — going from the most efficient to the least.
Or simply associate the appliance type with compliance demand:
Fixed (Herbst) = Highest efficiency
Partially fixed (Twin Block) = Second
Removable (Bionator, Activator, Fränkel) = Lower, in descending order
The Clinical Takeaway
For busy orthodontic practices where treatment time matters — especially in growing patients with a closing window of skeletal opportunity — choosing a more efficient appliance can make a meaningful difference. A patient treated for 18 months with a Herbst gains the equivalent of roughly 3× more supplementary mandibular growth per month compared to a Fränkel wearer.
That said, efficiency isn’t everything. Patient age, compliance, facial type, and skeletal pattern all factor into appliance selection. But the next time someone asks “which functional appliance works best?” — you now have the data to give a precise, evidence-based answer.
Reference: Cozza P, Baccetti T, Franchi L, De Toffol L, McNamara JA Jr. Mandibular changes produced by functional appliances in Class II malocclusion: a systematic review. Am J Orthod Dentofacial Orthop. 2006 May;129(5):599.e1-12. PMID: 16679196.
In orthodontics, one of the greatest clinical advantages you can develop is predictability. The ability to anticipate how a patient will respond to treatment—especially functional appliance therapy—can transform your treatment plan, appliance choice, and patient counseling. Yet many students focus on memorizing appliance designs while overlooking the cephalometric predictors that actually determine whether treatment will succeed.
One of the most valuable—but often underemphasized—predictive tools lies in understanding mandibular morphology and growth potential, particularly concepts such as the Stutzman angle and the Co–Go–Me angle.
The Landmark Study That Shifted Prognostic Thinking
A pivotal investigation by Lorenzo Franchi and Tiziano Baccetti evaluated pretreatment cephalometric predictors of mandibular growth response in Class II patients treated during peak pubertal growth.
They analyzed 51 patients who underwent functional therapy with Twin Block or Herbst appliances at CS3 (peak growth stage). Importantly, their outcome measure was actual mandibular growth increase, not merely occlusal correction—making the findings especially clinically meaningful.
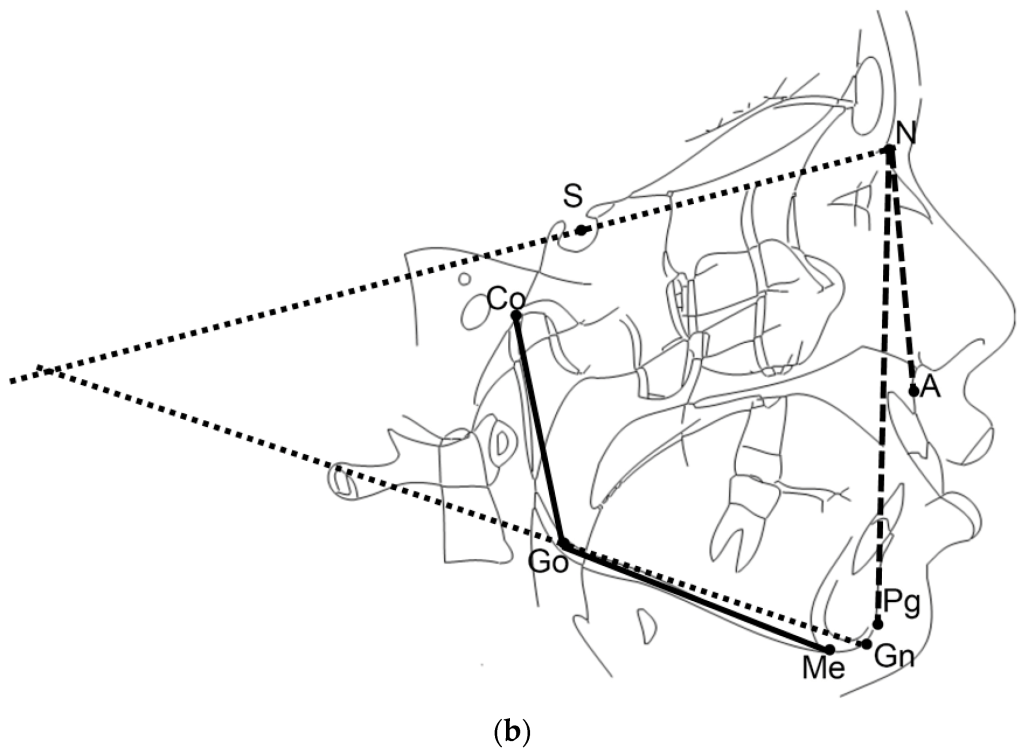
The Co–Go–Me Angle: A Powerful Prognostic Indicator
The mandibular angle Co–Go–Me (condylion–gonion–menton) has emerged as a highly practical predictor of treatment response.
< 125–125.5° → Favorable prognosis
> 125.5° → Poor prognosis
Interpretation Table
Value
Prognosis
Clinical Meaning
< 125.5°
Favorable
Strong mandibular growth potential
> 125.5°
Unfavorable
Limited skeletal response expected
Patients with smaller Co–Go–Me angles typically demonstrate greater mandibular growth during functional appliance therapy.
Additional Cephalometric Features That Predict Success
A strong skeletal response is more likely when the patient also presents with:
High Jarabak ratio (greater posterior vs anterior facial height)
Together, these features indicate a horizontal growth pattern, which is biologically more responsive to mandibular advancement therapy.
Viva one-liner: Co–Go–Me < 125° with low MP angle, low basal plane angle, and high Jarabak ratio indicates good prognosis for functional appliance therapy in Class II patients.
Memory Hook
Low angle = Grower → Treat confidently with functional appliance
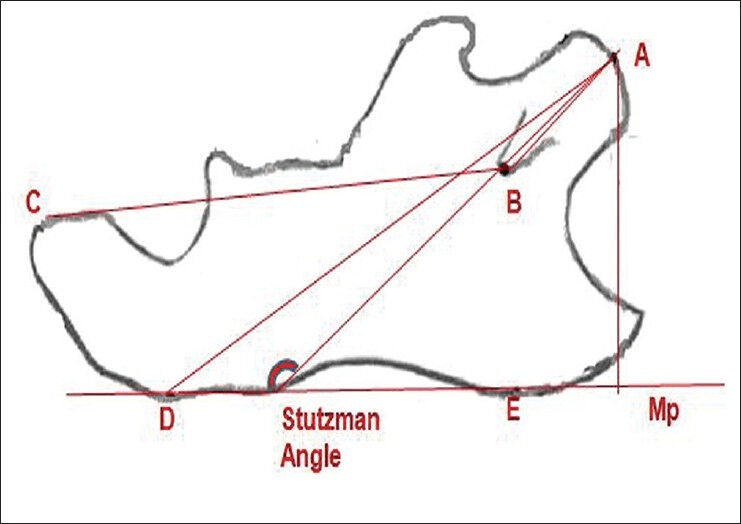
The Stutzman Angle: Direction Matters as Much as Amount
While Co–Go–Me predicts how much growth may occur, the Stutzman angle provides insight into how the mandible grows.
Definition: The Stutzman angle is formed between:
the condylar process axis (line from the most posterosuperior condylar point to the midpoint of the mandibular foramen), and
the mandibular plane
Clinical Significance
This angle reflects directional growth and biologic response, not just magnitude. It is especially useful for monitoring treatment progress over time.
Change
Meaning
Clinical Interpretation
Increase (Opening)
Condylar axis elongates/rotates
Active growth or forward positioning
No change
Minimal structural change
Limited skeletal response
Decrease (Closing)
Remodeling
Stabilization after advancement
Clinical rule: Opening = growth or advancement Closing = remodeling or stabilization
Why These Predictors Matter
Understanding these angles allows clinicians to move beyond trial-and-error treatment. Instead of hoping a functional appliance will work, you can predict response before treatment begins, improving:
Case selection
Treatment timing
Appliance choice
Patient counseling
Clinical confidence
In modern orthodontics, success isn’t just about mechanics—it’s about biologic forecasting. And mastering predictors like the Co–Go–Me and Stutzman angles gives you that edge.
If you’ve ever wondered how functional appliances actually stimulate mandibular growth, this is the idea that changes everything. Not muscles. Not magic. Not forced growth.
Instead — growth is relative.
Let’s break it down so clearly that you’ll remember it even during a 3 AM exam panic.
The Big Idea in One Line
Mandibular advancement doesn’t create new growth — it redirects existing growth potential through biomechanical signaling.
Why This Hypothesis Was Needed
For years, people believed that forward posturing appliances worked mainly because muscles became hyperactive and stimulated bone growth.
But that didn’t fully explain:
why growth changes occur even when muscles adapt
why both condyle and glenoid fossa remodel together
why relapse can occur when advancement stops
So researchers proposed the Growth Relativity Hypothesis — most notably explained by Voudouris.
The Three Forces That Actually Drive Growth
Think of mandibular advancement like stretching a spring-loaded system. Three biological forces start working simultaneously:
1️⃣ Displacement — The Trigger
When a functional appliance holds the mandible forward:
the condyle is physically displaced from its original fossa position
the joint must adapt to this new relationship
👉 Displacement = switch turns ON
2️⃣ Viscoelastic Tissue Pull — The Driver
Non-muscular tissues stretch:
retrodiscal tissues
capsule
ligaments
synovial structures
These tissues behave like elastic bands trying to pull the condyle back.
👉 This pull generates continuous biological signals.
3️⃣ Transduction Through Fibrocartilage — The Builder
The stretched forces don’t stay localized.
They spread through:
condylar fibrocartilage
glenoid fossa lining
This mechanical signaling stimulates:
bone apposition
remodeling
adaptive growth
👉 Transduction = signal converted into growth
The Golden Principle
Growth is not increased. It is redirected.
The condyle and fossa simply:
grow relative to their new displaced relationship
They are adapting — not overgrowing.
The Light-Bulb Memory Trick 💡
Imagine condylar growth as a light bulb with a dimmer switch:
Appliance activation → brightness increases
Tissue stretch → keeps light on
Appliance removal → light dims
You don’t create electricity. You just turn the dial.
Why Relapse Happens (And Students Forget This!)
After appliance removal:
stretched tissues recoil
muscles regain original balance
joint tries returning to old position
If retention isn’t managed → relapse tendency
The One Sentence You Should Write in Exams
Condylar and glenoid fossa growth during mandibular advancement is governed by displacement, viscoelastic tissue forces, and fibrocartilage force transduction, producing adaptive remodeling rather than true growth stimulation.
Memorize that line and you can answer:
theory questions
viva questions
mechanism questions
comparison questions
Ultra-Simple Analogy (Final Memory Lock 🔒)
Functional appliance = moving a plant toward sunlight You didn’t make the plant grow. You just changed where it grows.
Definition: Viscoelasticity describes the combination of viscous (fluid-like) and elastic (solid-like) properties exhibited by biological tissues. It primarily applies to elastic tissues such as muscles, but the concept extends to all non-calcified tissues.
Key Concepts:
It concerns both viscosity and flow of synovial fluids and elasticity of soft tissues including:
Retrodiskal tissues
Fibrous capsule
TMJ ligaments and tendons
Lateral pterygoid muscle (LPM) perimysium
Other non-muscular, non-mineralized soft tissues
Essentially, it explains how these tissues deform under stress and recover when the stress is removed, with a time-dependent response.
Historical Notes:
The concept faced opposition from Herren (1953), Harvold (1974), and Woodside (1973) to the original Anderson–Haupl theory, which had a different interpretation of joint tissue adaptation.
Stages of the Viscoelastic Reaction
The viscoelastic reaction proceeds through five sequential stages:
Emptying of blood vessels – initial vascular response to stress.
Pressing out interstitial fluid – displacement of tissue fluids to redistribute pressure.
Stretching of fibres – collagen and elastic fibers undergo elongation.
Elastic deformation of bone – bone matrix responds elastically under load.
Bioplastic adaptation – long-term remodeling and adaptation of supporting tissues.