🎬 WHY THIS PAPER EXISTS (The “So What” in 30 Seconds)
Orthodontics always taught: “Functional crossbite = symmetric mandible, just positioned wrong. Fix the maxilla, mandible self-corrects.” Clean. Simple. Reassuring.
Santos Pinto said: Not so fast.
In growing children, a mandible that’s been displaced for months to years actually remodels and becomes structurally asymmetric — especially at the ramus. This paper is the first to prove both morphological AND positional asymmetry exist simultaneously, and that early RPE can reverse both.
🔴 Examiner hook: “Functional crossbite means symmetric mandible.” — TRUE for adults, NOT fully true for growing children. This paper is your evidence.
LAYER 1 — POSITIONAL (Where is the mandible sitting?)
→ Whole mandible shifted LATERALLY + POSTERIORLY to crossbite side
→ Midline deviation = 1.6 mm toward crossbite side
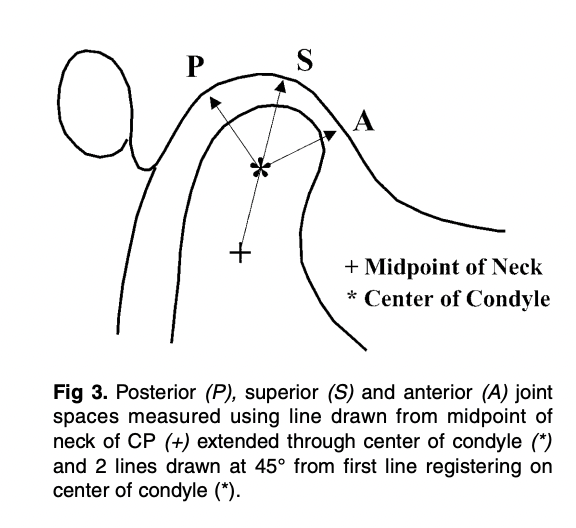
LAYER 2 — JOINT SPACE (Where is the condyle in the fossa?)
→ Noncrossbite condyle = more anterior on articular eminence
→ Superior joint space: 4.0 mm (non-XB) vs 3.2 mm (XB) ← SIGNIFICANT
→ Posterior: larger on non-XB (not significant)
→ Anterior: EQUAL on both sides ← MCQ TRAP
LAYER 3 — MORPHOLOGICAL (Has the bone actually changed shape?)
→ Yes! Ramus is SHORTER on crossbite side
→ Co–Sy: 75.5 mm (non-XB) vs 73.9 mm (XB) — 1.6 mm difference
→ Asymmetry in RAMUS (condyle + coronoid) but NOT in body (L6–L1 equal)
⚡ THE NUMBERS BANK — Memorise These 10 Numbers
Value
What It Represents
5.9–9.4%
Incidence of UPXB
67–79%
Proportion of UPXB that are functional
1.6 mm
Midline deviation + Co–Sy difference
~3 mm
L6 and coronoid horizontal offset (crossbite side more lateral)
4.0 vs 3.2 mm
Superior joint space (non-XB vs XB) — only SIGNIFICANT TMJ finding
8.8 yrs
Mean age of subjects
15
Sample size
1 month
RPE activation phase
6 months
Retention phase
11
Total SMV landmarks digitized
🔥 MECHANISM CHAIN — Viva Storytelling Version
Examiner: “Walk me through how FUPXB causes skeletal asymmetry.”
YOUR ANSWER:
Narrow maxilla creates a dental interference → mandible must shift from CR to ICP, deviating laterally and anteroposteriorly toward the crossbite side → this asymmetric posture alters condylar loading: noncrossbite condyle rides higher on the articular eminence → muscle compensation: anterior temporalis fires more on the noncrossbite side; posterior temporalis fires more on the crossbite side → sustained asymmetric forces trigger adaptive bone remodeling → the ramus on the crossbite side becomes shorter (both condylar and coronoid processes affected) → result: a functionally crossbited child now has a morphologically asymmetric mandible
🎯 EXAMINER TRAPS — Don’t Fall For These
Trap Statement
The Truth
“All joint spaces are asymmetric in FUPXB”
❌ Only superior space is significant; anterior joint spaces are EQUAL
“RPE doesn’t affect morphological asymmetry”
❌ RPE + retention eliminated morphological asymmetry — crossbite side grew MORE
“The mandibular body is asymmetric”
❌ L6–L1 distance is EQUAL — asymmetry is in the ramus only
“Glenoid fossa is asymmetric too”
❌ Fossa position showed little/no transverse or AP asymmetry
“Chewing patterns normalize after RPE”
❌ Reverse chewing sequencing persists even after correction
“Functional crossbite = symmetric mandible”
⚠️ Only in adults — in growing children, morphological change occurs
🧠 MUSCLE MNEMONIC — Never Mix This Up
“At the PARTY, Non-Cross goes FORWARD, Cross goes BACK”
ANTERIOR temporalis (forward-pulling) → fires more on NON-crossbite side
POSTERIOR temporalis (backward-pulling) → fires more on CROSSBITE side
📊 Pre vs. Post Treatment — What Changed?
Measurement
Pre-Treatment
Post-Retention
Verdict
Co–Sy side difference
Significant
Not significant
✅ Resolved
L6 lateral offset
~3 mm
~0 mm
✅ Resolved
Midline deviation (L1)
1.6 mm
Not significant
✅ Resolved
Superior joint space gap
Significant
Not significant
✅ Resolved
Glenoid fossa position
Not significant
Not significant
➡️ Unchanged (already symmetric)
Chewing pattern (reverse)
Abnormal
Still abnormal
❌ NOT resolved
🔑 Key insight on growth: Crossbite-side ramus grew MORE than noncrossbite side during treatment — compensatory catch-up growth. The mandible also rotated forward and medially on the crossbite side, and backward and laterally on the noncrossbite side.
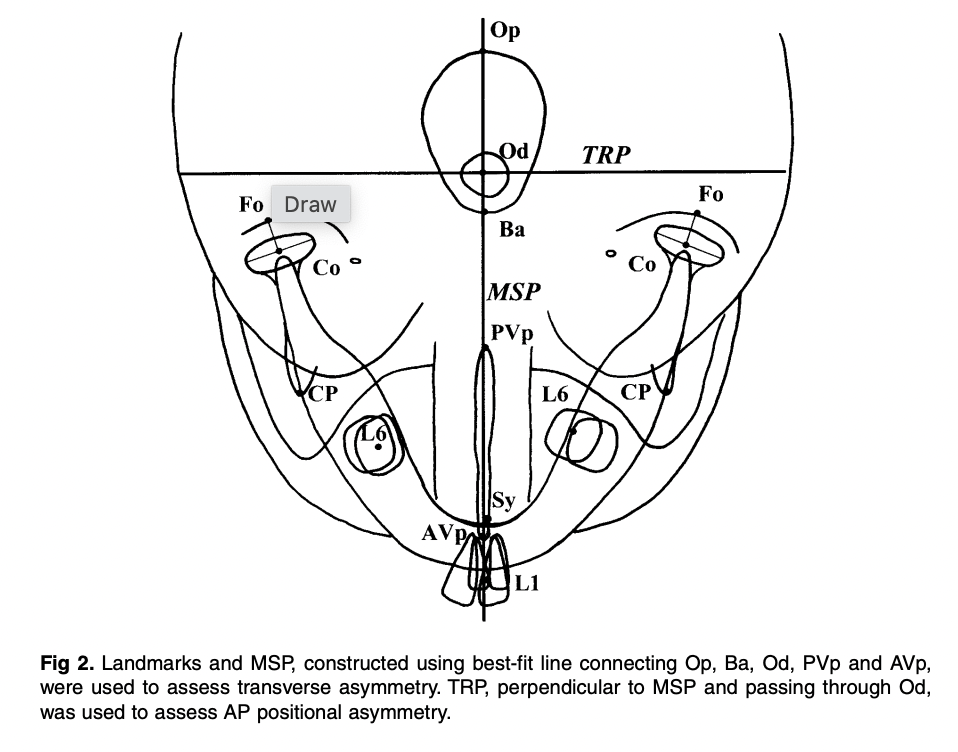
🏛️ LANDMARKS MNEMONIC (All 11 SMV Landmarks)
“Old Baboons Often Play Violins — Conducting Fine Concerts, Like Symphony”
❓ SELF-TEST — Rapid Fire (Cover answers, test yourself)
Question
Answer
Which ramus is LONGER in FUPXB?
Noncrossbite side
Which joint space is EQUAL on both sides?
Anterior
Which is the ONLY significantly different joint space?
Superior
Where does the asymmetry occur in the mandible?
Ramus (not body)
What persists even after successful RPE?
Reverse chewing sequencing
What muscle is more active on the noncrossbite side?
Anterior temporalis
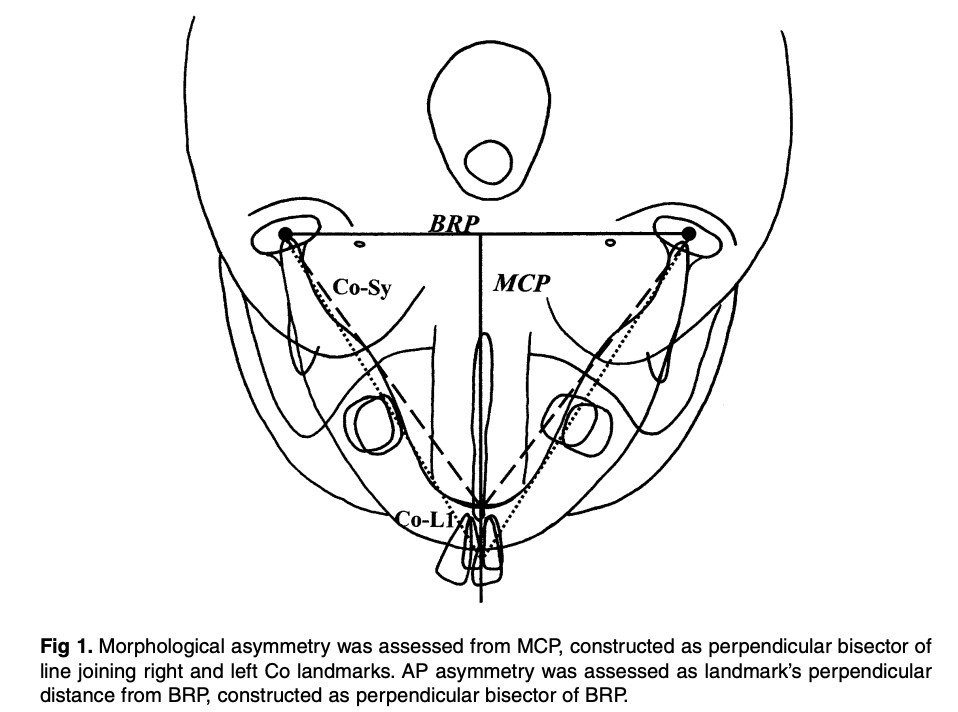
What does the MCP stand for and how is it constructed?
Midcondylar reference plane — ⊥ bisector of Co-Co line
What was the midline deviation pre-treatment?
1.6 mm toward crossbite side
Which radiograph assessed TMJ spaces?
Zonograms (4-turn spiral tomography)
What is the key conclusion that overturns classic teaching?
Functional crossbites cause morphological (structural) mandibular asymmetry in growing children
🩺 VIVA CLINCHER — The One Paragraph Examiners Love
“Santos Pinto et al. demonstrated that the classic view of functional crossbite as purely a positional problem is incomplete in growing children. Their prospective study showed the mandible is both positionally displaced and morphologically asymmetric — with the ramus shorter on the crossbite side due to adaptive remodeling. Crucially, the asymmetry is ramus-specific; the mandibular body remains symmetric. Early bonded RPE successfully resolved both layers of asymmetry through compensatory growth, though abnormal chewing patterns persisted, highlighting the need for functional rehabilitation post-treatment.”