

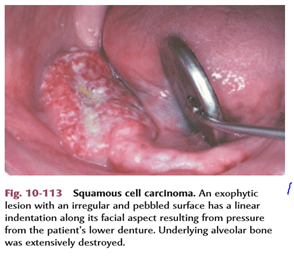
Squamous Cell Carcinoma (Epidermoid Carcinoma)
- SCC is defined as ‘a malignant epithelial neoplasm exhibiting squamous differentiation as characterized by the formation of keratin and/ or the presence of intercellular bridges‘.
- The epidermoid carcinoma is the most common malignant neoplasm of the oral cavity.
- The male-female ratio is approximately 2:1 for oral carcinoma, except for carcinoma of the vermilion border of the lower lip
ETIOLOGY:-
- The cause of oral squamous cell carcinoma is multifactorial.
- No single causative agent or factor (carcinogen) has been clearly defi ned or accepted, but both extrinsic and intrinsic factors may work .
- FACTORS:-
- TOBACCO SMOKING
- SMOKELESS TOBACCO
- BETEL QUID (PAAN)
- ALCOHOL
- PHENOLIC AGENTS
- RADIATION
- IRON DEFICIENCY
- VITAMIN-A DEFICIENCY
- SYPHILIS
- CANDIDAL INFECTION
- ONCOGENIC VIRUSES
- IMMUNOSUPPRESSION
- ONCOGENES AND TUMOR SUPPRESSOR GENES
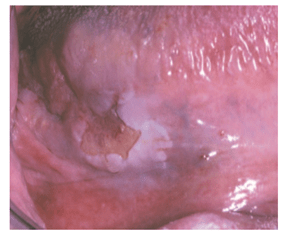
- CLINICAL FEATURES:-

- Oral squamous cell carcinoma has a varied clinical presentation, including the following:
● Exophytic (mass forming; fungating, papillary, verruciform)
● Endophytic (invasive, burrowing, ulcerated)
● Leukoplakic (white patch)
● Erythroplakic (red patch)
● Erythroleukoplakic (combined red-and-white patch)

- STAGING :-
Tumor size and the extent of metastatic spread of oral squamous cell carcinoma are the best indicators of the patient’s prognosis. Quantifying these clinical parameters is called staging the disease.
The most popular staging protocol, the tumor-node-metastasis (TNM) system.
This staging protocol depends on three basic clinical features:
1. T—Size of the primary tumor, in centimeters
2. N—Involvement of local lymph nodes
3. M—Distant metastasis
The American Joint Committee on Cancer (AJCC) designated staging by TNM Classification was used.
TNM clinical classification:-


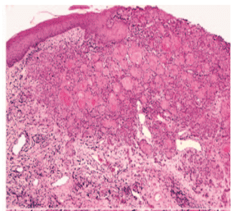
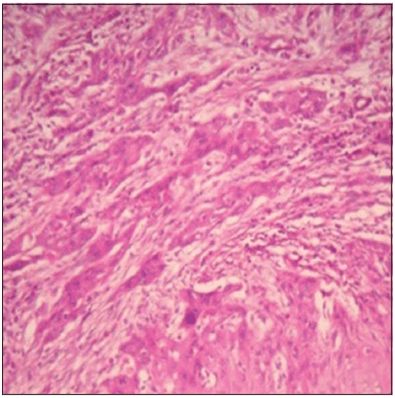
- HISTOPATHOLOGIC FEATUR:-
- Squamous cell carcinoma arises from dysplastic surface epithelium.
Features are:-
- sheets or islands of cells or cords
- a strong infl ammatory or immune cell response
- focal areas of necrosis
- invading into underlying muscles, bonesor adipose tissues
- angiogenesis
- desmoplasia or scirrhous change
- abundant eosinophilic cytoplasm with large, often darkly staining (hyperchromatic) nuclei
- increased nuclearto-cytoplasmic ratio.
- nuclear pleomorphism
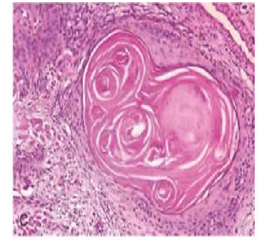
- keratin pearls (a round focus of concentrically layered keratinized cells)
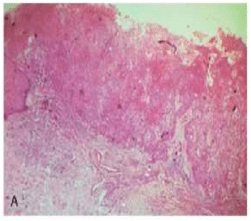
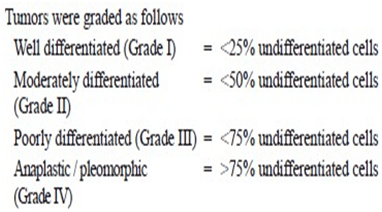
- GRADING:-
- Histopathologic evaluation of the degree to which these tumors resemble their parent tissue (squamous epithelium) and produce their normal product (keratin) is called grading.
- The one advantage of grading a tumour is that the grade reflects the anaplasticity of the lesion, which in turn indicates the general rapidity of growth, the rapidity of metastatic spread, the general reaction to be expected after X-ray radiation and the prognosis.
- There are 4 classifications used to describe grading systems :-
- 1-BRODERS CLASSIFICATION:-
- Broders’ system (1920) was first established on the basis of the proportion of highly differentiated cells in the tumour. Broders’ system was simple and widely used, it was a poor predictor for survival or me- tastasis.
* a system of grading tumours in which a grade 1 lesion was highly differentiated (its cells were producing much keratin), while grade 4 was very poorly differentiated (the cells were highly anaplastic and showed no keratin formation).
I-WELL DIFFERENTIATED:
-consists of sheets and nests of cells
-cells are generally large
– intercellular bridges or tonofibrils are not demonstrated.
-The nuclei are large and demonstrate variability in the intensity of the staining reaction.
-Nuclei that stain heavily with hematoxylin are referred to as hyperchromatic.
-mitotic figures may be found(Many of these mitotic figures are atypical.)
-the most prominent features of the welldifferentiated epidermoid carcinoma is the presence of individual cell keratinization-the formation of numerous epithelial or keratin pearls of varying size.
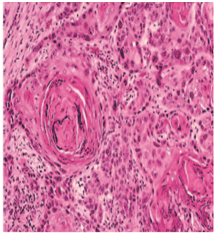
II– ModeratelyDifferentiated epidermoid carcinomas:
– lose certain features so that their resemblance to squamous epithelium is less pronounced
-The characteristic shape of the cells and their arrangement may be altered.
– The growth rate of individual cells is more rapid,
– the greater number of mitotic figures,
– even greater variation in sizes, shape and tinctorial reaction,the failure to carry out the function of a differentiated squa- mous cell, the formation of keratin.
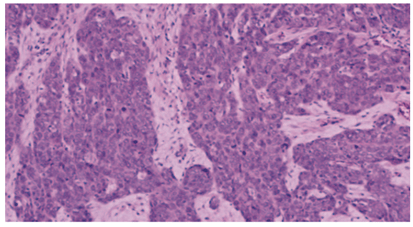
III-POORLY DIFFERENTIATED TYPE:
-bear little resemblance to their cell of origin
-will often present diagnostic difficulties because of the primitive and uncharacteristic histological appearance of malignant,
-rapidly dividing cells
– cells show an even greater lack of cohesiveness and are extremely vagarious.

2.JAKOBSS0N’s GRADING SYSTEM:-
-In 1973, Jakobsson et al developed a multifactorial
grading system which had the advantage of scoring tumour-host interactions and tumour characteristics, but eventually proved to be useful only when applied to tongue cancers.
-Parameters used in Jakobsson’s method are:-
i- KRE- keratinization
ii-NP- nuclear pleomorphism
iii-MIT-mitosis
iv-POI- pattern of invasion
v-LPR- lympho-plasmocyticrspon
Tumor cells invading in strands and cords
-Similar findings were observed in Anneroth and Hansen’s grading where the criteria were similar except that the parameter vascular invasion (VI) was omitted.
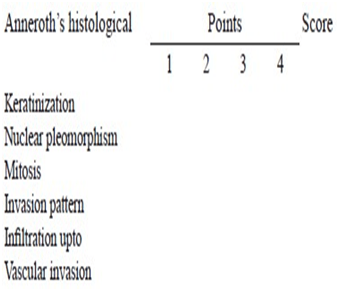
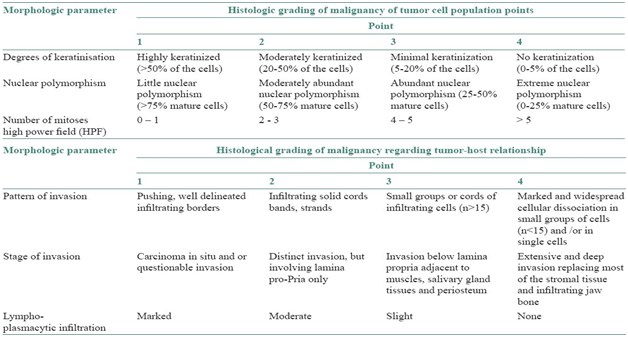
3-Anneroth’s classification:
- This system is constituted by six histological variables of equal value in the determination of the grade of malignancy, three connected with the tumor cellular population (differentiation and proliferation mitosis) and the other three connected with tumor-host relationship (pattern and stage of invasion; and cellular response).
Anneroth’s classification (multifactor grading system)
-According to the classification, three parameters reflecting tumor cell features including keratinization, polymorphism, and mitoses were evaluated in the whole thickness of the tumor and each was scored from 1 to 4. Mode of invasion and inflammatory infiltration representing tumor-host relationship were graded in the most invasive margins and scored from 1 to 4:
-Variables such as:-
i-pattern of invasion,
ii- tumor thickness,
iii-degree of keratinization,
iv-nuclear pleomorphism,
v-lymphocytic response,
vi-mitotic rate
4.BRYNE’S GRADING SYSTEM:-
-Bryne et al (1989) modified Anneroth’ s grading system and developed a malignancy grading focusing on the invasive front of the tumour.
– This method of grading appeared to be less time-consuming in the assessment of the neoplasm.
-Nevertheless, this system is not sufficiently homogeneous to allow grading parameters to be assessed individually
-This was performed at the invasive tumor front (ITF).
-The Bryne’s grading system is more predictive for LNM as compared with the multifactorial grading systems that is, Jakobsson’s and Anneroth and Hansen’s. Broder’s grading system is of no prognostic value.
-Parameters used are:-
i-Keratinisation
ii-nuclear polymorphism
iii-mitosis
iv-pattern of invasion
v-lympho-plasmocytic response
vi-lymph nodes
REFERENCES :
| 1.Comparative study of various grading systems in oral squamous cell carcinoma and their value in predicting lymph node metastasis |
| Saleha Jamadar1, TV Narayan1, Balasundari Shreedhar2, Leeky Mohanty1, Sadhana Shenoy1 1 Department of Oral Pathology and Microbiology, The Oxford Dental College, Hospital and Research Centre, Bommanahalli, Bengaluru, Karnataka, India 2 Department of Oral Pathology and Microbiology, Career Dental College, Lucknow,Uttar Pradesh, India |
2.A study on histological grading of oral squamous cell carcinoma and its co-relationship with regional metastasis
M Akhter, S Hossain, Quazi B Rahman, Motiur R Molla
Department of Oral and Maxillofacial Surgery, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh
3.Shafer’s Textbook of Oral Pathology,8e
4.NEVILLE -Oral & Maxillofacial Pathology,3e


Awesome !!
LikeLiked by 1 person
Thank you 🙂
LikeLike