HABIT– It’s a tendency towards an act that has become a repeated performance either fixed, consistent and easy to perform by an individual.HABITS which do not apply a direct force on the teeth or its supporting structures are termed non-pressure habits. An example of a non-pressure habit is mouth breathing.
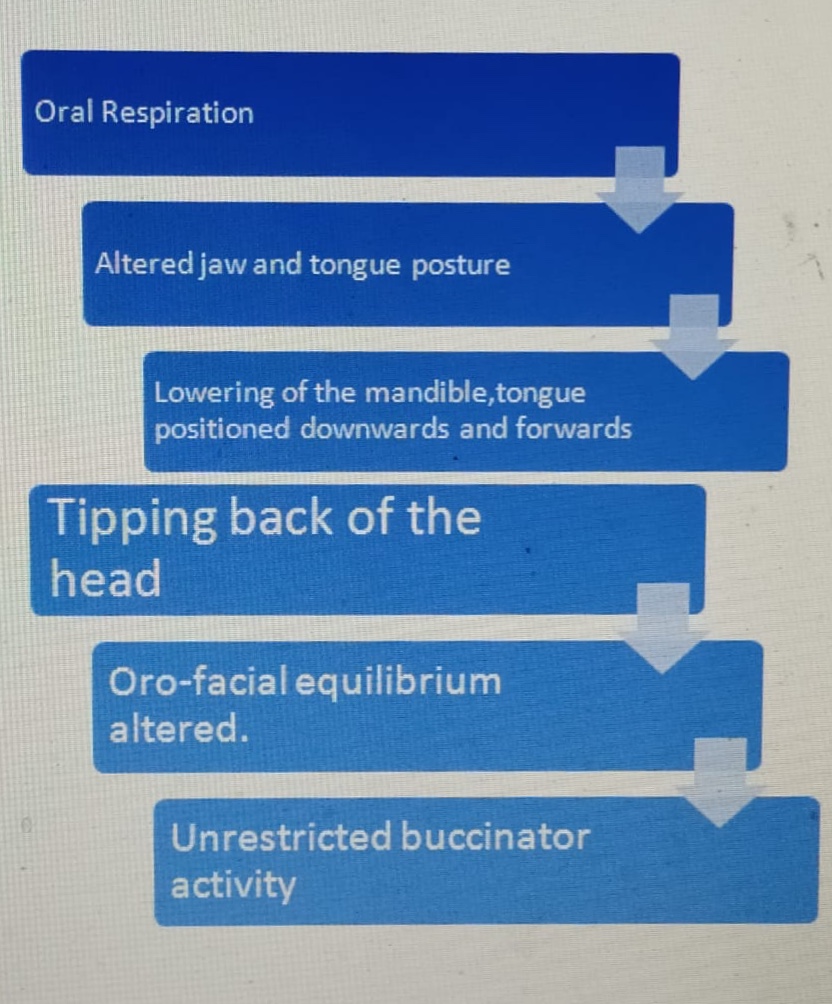
MOUTH BREATHING HABIT– Habitual respiration through the mouth instead of the nose. It’s a possible etiological factor for malocclusion. The mode of respiration influences the posture of the jaw, the tongue and to a lesser extent the head. Thus mouth breathing could alter the oro-facial equilibrium thereby leading to malocclusion. Most normal people indulge in mouth breathing when they are under physical exertion such as during strenuous exercise or sports activity.
Classification based on etiology of Mouth breathing:
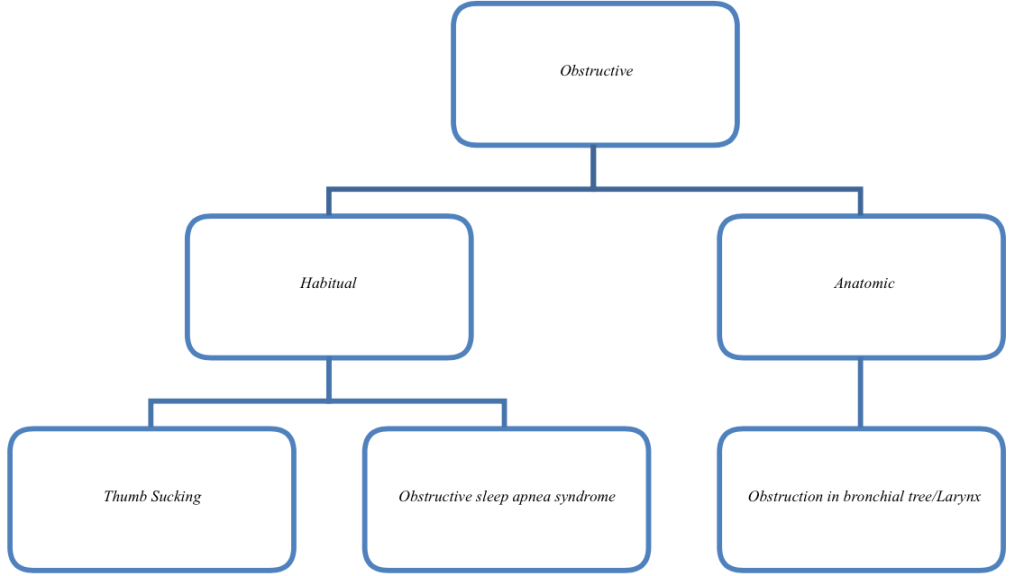
Mouth breathers can be classified into 3 types:
a. OBSTRUCTIVE–Causes of nasal obstruction:
-Enlarged Turbinates
-Enlarged Adenoids
-Deviated Nasal Septum
-Nasal polyps
-Allergic Rhinitis
-Chronic inflammation of nasal mucosa
-Benign tumors.
Ectomorphic children with tapering face and nasopharynx-Genetics-prone to develop nasal obstruction.
b. HABITUAL: A habitual mouth breather is one who continues to breathe through his mouth even though the nasal obstruction is removed. It becomes a deep rooted habit that is performed unconsciously.
c. ANATOMIC: Abnormally short upper lip preventing proper lip seal.
PATHOPHYSIOLOGY:
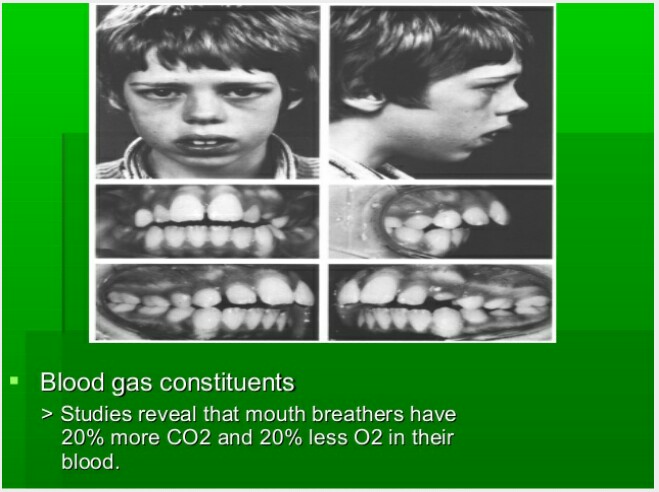
CLINICAL FEATURES OF MOUTH BREATHING: The type of malocclusion most often associated with mouth breathing is called long face syndrome or the classic adenoid facies. These patients exhibit the following features:
a. Long and narrow face.
b.Narrow nose and nasal passage.
c. Short and flaccid upper lipd.
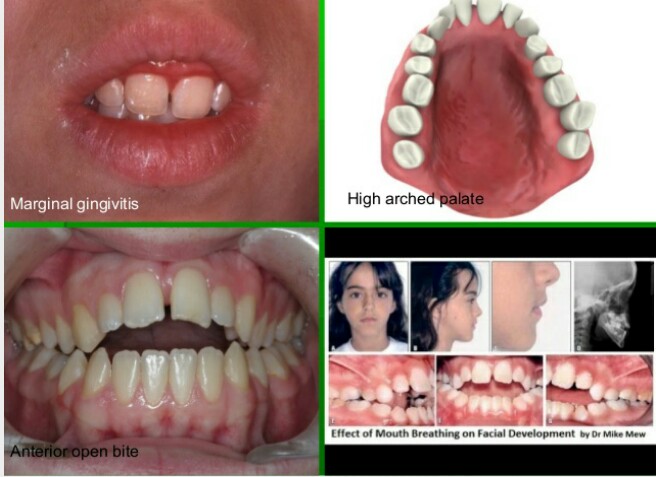
d. Contracted upper arch with possibility of posterior cross bite
e. An expressionless face
f. Increased overjet as a result of flaring of the incisors.
g. Anterior marginal gingivitis can occur due to drying of the gingiva.
h. The dryness of the mouth predisposes to caries.
i. Anterior open bite can occur
DIAGNOSIS OF MOUTH BREATHING:
History: A good history should be recorded from the patient as well as parents.
Clinical examination: Look out for its various clinical features. A number of simple tests can be carried out to diagnose mouth breathing such as mirror test, water test etc.
a. Mirror test: Also called as fog test. A double sided mirror is held between the nose and mouth. Fogging on the nasal side indicates nasal breath while fogging on oral side-mouth breathing.
b. Massler’s water holding test: Patient is asked to hold the mouth full of water.


Cephalometrics: Cephalometric examination helps in establishing the amount of nasopharyngeal space, size of adenoids and also helps in diagnosing long face associated with mouth breathing.
Rhinomanometry: It is the study of nasal airflow characteristics using devices consisting of flow meters and pressure gauges. These devices help in estimation of airflow through the nasal passage and nasal resistance.
MANAGEMENT:
1. Removal of nasal or pharyngeal obstruction: Any nasal or pharyngeal obstruction should be removed by referring the patient to the E.N.T surgeon.
2. Interception of the habit:
- Through physical exercises, lip exercises & maxillothorax myotherapy.
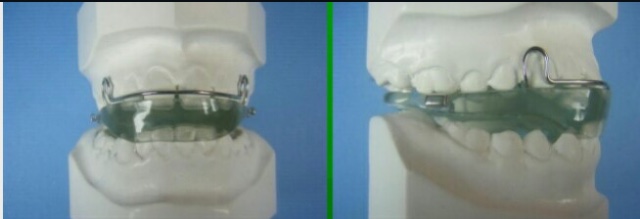
- Use of a vestibular screen
- Alternatively adhesive tapes can be used to establish the lip seal.
3. Rapid Maxillary Expansion:
Patients with narrow, constricted maxillary arches benefit from rapid palatal expansion procedures aimed at widening the arch.RME has been found to increase the nasal airflow and decrease the nasal air resistance.
4. Correction of malocclusion:
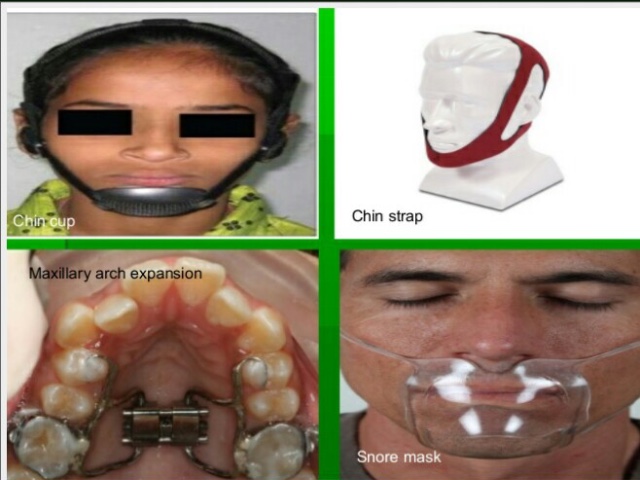
- Class I: Oral shield appliance
- Class II div.1: Monobloc activator
- Class III: Chin cap, interceptive methods.


References: Textbook of Orthodontics The Art and Science 6th Edition By Bhalajhi! Random google images.


[…] https://dentowesome.wordpress.com/2020/04/06/mouth-breathing/ […]
LikeLike