• Swellings at the angle of Mandible include: ✍🏻👇🏻
🔅Congenital disease
• Branchial Cleft Cyst
🔅Neoplasm
(i) Benign
Hemangioma
Lymphangioma, Cystic hygroma
Pleomorphic adenoma (mixed tumor)
Warthin tumor
Neurofibroma
Angiolipoma
Adenoma
Hamartoma
Lipoma
Oncocytoma
(ii) Malignant
Mucoepidermoid carcinoma
Squamous cell carcinoma
Adenoid cystic carcinoma
Acinic cell carcinoma
Adenocarcinoma
Rhabdomyosarcoma
Lymphoma, leukemia
Metastatic adenopathy
🔅Inflammation/Infection
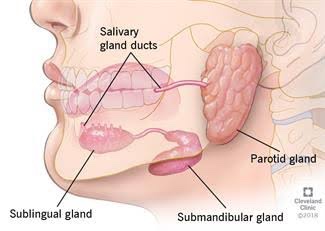
Parotitis
Parotid Abscess
Tuberculosis
Sarcoidosis
Sjögren disease
HIV
Detailed View🔍
1) Branchial Cleft Cyst:
Failure of involution of clefts and pouches lead to cysts, fistulas or sinus tracts.
Its a painless fluctuant swelling
First branchial cleft cysts are rare usually located at parotid gland or periparotid region.
Second branchial cleft cyst – Type II are the most common
Typically, second branchial cleft cysts present as a rounded swelling just below the angle of mandible, anterior to the sternocleidomastoid
2) Hemangiomas:
They are the most common benign salivary gland mass. Capillary hemangiomas involve parotids
3) Lymphangiomas
They are congenital malformations of the lymphatic system that may involve the parotid gland (Soft asymptomatic neck mass associated with facial asymmetry)
4) Pleomorphic Adenoma:
Hard painless slow growing mass
5) Warthin Tumor:
Incorporation of heterotopic salivary gland ductal epithelium within intraparotid & periparotid nodes
6) Parotitis & Parotid Abscess:
Most common in children
Mumps is the most common viral cause of parotitis
The condition manifests tender swelling at the angle of Mandible
Sialadenitis is most commonly due to bacterial infections caused by Staphylococcus aureus.
Premature neonates and immunosuppressed individuals are affected.
• Swellings in the floor of Mouth: 👇🏻✍🏻
Ranula presents as a translucent blue, dome-shaped fluctuant swelling & contains viscid, glairy jelly like fluid
Ranula – a type of mucocele found on the floor of the mouth. Present as a swelling of connective tissue consisting of collected Mucin from a ruptured salivary gland by local trauma.
Swellings in the floor of the mouth are more likely to arise from structures above the Mylohyoid muscle. The commonest swellings in the floor of the mouth are denture induced hyperplasia & salivary calculus.
Swellings in the floor of the mouth may inhibit swallowing & speech.
Mandibular tori produce bony hard swelling lingual to the lower premolars.
Torus palatinus is an intrinsic bone lesion whereas a dental abscess pointing on the palate (usually from the palatal roots of the 1st & 2nd maxillary molars or from upper lateral incisors) is extrinsic.
Salivary neoplasms
Invasive carcinoma from the maxillary sinus may produce a palatal swelling.
Kaposi’s sarcoma, typical of HIV/AIDS may also present as lump on palate.
Rest is necessary for the prompt healing of wounds. Ambulatory patients should be directed to go home & remain quiet for several hours, preferably sitting in a comfortable chair or, if lying down, keeping the head elevated on several pillows.
Only liquids and soft solids should be eaten the first day. They may be warm or cold but not extremely hot.
Food intake should not begin until several hours after surgery to avoid disturbing the blood clot.
If the extractions were limited to one side, chewing can be done on the unoperated side, but when local anesthesia has been used, chewing should be avoided until sensation has returned.
Fluids should be taken in greater amounts than usual to prevent dehydration from limited food intake.
A normal diet should be resumed as soon as possible, since this facilitates healing.
Some degree of postoperative pain accompanies many exodontic procedures and begins after the effects of anesthetic have left. This is considered a normal response to the unavoidable trauma of surgery.
In most cases, such pain lasts no more than 12 to 24 hours, although a traumatic periostitis may persist for several days.
Ordinarily this type of pain can be controlled by the use of cold packs (30 minutes per hour) during the first 24 hours & the proper administration of analgesic drugs.
For mild pain, as after a routine extraction, one of the antipyretic analgesics is usually adequate.
For moderate pain, such as after removal of an impacted tooth, a drug such as codeine or meperidine (Domerol) should be used.
Narcotics are needed only in rare instances.
The combination of a sedative drug with an analgesic agent can also be used but barbiturate alone should never be used to relieve pain as it can result in mental disorientation in a patient suffering from extreme pain.
The degree of swelling that occurs is generally in direct proportion to the degree of surgical trauma.
The application of cold to the operated site helps diminish postoperative swelling. If a rubber ice bag is not available, the ice can be placed in a plastic bag.
Cold can be applied intraorally by holding an ice cube in the mouth.
Pressure dressings can also be beneficial in limiting postoperative swelling.
Once swelling has reached the maximum (usually after 24 to 48 hours), cold is no longer effective, and heat, in the form of moist compresses, should be applied. It too should be used only 30 minutes per hour. The area should be lubricated with petroleum jelly to avoid burning the skin.
Intraoral heat is achieved by the use of hot isotonic saline rinses.