Understanding the growth patterns of the maxillary and mandibular lips is essential for effective orthodontic treatment planning. As orthodontic students, recognizing the interplay between facial soft tissues and the underlying hard tissues, particularly during the critical growth period from 8 to 18 years, can significantly influence treatment outcomes. This blog post delves into a lip growth and its implications for orthodontic therapy, providing data-driven insights and clinical guidelines.
Key Findings on Lip Growth
1. Maxillary Lip Length
| Maxillary Lip Length Growth (mm) | Age 8 | Age 18 | Percentage Increase | Largest growth occurred between |
|---|---|---|---|---|
| Males | 17.73 | 21.53 | 21.43% | Ages 10 and 16. |
| Females | 17.73 | 19.88 | 12.11% | Ages 10 and 14. |
2. Maxillary Lip Thickness
| Maxillary Lip Thickness Growth (mm) | Age 8 | Age 18 | Percentage Increase | |
| Males | 10.77 | 15.76 | 46.33% | Growth was continuous, with the largest increase between ages 12 and 16. |
| Females | 10.90 | 12.50 | 14.68% | Growth occurred primarily between ages 10 and 14. |
3. Mandibular Lip Length
| Mandibular Lip Length Growth (mm) | Age 8 | Age 18 | Percentage Increase | |
| Males | 19.14 | 26.53 | 38.56% | Largest increase occurred between ages 12 and 16. |
| Females | 19.14 | 22.73 | 18.65% | Growth occurred primarily between ages 10 and 16. |
4. Mandibular Lip Thickness
- Males: Increased steadily from ages 8 to 16, with a plateau between ages 16 and 18.
- Largest increases occurred between ages 14 and 16.
- Females: Growth was less pronounced, with significant increases only between ages 10 and 14.
Clinical Implications for Orthodontic Treatment
1. Sexual Dimorphism in Lip Growth
- Males experience greater increases in both lip length and thickness compared to females.
- Females show more limited growth, particularly in lip thickness during puberty.
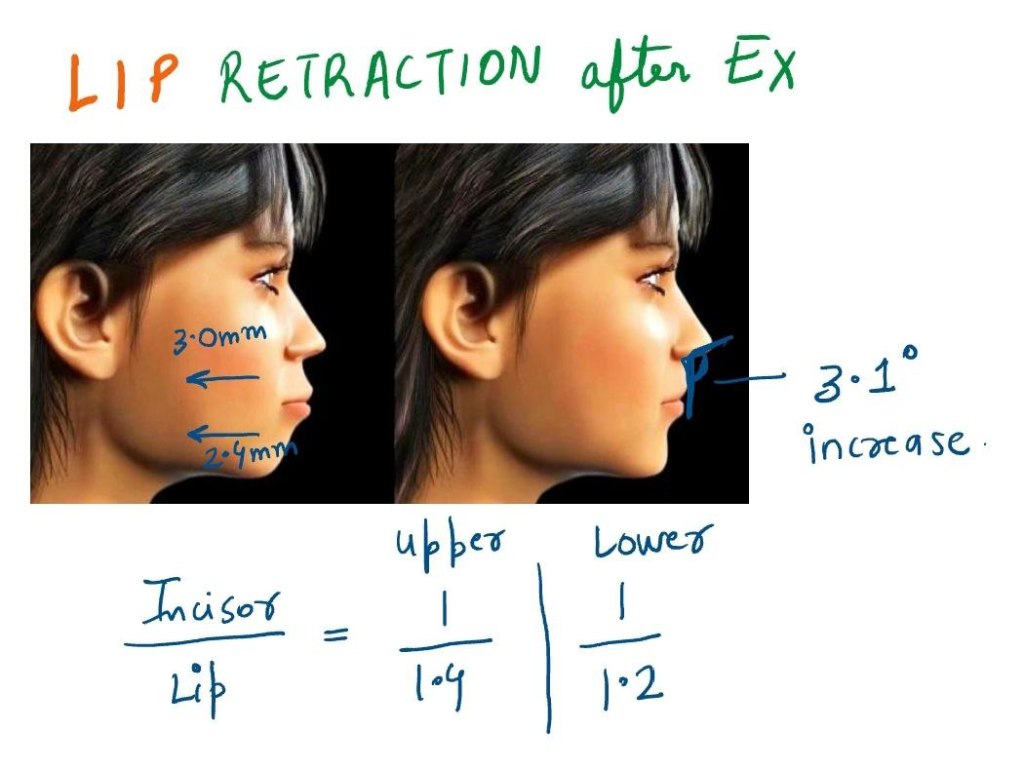
2. Extraction Therapy Considerations
- Female Patients: Limited lip thickening during puberty makes the effects of extraction therapy more noticeable, especially in patients with straight or concave profiles. Treatment plans should be approached with caution to avoid adverse effects on facial esthetics.
- Male Patients: Greater lip thickening provides more flexibility for extractions without significantly impacting facial profile fullness.
Maxillary Lip Thickness Growth Rates
- Males:
- 0.5 mm/year (ages 8–12).
- 0.7 mm/year (ages 12–16).
- Females:
- 0.5 mm/year (ages 10–12).
- 0.3 mm/year (ages 12–14).
Conclusion
Understanding the growth patterns of maxillary and mandibular lips is essential for predicting soft-tissue responses and planning effective orthodontic treatments. Sexual dimorphism plays a significant role, with males experiencing greater growth in both lip length and thickness compared to females. These differences must be factored into treatment decisions, particularly for extraction therapy, to ensure optimal esthetic and functional outcomes. As orthodontic students, incorporating these insights into clinical practice will enhance your ability to deliver patient-centered care.