• Types of giant cells - grossly classified into 2 types. – • The giant cells which exist in normal tissue (physiological) e.g osteoclasts in bones, trophoblasts in placenta, odontoclast, straited muscle.
• The giant cells which exist pathological -eg. Foreign body giant cells Langhan's giant cells Touton giant cells Aschoff giant cells Anaplastic cancer giant cells Reed-Sternberg giant cells
Curated by: Dr. Tabassum Sayyad (Dental Intern – MARDC)
Leukemias are malignant Neoplasms of the haematopoetic stem cells characterized by diffused replacement of bone marrow by Neoplastic cells with or without involvement of the peripheral blood.
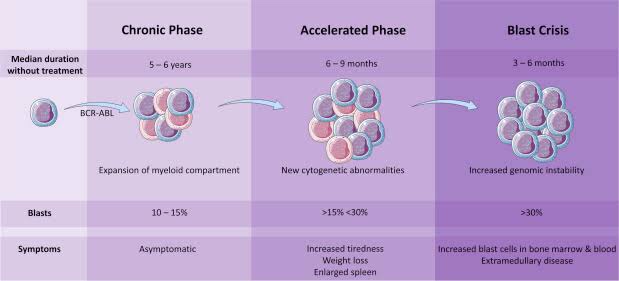
➡️ Chronic leukaemia is a disease of insidious onset, affecting middle aged & young adults (CML)
🔅CLINICAL FEATURES:
Gradually developing Anaemia
Hepatosplenomegaly (In CML, a massive splenomegaly reaching upto the umblicus) Therefore, acute pain due to splenic infarction
The standard treatment for chronic phase CML is a tyrosine kinase inhibitor (TKI) like imatinib oral therapy. Imatinib works by reducing the production of abnormal white blood cells.
Allogenic bone marrow transplants.
Interferon was once the best treatment for CML, but now, the tyrosine kinase inhibitors are the mainstay of treatment and interferon is rarely used. To treat CML, this drug is most often given as a daily injection (shot) under the skin. It may also be injected into a muscle or vein. It’s given for many years.
Chemotherapy: Today, chemo may be used to treat CML when the TKIs have stopped working. It’s also used as part of a stem cell transplant.
Others:
Splenectomy
Splenic irradiation
Leukapheresis
🔘 Splenectomy and splenic irradiation have been used in patients with large and painful spleens, usually in the late phase of CML. This is rarely needed in patients whose disease is well controlled.
🔘 For those patients unable to tolerate chemotherapy, leukapheresis is a viable option.
Dr. Mehnaz Memon🖊
References:
Textbook of Pathology, Harsh Mohan; Internet articles
🔹OEDEMA〰️Swelling. Abnormal/excessive accumulation of free fluid in the interstitial tissue spaces & serous cavities.
🔹Accumulation of fluid (abnormally) inside the cell is intracellular edema/hydropic degeneration.
🔹Accumulation in body cavities:
Peritoneal Cavity – Ascitis
Pleural Cavity – Hydrothorax (T.B)
Pericardial cavity – Hydropericardium
TYPES OF OEDEMA👆🏻
🔹PITTING & NON-PITTING EDEMA:
Source: Healthline
➡️ When interstitial fluid volume increases, most of the fluid becomes free that is not bound to proteoglycan meshwork. This type of edema is called pitting edema because when this area is pressed with finger, fluid gets displaced producing depression or a pit as seen in SUBCUTANEOUS TISSUES.
➡️ Edema also develops due to swelling of the cells/clotting of interstitial fluid in the presence of fibrinogen. This is called Non-pitting/solid edema because its hard & a pit is not formed by pressing.
e.g. – Myxodema
– Elephantiasis
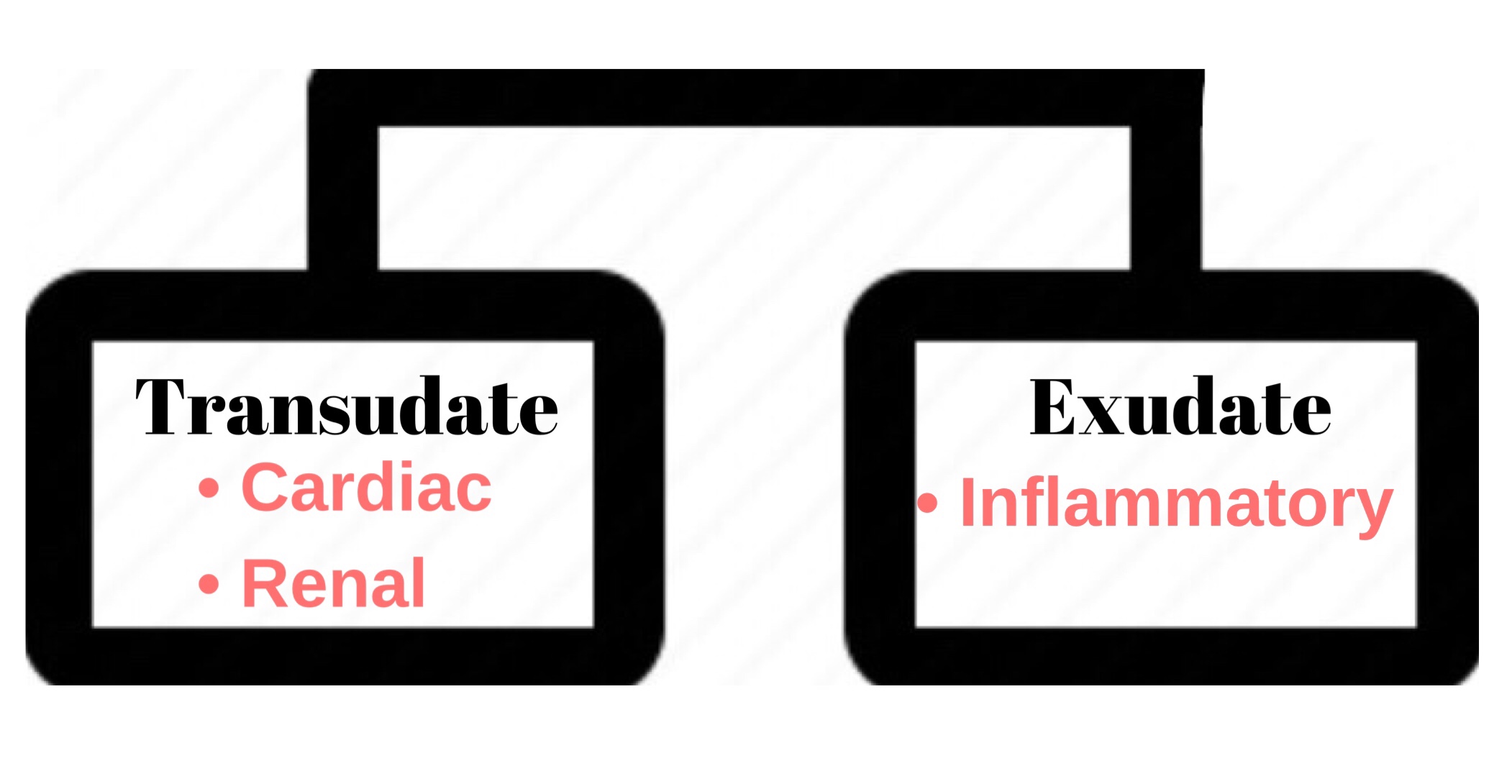
Oedema Fluid
🔹 Pathogenesis of Edema:
➡️ Causative mechanisms that produce edema are:
⬇️ Plasma oncotic pressure
⬆️ capillary hydrostatic pressure
Lymphatic obstruction
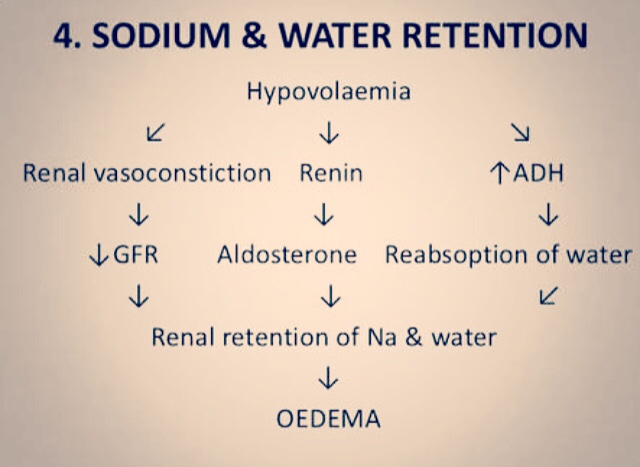
Sodium & Water retention
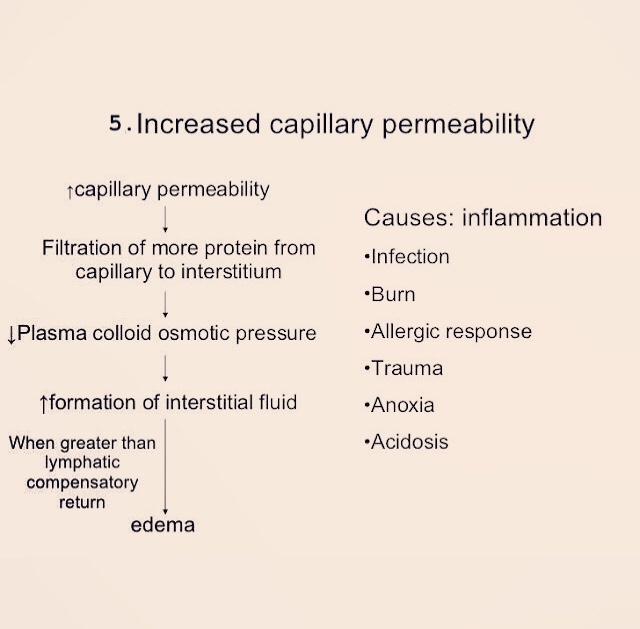
⬆️ capillary permeability
Tissue factors
These mechanisms interfere with normal fluid balance of plasma, interstitial fluid & lymph flow.
It is exerted by total amount of plasma proteins that tend to draw fluid into the vessels normally.
A fall in the total plasma protein level (<5g/dl), results in lowering of plasma oncotic pressure in a way that it can no longer counteract the effect of hydrostatic pressure of blood.
Therefore, increased outward movement of fluid from capillary wall & decreased inward movement of fluid from the interstitial space causing edema.
Fluid pressure and colloid osmotic pressure forces operate at the capillary membrane, tending to move fluid either outward or inward through the membrane pores
Hypoproteinaemia usually produces generalized edema
Hypoalbuminaemia – <2.5g/dl albumin concentration has 4 times higher plasma oncotic pressure than globulin
➡️ Fluid from capillary wall to interstitial space by counteracting the force of plasma oncotic pressure.
➡️ Edema results when hydrostatic pressure at Venular end of capillary wall(12mmHg) becomes more than the plasma oncotic pressure, resulting in no reabsorption of fluid at the Venular end.
Example, edema of Cardiac disease – Congestive cardiac failure, constrictive pericarditis
Cirrhosis of liver
Passive congestion – e.g. mechanical obstruction due to thrombosis of veins of lower legs, varicosities, pressure by pregnant uterus, tumours etc.
Postural edemae.g. ⬆️ Venous pressure (Edema of feet & ankle)
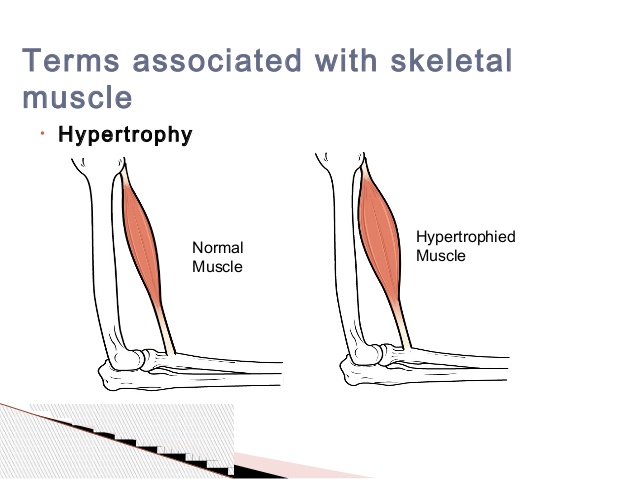
Increase in the size of the organ or tissue due to increase in the size of the cells
WHAT CAUSES HYPERTROPHY?
Due to increase in the functional demand/workload
1.PHYSIOLOGICAL
Hypertrophy of skeletal muscles- Ex- bulging muscles of athletes
Hypertrophy of the smooth muscles- Ex- growth of the the uterus during pregnancy from estrogenic stimulation
Source – Google
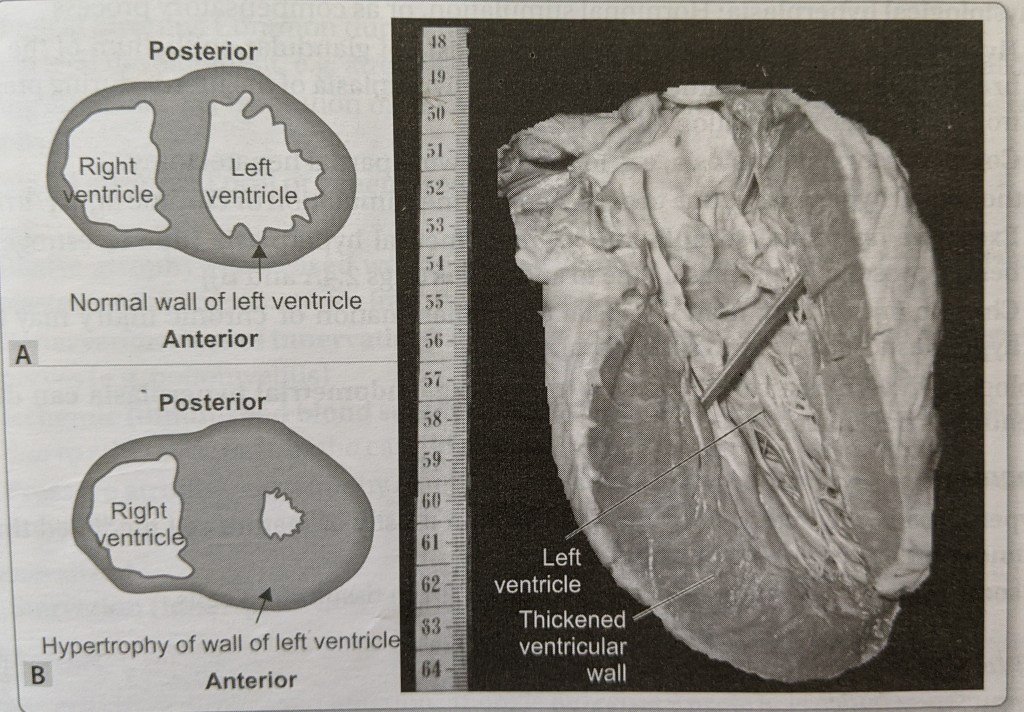
PATHOLOGICAL
Hypertrophy of cardiac muscle – left ventricular hypertrophy or damaged valves ( aortic stenosis, mitral incompetence)
Hypertrophy of smooth muscle– hypertrophy of the urinary bladder in response to urethral obstruction ( prostrate hyperplasia) and hyperplasia of the stomach due to pyloric stenosis .
Source – pathology preparatory manual for dental students – Ramdas NayakSource – Google
Mechanism of hypertrophy –
It occurs due to synthesis of the cellular proteins .
Mechanism involved in the hypertrophy of cardiac muscle-
Physiological hypertrophy– Due to increase in the workload causes mechanical stretch of the myocardium.
Pathological hypertrophy– due to to growth factors and hypertrophy agonists-
Introduction & Etiology👆🏻Clinical Features & Phases of PDB..👆🏻Clinical Features contd…👆🏻O/M of PDB..👆🏻Radiographic Features of PDB..👆🏻Histological Features of PDB…👆🏻Lab. Findings & Treatment of PDB..👆🏻
References: Shafer’s Textbook of Oral Pathology 7th Edition