The extraction of a tooth requires the separation of its attachment to the alveolar bone via the crestal and principal fibers of the periodontal ligament. Also involved is a process of expanding the alveolar socket.
After the tooth has been removed, the form of alveolar process is restored by finger pressure. Bleeding is arrested by means of a pressure pack placed between the jaws, and the wound is allowed to fill with a blood clot.
EXODONTIC PROCEDURES:
The following techniques may be used for tooth removal:
- the forceps technique
- the elevator technique (https://dentowesome.wordpress.com/2020/06/18/dental-elevators/)
- the open view technique
Odontotomy can be used to facilitate any of these three procedures.
ODONTOTOMY
- In some instances the extraction may be simplified by cutting a tooth apart. This is especially desirable in the case of multi-rooted deciduous or permanent teeth with severely divergent roots.
- It is also useful in cases where the crown is so decayed that only a shell remains. (As shown in the figure👇🏻)
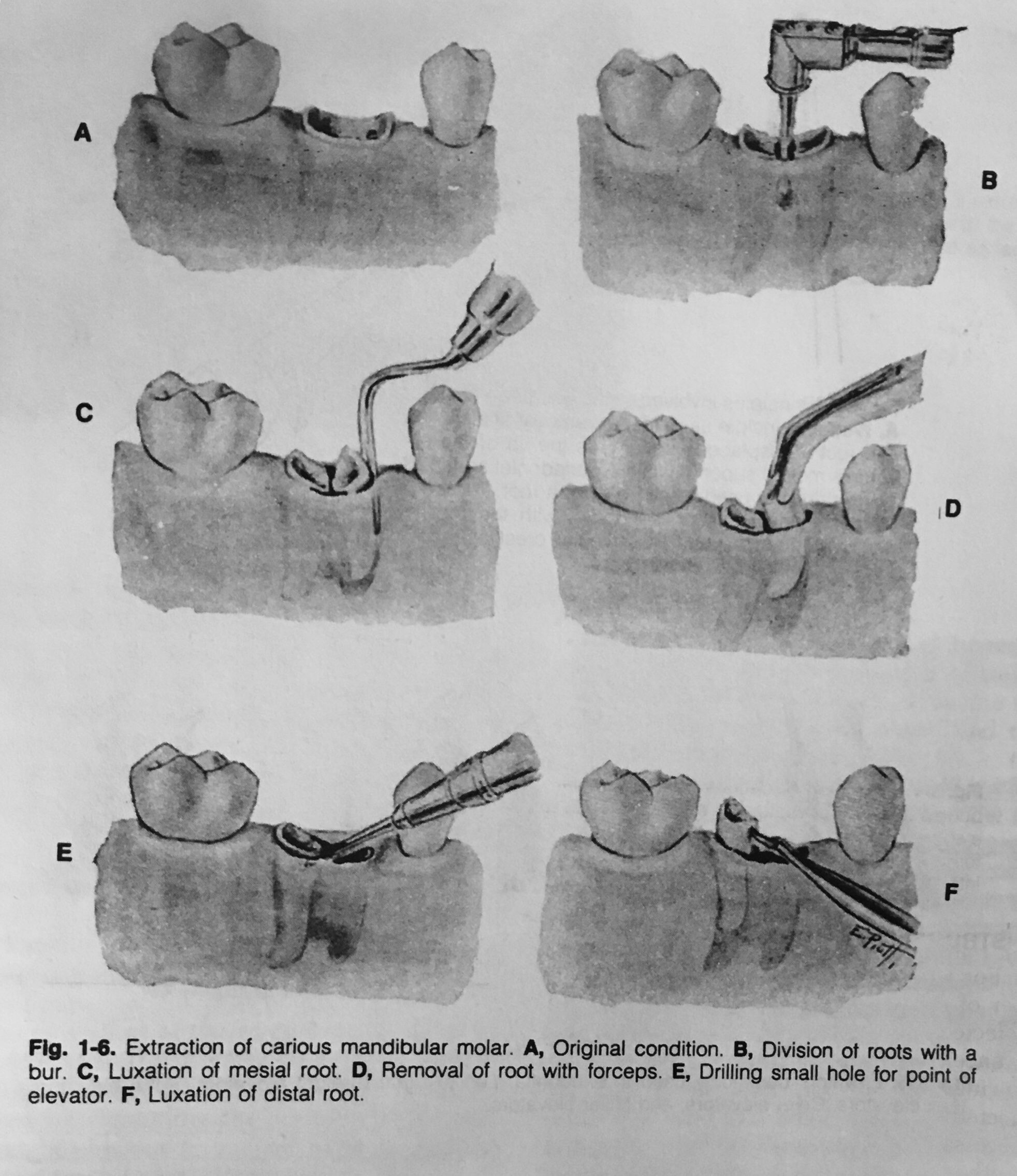

- If the roots are divergent, the bur cut, instead of being vertical, may be made parallel with one of the roots, and this part of the tooth then is extracted first.
- The other roots may be removed either with forceps or an elevator.
Dentowesome|@drmehnaz🖊
References: Textbook of Oral Surgery – Daniel M Laskin