

Source- textbook of oral pathology Shafers and Google images
Source- textbook of oral pathology Shafers and Google images
Also called as Octocephaly, Holoproscencephaly Agnathia



Source – textbook of oral pathology Shafers and Google images


General factors which would influence and tend to favour mandibular prognathism are as follows:
• Increased height of the ramus
• Increased mandibular body length
• Increased gonial angle
• Anterior positioning of the glenoid fossa
•Decreased maxillary length
• Posterior positioning of the maxilla in relation to the cranium
• Prominent chin button
•Varying soft-tissue contours
Source- textbook of oral pathology Shafers and Google images



Source- textbook of oral pathology Shafers and Google images
Reiter’s syndrome is associated with urethritis, balanitis, conjunctivitis, and mucocutaneous lesions.
It is a disease of unknown aetiology, although there is evidence of an infec- tious origin.
It is one of the most common complications of non-specific urethritis and it clinically mimicks gonorrhoea, although the urethral discharge is negative for Neisseria.

CLINICAL FEATURES
>Reiter’s syndrome is more prevalent in young adult men, usually between 20 and 30 years of age.
>The male-to-female ratio is 9:1.
>There is a typical tetrad of manifestations: non- gonococcal urethritis, arthritis, conjunctivitis, and mucocutaneous lesions.
>Urethritis may be the first sign. The urethral discharge is usually associated with itching and burning sensation.
>The arthritis is often bilaterally symmetrical and usually polyarticular.
>Conjunctivitis is often so mild as to be overlooked.
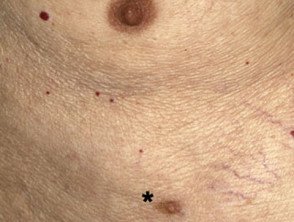
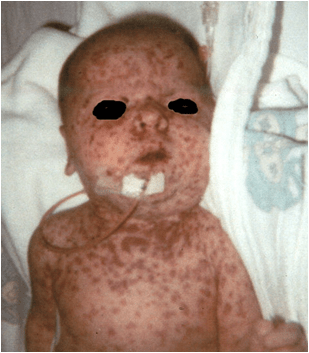
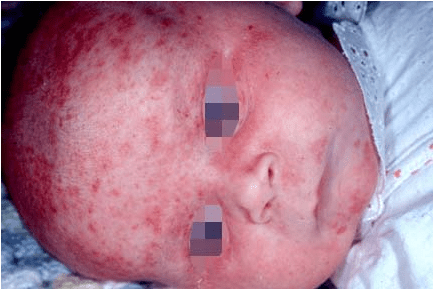
>The skin lesions are similar to those seen in keratoderma blennorrhagica and consist of red or yellow keratotic macules or papules which eventually desquamate.
Oral Manifestations
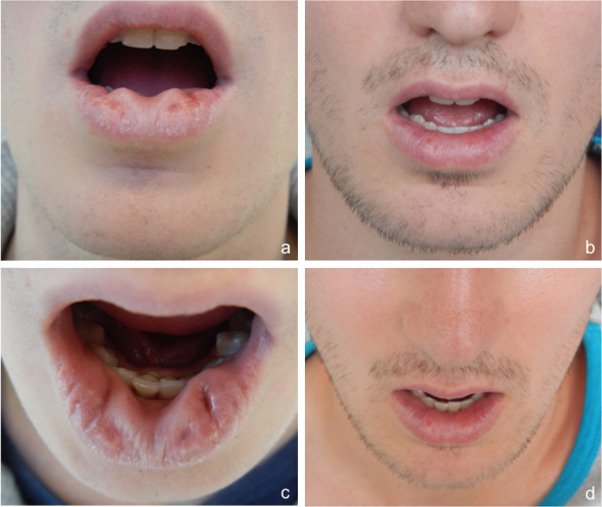
Sites—it is seen on the buccal mucosa, lips and gingiva.
Oral lesions appear as painless, red, slightly elevated areas, some- times granular or even vesicular, with a white circinate border on the buccal mucosa, lips, and gingiva.
The palatal lesions appear as small, bright red purpuric spots, which darken and coalesce, while the lesions on the tongue closely resemble ‘geographic’ tongue.

Laboratory Findings
The patients usually have a mild leukocytosis, an elevated erythrocyte sedimentation rate, and pyuria.

REFERENCE- SHAFER’S TEXTBOOK OF ORAL PATHOLOGY [8TH ED} AND ANIL GHOM TEXTBOOK OF ORAL MEDICINE




•When tooth eruption is impeded, surgical removal of the excessive tissue and exposure of the teeth are indicated.
•The cosmetic appearance may also require surgical excision.
•The lesion sometimes recurs. It has been reported that tooth extraction alone will cause the tissues to shrink almost to normal and that recurrences can be prevented by this.
Source- textbook of oral pathology Shafers and Google images




Source- textbook of oral pathology Shafers and Google images
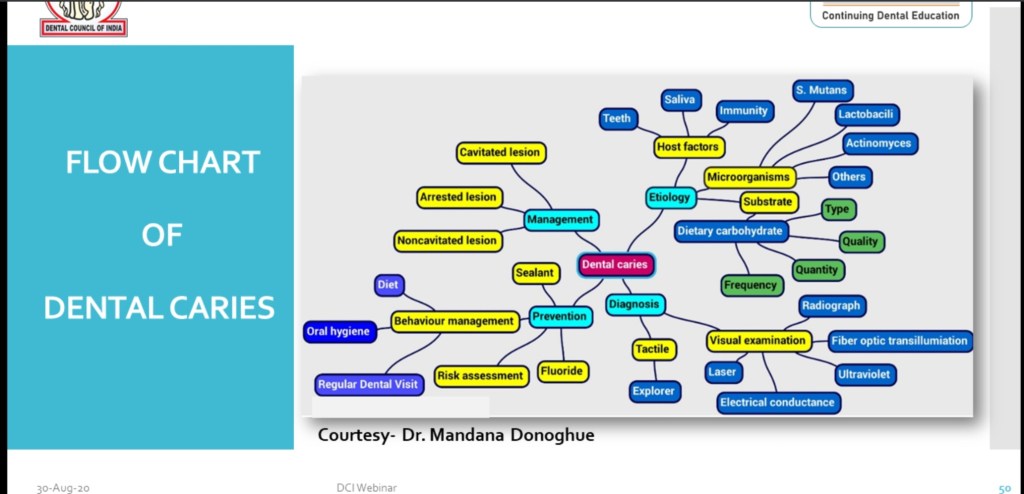
Flow Chart of Dental Caries includes:-
•Etiology
•Diagnosis
•Management
•Prevention
Source:- DCI WEBNEIR on Dental caries-30 Aug 2020.
Clinical features:-
Oral manifestations:-
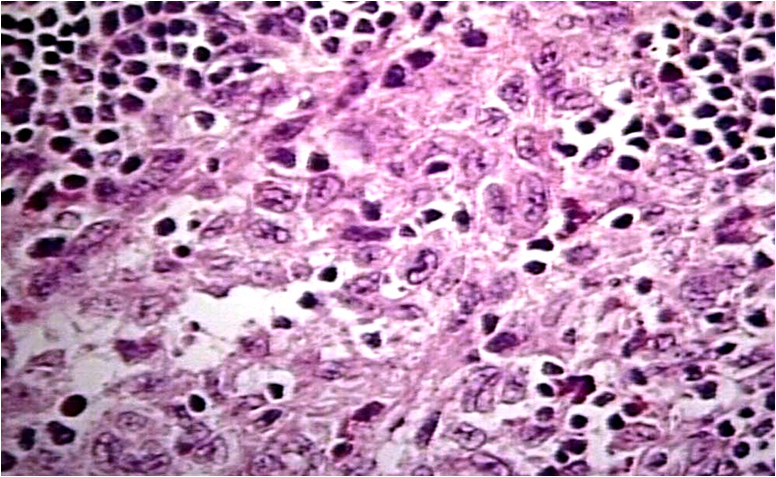
Histologic Features:-
1.Very similar to HSC; histiocytic proliferation with or without eosinophils.
2.These histiocytes do not contain significant amounts of cholesterol.
3.‘Foam cells’ not a feature.
Treatment & Prognosis:-
References:-
Shafer’s 8th edition
Clinical features:-
Oral manifestations:-

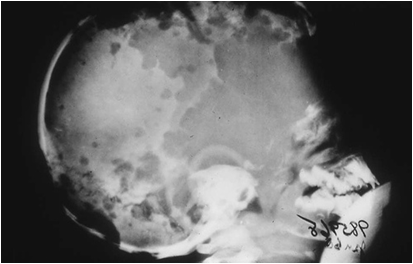
Radiological features:-


Histological features:-

Treatment & prognosis:-
Reference:
1.Faculty notes
2.Google
