





References: Essentials Of Periodontology by S Sahitya Reddy; Shafer’s Oral Pathology; Carranza’s clinical periodontology; Internet
References: Essentials Of Periodontology by S Sahitya Reddy; Shafer’s Oral Pathology; Carranza’s clinical periodontology; Internet





References: Shafer’s Textbook of Oral Pathology 7th Edition
Dr. Mehnaz Memon🖊
References: Shafer’sTextbook Of Oral Pathology




References: Shafer’sTextbook Of Oral Pathology
BY: Dr.Kriti Naja Jain :-
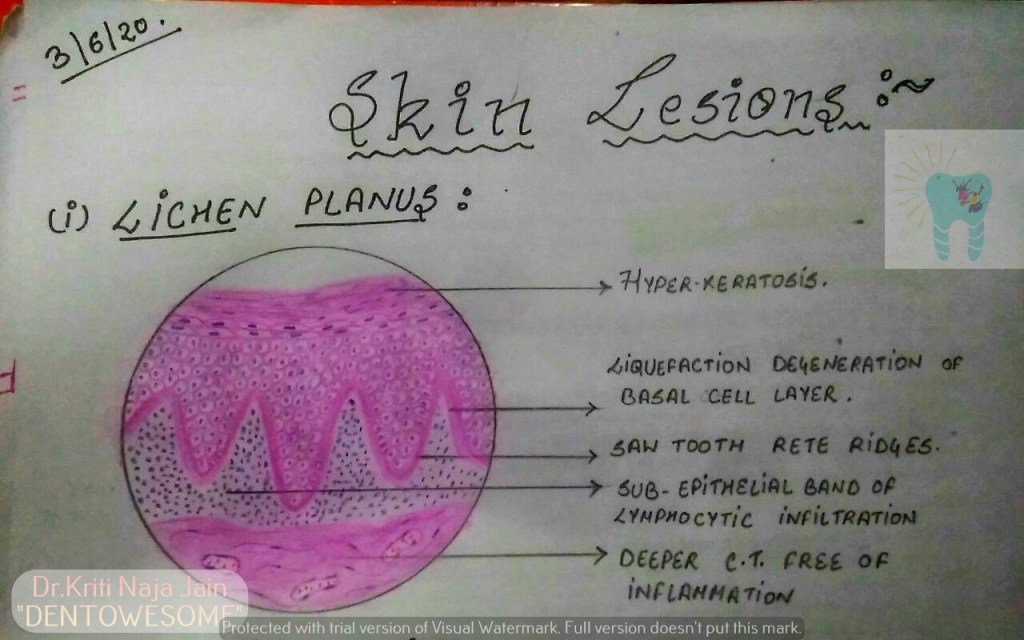
1.LICHEN PLANUS:-
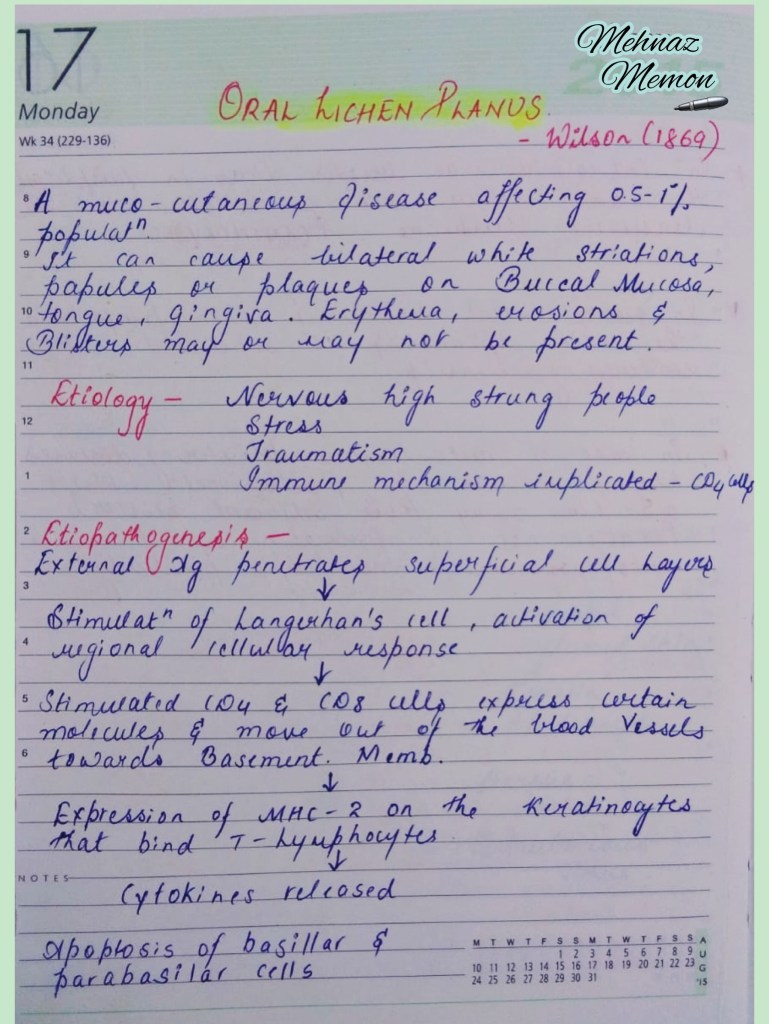
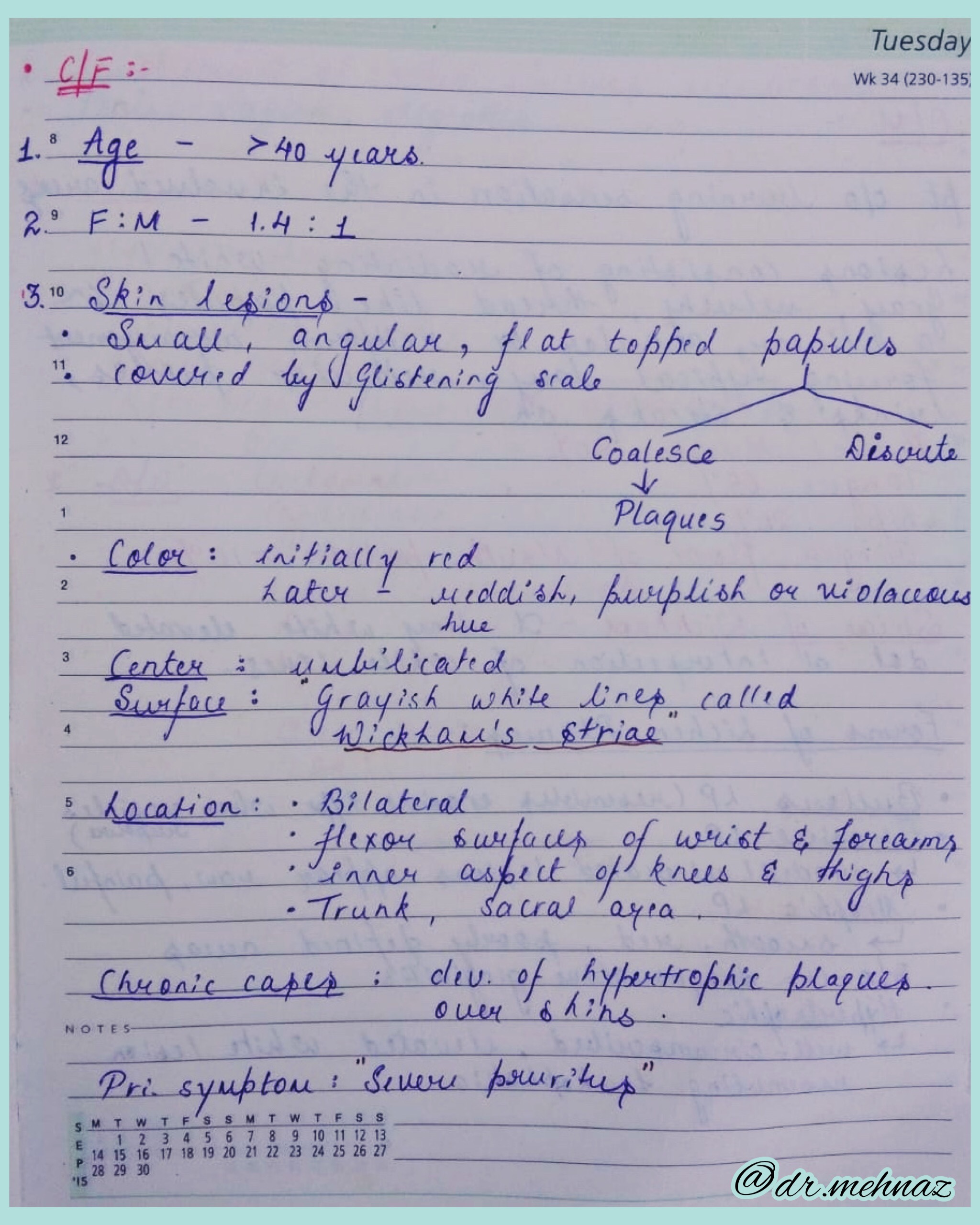
*Lichen planus is a chronic mucocutaneous disorder manifested in a various forms in the oral cavity.
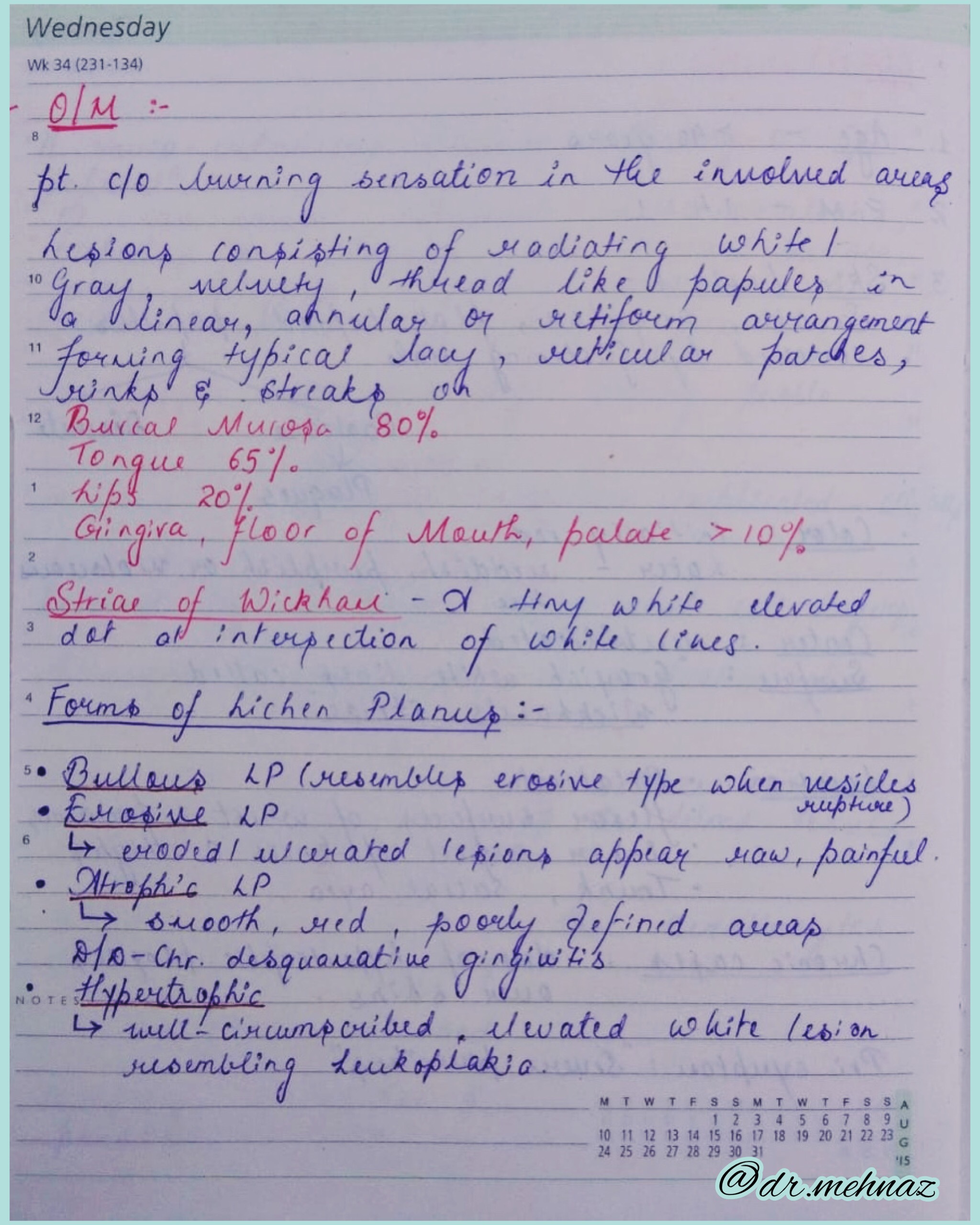
*The most characteristic pattern is” RETICULAR TYPE” with the interlacing white stripe called “WICKHAM’S STRIAE”.
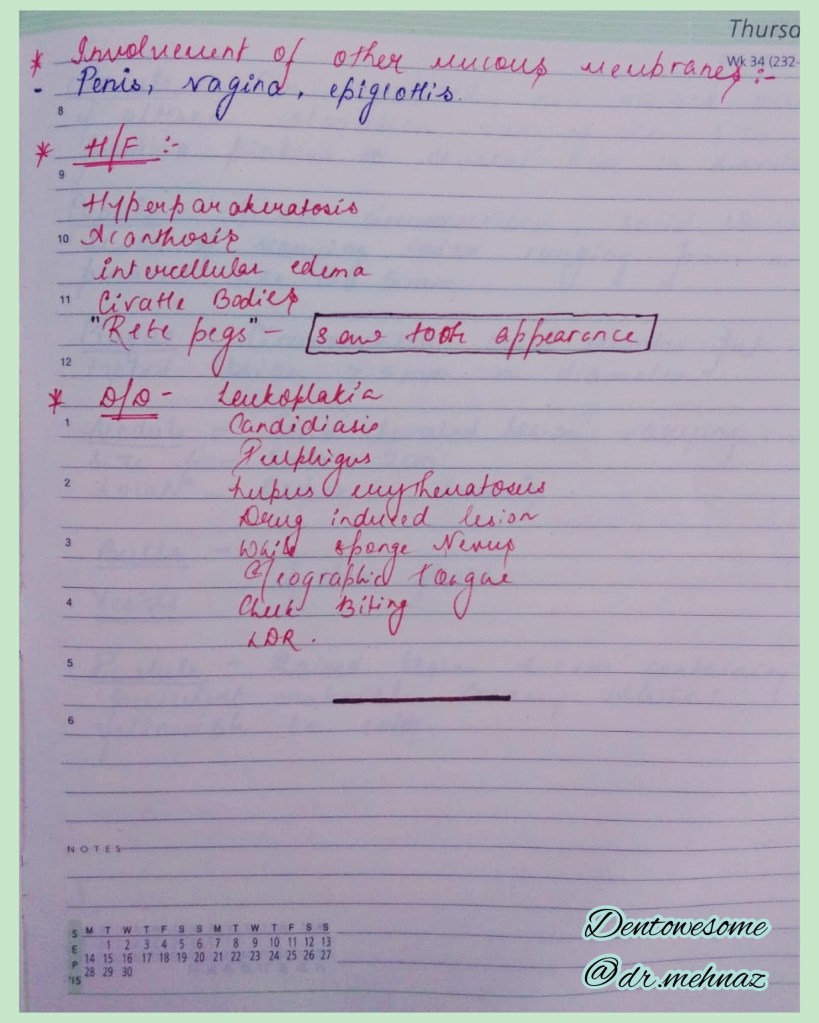
*HISTOPATHOLOGY:-

2.PEMPHIGUS :-
Pmphigus is a tissue specific autoimmune disease affecting the skin and mucosa. Clinical manifestations is in the from of “vesiculobullous lesions” that rupture to form ulcer and erosions .
*Vesiculobullous lesions develop due to immune mediated acantholysis causing intraepithelial vesicle formation.
*HISTOPATHOLOGY :-


3.PEMPHIGOID :-
Pemphigoid is a vesiculobullous lesions that develop due to an autoimmune reaction directed against some components of basement membrane.
*This results in seperation of epithelium from the connective tissue with sub epithelial vesicles formation .
*Bullous pemphigoid and cicatricial pemphigoid are two different types of pemphigoid lesions.
*HISTOPATHOLOGY:-


REFERENCE:-

source – don’t remember, had written it a lot time ago
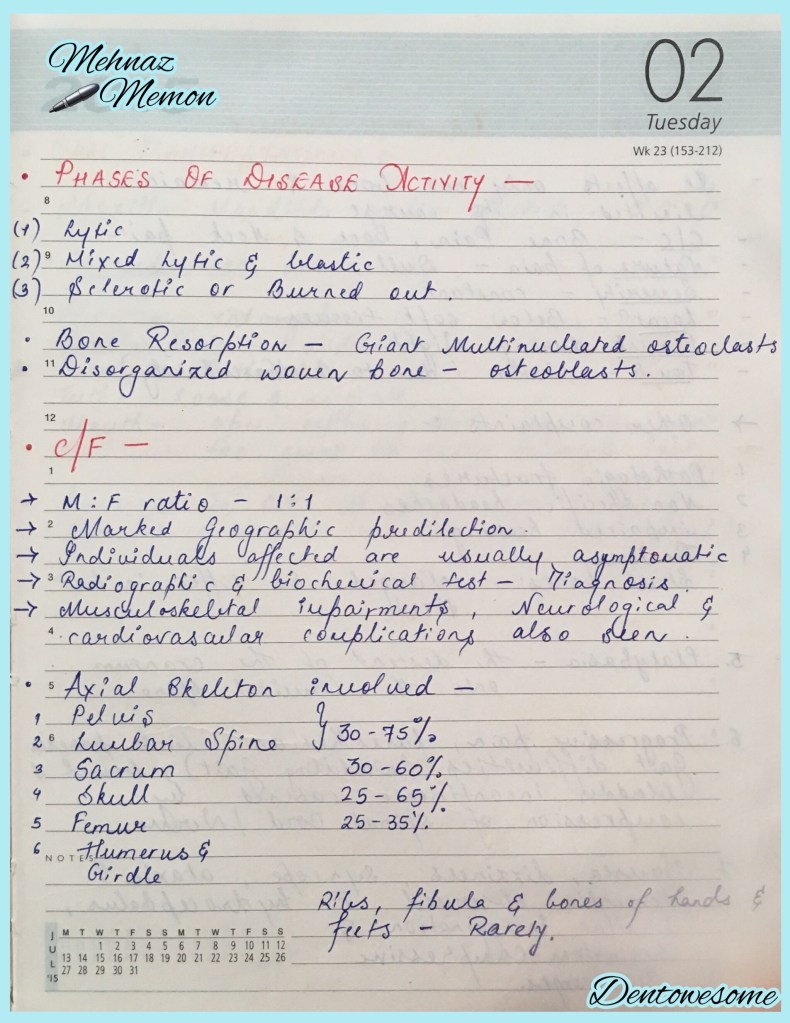
🔹Most common primary neoplasm of skeletal system.
1. Cells are closely packed in large sheets..👇🏻
2. Russell bodies: Russell bodies are multiple round cytoplasmic hyaline inclusions that are frequently seen in bone marrow aspirates in myeloma. They are composed of immunoglobulin molecules within vesicular structures derived from rough endoplasmic reticulum. Plasma cells containing them are sometimes referred to as Mott cells.
References: Shafer’sTextbook Of Oral Pathology
Dr. Mehnaz Memon🖊




source – don’t remember, had written it a lot time ago


source – don’t remember, had written it long back. , textbook – Shafers
