Understanding the growth patterns of the maxillary and mandibular lips is essential for effective orthodontic treatment planning. As orthodontic students, recognizing the interplay between facial soft tissues and the underlying hard tissues, particularly during the critical growth period from 8 to 18 years, can significantly influence treatment outcomes. This blog post delves into a lip growth and its implications for orthodontic therapy, providing data-driven insights and clinical guidelines.
Key Findings on Lip Growth
1. Maxillary Lip Length
Maxillary Lip Length Growth (mm)
Age 8
Age 18
Percentage Increase
Largest growth occurred between
Males
17.73
21.53
21.43%
Ages 10 and 16.
Females
17.73
19.88
12.11%
Ages 10 and 14.
2. Maxillary Lip Thickness
Maxillary Lip Thickness Growth (mm)
Age 8
Age 18
Percentage Increase
Males
10.77
15.76
46.33%
Growth was continuous, with the largest increase between ages 12 and 16.
Females
10.90
12.50
14.68%
Growth occurred primarily between ages 10 and 14.
3. Mandibular Lip Length
Mandibular Lip Length Growth (mm)
Age 8
Age 18
Percentage Increase
Males
19.14
26.53
38.56%
Largest increase occurred between ages 12 and 16.
Females
19.14
22.73
18.65%
Growth occurred primarily between ages 10 and 16.
4. Mandibular Lip Thickness
Males: Increased steadily from ages 8 to 16, with a plateau between ages 16 and 18.
Largest increases occurred between ages 14 and 16.
Females: Growth was less pronounced, with significant increases only between ages 10 and 14.
Clinical Implications for Orthodontic Treatment
1. Sexual Dimorphism in Lip Growth
Males experience greater increases in both lip length and thickness compared to females.
Females show more limited growth, particularly in lip thickness during puberty.
2. Extraction Therapy Considerations
Female Patients: Limited lip thickening during puberty makes the effects of extraction therapy more noticeable, especially in patients with straight or concave profiles. Treatment plans should be approached with caution to avoid adverse effects on facial esthetics.
Male Patients: Greater lip thickening provides more flexibility for extractions without significantly impacting facial profile fullness.
Maxillary Lip Thickness Growth Rates
Males:
0.5 mm/year (ages 8–12).
0.7 mm/year (ages 12–16).
Females:
0.5 mm/year (ages 10–12).
0.3 mm/year (ages 12–14).
Conclusion
Understanding the growth patterns of maxillary and mandibular lips is essential for predicting soft-tissue responses and planning effective orthodontic treatments. Sexual dimorphism plays a significant role, with males experiencing greater growth in both lip length and thickness compared to females. These differences must be factored into treatment decisions, particularly for extraction therapy, to ensure optimal esthetic and functional outcomes. As orthodontic students, incorporating these insights into clinical practice will enhance your ability to deliver patient-centered care.
Palatal expansion has been a cornerstone of orthodontic treatment for over a century. Despite its proven efficacy, this technique has sparked debates within the orthodontic community. Is rapid expansion the best approach, or do slower methods offer greater stability? Let’s dive into the history, mechanics, and clinical applications of maxillary expansion, with a special focus on the quad-helix appliance.
The primary goal of palatal expansion is to coordinate the maxillary and mandibular denture bases, addressing narrow or collapsed arches. This can be achieved through:
Orthodontic Movement (tooth-focused)
Orthopedic Movement (bone-focused)
Combination Therapy
A variety of appliances—fixed, semi-fixed, and removable—are employed to achieve these goals.
Method
Advantages
Challenges
Rapid Palatal Expansion
Quick skeletal changes
Potential for relapse and sutural strain
Slow Expansion
Greater histologic integrity of sutures
Requires longer treatment time
HISTORY
Coffin Loop Appliance:
Incorporated in a vulcanite plate for upper arch expansion.
Produces continuous force due to the configuration of the palatal compound loop.
Martin Schwarz Appliance:
Popular in Europe.
Utilizes tissue-borne anchorage with wire components for tooth movement.
Expansion force is intermittent due to the jackscrew mechanism.
Haas and Wertz Fixed Appliance:
Designed for rapid expansion of the midpalatal suture in narrow maxillary arches.
Cemented to maxillary first premolars and first permanent molars.
Includes a palatal jackscrew and acrylic extensions.
Produces lateral orthopedic movement of the maxilla due to high force magnitude.
Load-Activation Characteristics:
Chaconas and Caputo found differences in stress transmission through craniofacial bones with various fixed expansion appliances.
Impact on craniofacial sutures varies depending on the appliance.
Rickett’s “W” Expansion Appliance:
Initially used for cleft palate conditions with collapsed dental arches.
Acts continuously over time until activation force dissipates.
What Makes the Quad-Helix Appliance Unique?
Helical Loops for Increased Flexibility:
Initially added to the posterior segment of the palatal arch
Further modification introduced four loops (two anterior and two posterior), creating the quad-helix appliance.
Construction Details:
Made of 0.038-inch (0.975 mm) wire.
Soldered to bands cemented to maxillary first permanent molars or deciduous second molars, depending on the patient’s age.
Initial Activation and Effects:
Appliance is activated before cementation.
Results in expansion of buccal segments and rotation of banded teeth
Force Magnitude:
Chaconas and Caputo reported that 8 mm of expansion before cementation generates approximately 14 ounces of force
Effectiveness in Different Age Groups:
Effective in orthopedically widening the maxilla in children, helping to establish a normal maxillomandibular relationship.
Force is sufficient for tooth movement but insufficient for orthopedic effects in adults with closed midpalatal sutures.
In children, particularly in the deciduous or early mixed dentition stages, the resistance of the patent suture is lower than the dentoalveolar area.
Clinical Case: A Pediatric Success Story
Patient History: Prolonged thumb-sucking led to a narrow maxilla due to lowered tongue position and buccinator muscle forces.
Treatment: Quad-helix appliance activated ~8 mm, sufficient for maxillary expansion.
Outcome: Successful expansion and resolution of thumb-sucking habit. The appliance’s palatal position ensured comfort and minimal impact on speech.
Maxillary Molar Width: Increased by an average of 5.88 mm, reflecting significant dental expansion.
Average Frontal Molar Relation: Improved by 2.95 mm, indicating better occlusal alignment.
Maxillary Intercanine Width: Expanded by 2.74 mm, enhancing anterior dental arch form.
Orthopedic Changes (T₁ to Tₚ)
Maxillary Width: Increased by 0.92 mm, with five cases showing expansions exceeding 2.7 mm.
Maxillomandibular Width: Increased by 0.89 mm, with notable cases surpassing 1.4 mm.
Palatal Changes: The anterior palate moved downward, increasing maxillary height.
Relapse and Stability (Tₚ to T₂)
Minimal Relapse: Dental expansions remained stable over 42 months.
Orthopedic Effects: Demonstrated high stability, contrasting with the relapse often seen in rapid palatal expansion.
Palatal Plane and Maxillary Height: Slight decreases observed, indicating no net parallel downward movement.
Slow vs. Rapid Expansion
Slow expansion using the quad-helix appliance demonstrated superior stability and less relapse compared to rapid palatal expansion. The gradual physiologic movement allowed the facial skeleton to adapt, ensuring long-term stability.
Bite Opening
Active Expansion (T₁ to Tₚ): Slight bite opening occurred due to occlusal interferences.
Post-Expansion (Tₚ to T₂): Additional bite opening was attributed to orthodontic treatment rather than the expansion appliance.
Facial Skeletal Considerations
Stability was influenced by initial nasal and maxillary widths:
Narrow Maxilla + Normal/Wide Nasal Width: High stability.
Narrow Nasal Width + Normal Maxilla: Lower stability.
Facial Type
The sample skewed toward brachyfacial types, limiting conclusions about expansion outcomes across facial types.
Introduction Malocclusion, characterized by changes in teeth positioning and skeletal growth, represents a global public health concern.
Historical Context: Correction attempts date back to at least 1000 BC.
Prevalence: Class II malocclusion affects one-third of the population and is categorized as skeletal or dental in origin.
Etiology:
Only 20% of Class II Division 1 cases are due to maxillary protrusion.
The majority stem from mandibular retrusion.
This prevalence has led to the development of functional appliances aimed at stimulating mandibular growth. These devices are divided into removable and fixed functional appliances.
Fixed Functional Appliances
Types:
Rigid: Herbst appliance, MARA (Mandibular Advancement Repositioning Appliance).
Flexible: Jasper Jumper, Scandee tubular jumpers.
Hybrid: Forsus Fatigue Resistant Device (FFRD).
Forsus Fatigue Resistant Device (FFRD):
A telescoping spring mechanism for Class II correction.
Provides moderate patient tolerance with initial discomfort that subsides over time.
PowerScope Appliance:
Latest addition, introduced by Dr. Andy Hayes in 2016 in collaboration with American Orthodontics.
Features a telescopic mechanism with a nickel-titanium (NiTi) spring delivering 260 g constant force.
Designed as a preassembled, one-size-fits-all appliance for easy chairside application.
Study Rationale While Forsus FRD is extensively studied, limited literature evaluates and compares the skeletal, dental, and soft tissue effects of PowerScope. This study bridges that gap by conducting a cephalometric evaluation and comparison of these two fixed functional appliances.
Both appliances are effective in correcting Class II discrepancies caused by retrognathic mandibles. However:
Forsus FRD is superior in achieving skeletal changes, particularly maxillary retrusion and mandibular advancement.
PowerScope shows more pronounced effects on dentoalveolar and soft tissue parameters, especially upper incisor inclination correction and facial convexity improvement.
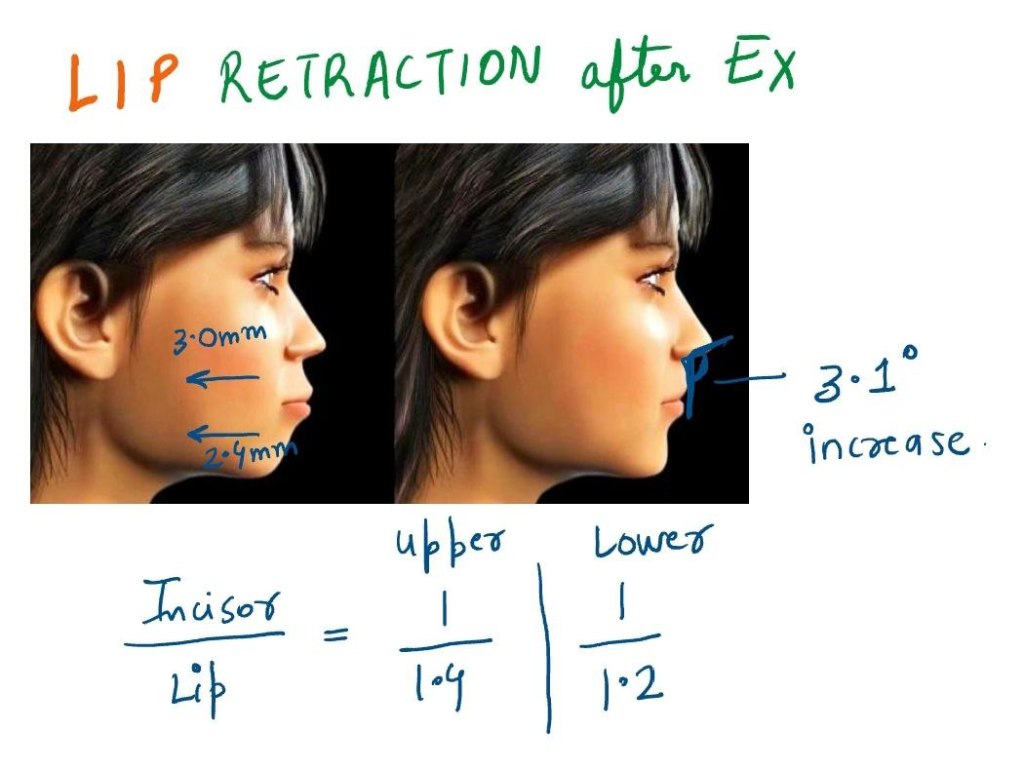
Bimaxillary protrusion is a common orthodontic condition marked by protrusive and proclined upper and lower incisors, coupled with increased lip prominence. While predominantly seen in African American and Asian populations, it is not limited to any single ethnic group. This condition often leads patients to seek orthodontic treatment due to the aesthetic concerns of protruding lips and dentition.
Soft Tissue and Hard Tissue Correlation
Orthodontic studies present two conflicting perspectives on the relationship between incisor retraction and lip position:
Strong Correlation: Some studies demonstrate a direct relationship between incisor and lip retraction.
Weak Correlation: Some studies suggest that soft tissue changes do not proportionally mirror dental movements due to variables like growth, lip tonicity, and anchorage.
Four retrospective studies on bimaxillary protrusion treatment provided valuable insights:
Study Findings
Upper Lip Retraction (mm)
Lower Lip Retraction (mm)
Nasolabial Angle Increase (°)
Caplan et al. (2009)
3.0
2.4
Not significant
Tan et al.
2.7
2.0
10.5
Lew
3.2
4.5
10.0
Bills et al.
3.0
2.4
3.1
Incisor Retraction and Lip Retraction Ratios
Study
Upper Lip to Incisor Retraction
Lower Lip to Incisor Retraction
Caplan et al.
1:1.4
1:1.2
Other Studies
1:2.2
1:1.75
Clinical Implications
Four-premolar extractions effectively reduce lip procumbency in bimaxillary protrusion.
Nasolabial angle tends to increase post-treatment.
Molar distalization is a crucial technique in orthodontics, particularly for patients with Class II malocclusion. Thanks to advancements in biomechanics, materials, and technology, orthodontists now have access to a variety of intramaxillary intraoral appliances that can apply light, continuous forces for effective molar distalization. These appliances have become a game-changer, providing us with more precise control and predictable results.
Types of Intramaxillary Appliances
The application of forces in molar distalization can come from two primary areas: the buccal or the palatal region. Depending on where the force is applied, appliances can be categorized into two broad groups:
Buccal Force Application: These appliances apply force from the outside of the dental arch.
Palatal Force Application: These appliances exert force from the roof of the mouth.
Additionally, the force mechanisms can be divided into two categories:
Friction-Free Mechanism: This type involves appliances like the pendulum, which are designed to move the molars without causing significant friction.
Sliding Mechanism: Appliances like nickel-titanium (NiTi) coil springs use a sliding mechanism to apply force, creating a more dynamic force delivery system.
Each of these appliance types has its own set of advantages and drawbacks, and comparing their efficiency in achieving molar distalization is key to making evidence-based treatment decisions. However, due to the limited number of randomized clinical trials, a meta-analysis is often not possible. That said, a comprehensive analysis of existing studies can still offer valuable insights into how these appliances work.
Treatment Outcomes: Overall Effects
When all intramaxillary appliances were considered together, some general findings emerged:
First Molar Movement: On average, first molars moved 2.9 mm distally, but this came with a 5.4° of distal tipping.
Incisor Movement: The incisors shifted mesially by 1.8 mm with 3.6° of mesial tipping.
Premolar Movement: Premolars showed a mesial shift of 1.7 mm, though tipping was less pronounced.
Vertical movements were generally extrusive for incisors and premolars, with incisors showing an average extrusion of 0.4 mm and premolars 1.1 mm. Interestingly, molar vertical movements were not statistically significant, indicating that the main effect on molars was distal movement and tipping rather than vertical displacement.
Treatment Effects: Buccal vs. Palatal Appliances
Now, let’s delve into the specific effects of buccal and palatal appliances. These results highlight the different ways these appliances move teeth:
Buccal Appliances:
Molar Movement: Molar distal movement was 2.6 mm, with a more significant tipping of 8.3°.
Incisor Movement: Incisors moved mesially by 1.9 mm with 5.0° of mesial tipping.
Premolar Movement: Premolars demonstrated a 2.0 mm mesial shift, accompanied by 7.0° of mesial tipping.
Vertical Movement: Premolars showed a slight extrusion of 0.7 mm, while incisors had a more modest extrusion of 0.2 mm.
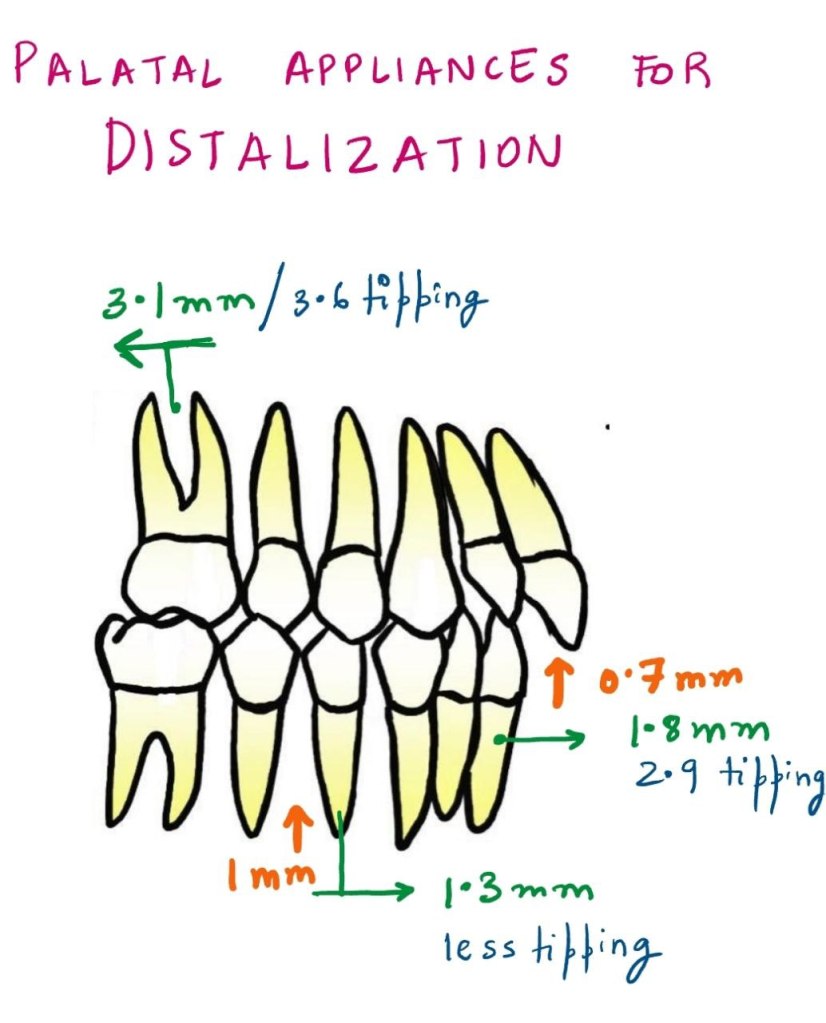
Palatal Appliances:
Molar Movement: Molar distalization was slightly more pronounced, with 3.1 mm of movement and 3.6° of tipping.
Incisor Movement: Incisors exhibited a mesial shift of 1.8 mm with 2.9° of mesial tipping.
Premolar Movement: Premolars moved mesially by 1.3 mm with less tipping than buccal appliances.
Vertical Movement: The extrusion for incisors was 0.7 mm, and premolars showed an extrusion of 1.0 mm.
Molar Distalization and Anchorage Loss
The primary effect of noncompliance intramaxillary appliances is molar distalization, which is typically achieved through a combination of crown distal movement and tipping. While distalization is the goal, a common side effect observed is loss of anchorage. This loss can be seen in the mesial movements and extrusions of incisors and premolars.
Key Findings:
Molars: Show a combination of distal crown movement and distal tipping.
Incisors: Exhibit mesial movement, tipping, and extrusion.
Premolars: Display mesial crown movement and extrusion.
As with any treatment modality, careful planning is required to manage these unintended side effects and achieve the best possible clinical outcomes.
Buccal vs. Palatal Appliances: Tipping and Force Mechanics
One interesting observation in the study was the difference in tipping effects between buccal and palatal acting appliances. Palatal appliances consistently resulted in less tipping of teeth compared to buccal appliances, as indicated by the non-overlapping confidence intervals.
Why the Difference?
The key reason for this difference lies in the moment arm of the force. In palatal appliances, the line of action of the force is closer to the center of resistance of the tooth, leading to less tipping and more controlled molar movement.
Table 1: Comparison of Tipping between Buccal and Palatal Appliances
Appliance Type
Molars Distal Movement (mm)
Molars Tipping (°)
Incisor Mesial Movement (mm)
Incisor Tipping (°)
Premolar Mesial Movement (mm)
Premolar Tipping (°)
Buccal Appliances
2.6
8.3
1.9
5.0
2.0
7.0
Palatal Appliances
3.1
3.6
1.8
2.9
1.3
3.0
This table highlights the greater tipping observed with buccal appliances compared to palatal appliances, as well as the differences in molar distalization and mesial movement of incisors and premolars.
The Nance Button: Anchorage Considerations
Another point of discussion is the use of the Nance button to reinforce anterior anchorage during molar distalization. While it can support anchorage to some extent, it does not provide absolute anchorage. This is because the Nance button, as part of the anchorage unit, cannot completely resist mesial forces during molar distalization. Clinically, this often results in an increased overjet and proclination of maxillary incisors.
Clinical Tip:
For patients already presenting with an increased overjet, orthodontists must proceed with caution when prescribing these appliances. These cases may require additional measures to control the overjet and manage incisor proclination.
The Pendulum Appliance: A Look at Tipping and Movement
The pendulum appliance, a popular friction-free appliance, was noted in the study to cause the greatest distal tipping of molars. However, this tipping was correlated with a larger amount of distal crown movement. Interestingly, this tipping can often be corrected with the use of molar uprighting bends.
Table 2: Molar Distalization and Tipping with the Pendulum Appliance
Movement Type
Molar Distal Movement (mm)
Molar Tipping (°)
Pendulum Appliance
3.4
9.0
This table shows that the pendulum appliance can achieve significant molar distalization but at the cost of increased tipping. These tipping movements can be addressed with molar uprighting bends, which can help reduce the tipping angle.
Factors Affecting Molar Distalization
Several factors can influence the effectiveness of molar distalization, including:
Teeth Used for Anchorage: Different anchorage setups can affect the extent of distal movement.
The Type of Appliance Used: Whether the appliance uses a sliding mechanism or a friction-free mechanism plays a role.
Patient Factors: Age, initial molar relationships, and the eruption of second and third molars all contribute to how effectively molars are distalized.
In studies that focus on growing patients, mean ages ranged from 11.2 to 14.9 years, which is crucial because the growth phase can significantly impact the effectiveness of treatment. For example, molar distalization is often more effective before the second molars have erupted. When second molars are erupted, more force may be required, and the treatment time may increase.
Table 3: Influence of Molar Eruption on Distalization Efficiency
So you’ve got the braces thing going on, huh? A journey to a stellar smile, no doubt! But let’s face it, chomping down on everything from apples to samosas can be a real drag with those metal friends attached. Fear not, fellow food enthusiasts, for this guide will turn you into a braces-wearing, balanced-diet boss!
Carbs: Your Chapatti and Rice BFFs
Lucky you! Most grains are soft and chew-friendly. Pile on the fluffy rice, indulge in those melt-in-your-mouth rotis (dunk ’em in dal for extra protein power!), and enjoy that breakfast bread (just maybe avoid the rock-hard baguettes for now). Discomfort? Mash those chapattis into a delightful curry and rice symphony – your taste buds and braces will thank you.
Dairy: Your Calcium Cavalry
Milk, yogurt, cheese – the holy trinity of strong teeth and happy braces! They’re soft, delicious, and pack a calcium punch. Bonus points for milkshakes (because, hello, who doesn’t love a good milkshake?), but go easy on the sugar. Think of yourself as a calcium crusader, venturing forth with every spoonful of yogurt!
Veggies: Your Mashed Marvels
Ah, vegetables – the dietary champions! Most Indian meals involve cooked veggies, which are a breeze for braces. Feeling a bit adventurous? Mash them up for extra comfort. Need a raw veggie fix? Grate those carrots or chop your salad into bite-sized pieces. Just remember, you’re not a superhero (yet!), so skip the superhero-sized bites.
Fruits: Your Juicy Jewels (with a Few Caveats)
Fruits – the colorful crew that adds sweetness to life! But with braces, things can get a little tricky. Apples? Unless you’re feeling like a dental daredevil, cut them up. Unripe pears and peaches? Give them a side-eye. Feeling extra tender after a wire change? Citrus fruits and berries are your new best friends. Remember, if all else fails, fruit juice is always a healthy option. Just a heads-up, though, chomping on icy-cold fruits might not be the most pleasant experience with all that metal in your mouth. Let your food warm up a bit for a friendlier feast.
Nuts & Seeds: Your Sneaky Saboteurs (But We Can Work With Them)
Okay, nuts and seeds – they’re delicious, nutritious, but a real challenge for braces. Here’s the deal: during your orthodontic adventure, swap those whole nuts for nut butters (think creamy peanut butter heaven!) or coarsely grind your favorite seeds. This way, you get the goodness without the potential for a braces breakdown.
Meat: Your Tender and Chopped Champs
Meat – the protein powerhouse! Unfortunately, it can be a bit fibrous and tough on braces. Here’s the golden rule: avoid gnawing on meat straight off the bone (think of your teeth, not your inner caveman). Tofu and cottage cheese are great protein alternatives, but if you must have meat, choose lean, tender cuts and chop them into bite-sized pieces.
The Absolute No-Nos: Your Braces’ Nightmares
Now, let’s talk about the foods that would make your braces weep. Gum (both sugary and sugarless) is a big no-no. Sticky candies? Forget about it. Hard foods like whole nuts (unless grinded), popcorn, corn on the cob, pizza crusts (sorry!), ice, and cookies are strictly off-limits. Think of them as villains in your quest for a perfect smile.
Remember: Consistency is key! Stick to this guide, embrace some creativity in the kitchen, and you’ll be a braces-wearing, balanced-diet pro in no time. Now go forth and conquer that delicious, nutritious world, one bite at a time (and maybe cut that bite in half)!