Dr. Mehnaz Memon🖊
Dentowesome 2020
References: Davidson’s Principles and Practice of Medicine Textbook





Dr. Mehnaz Memon🖊
Dentowesome 2020
References: Davidson’s Principles and Practice of Medicine Textbook

(A)
(B)
5. Regular exercise: Jogging & swimming – ⬇️ Arterial pressure
• Objectives
🔅 To reduce the incidence of adverse cardiovascular events viz coronary heart disease, stroke & heart failure
• Benefits:
🔅Diuretics or β blockers have shown to reduce the risk of
🔅Most of the excess Morbidity & Mortality associated with HT is attributable to CAD. Total CVR = CAD risk x 4/3
🔅 Hypertension in old age:
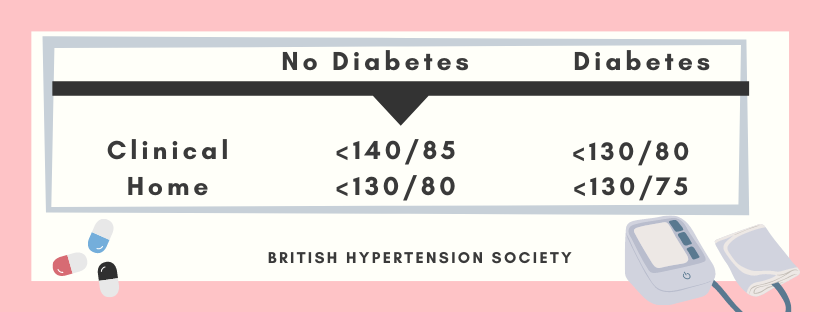
Target BP during AHT



A. ACE Inhibitors:
👉🏻Patients with renal artery stenosis/impaired Renal function (given with utmost care)
⬇️
Reduction of filteration pressure in the glomeruli
⬇️
Renal failure
👉🏻These agents also reduce the progression of Nephropathy in type II diabetes
👉🏻Level of electrolytes & creatinine should be checked before & after 1-2 weeks.
B. ARB’s
👉🏻Have lesser side effects of cough & angioedema than ACE inhibitors
C. Beta-blockers:
👉🏻These drugs are not used now as first line AHT; except in patient with Angina
👉🏻Labetalol & Carvedilol: Have better effect when combined. Labetalol is used as infusion in malignant phase HT.

D. CCB’s
👉🏻The dihydropyridines are effective, well-tolerated particularly in older people
👉🏻Rate–limiting CCB’s: HT with angina. Bradycardia may occur
E. Thiazides & other Diuretics:
👉🏻The loop diuretics have few A/D over thiazides unless there’s renal impairment.

Chart showing Mode of Action & Side effects of AHT’s☝🏻

The influence of comorbidity on the choice of antihypertensive drug therapy

Management of hypertension: British hypertension society guidelines
Criteria:
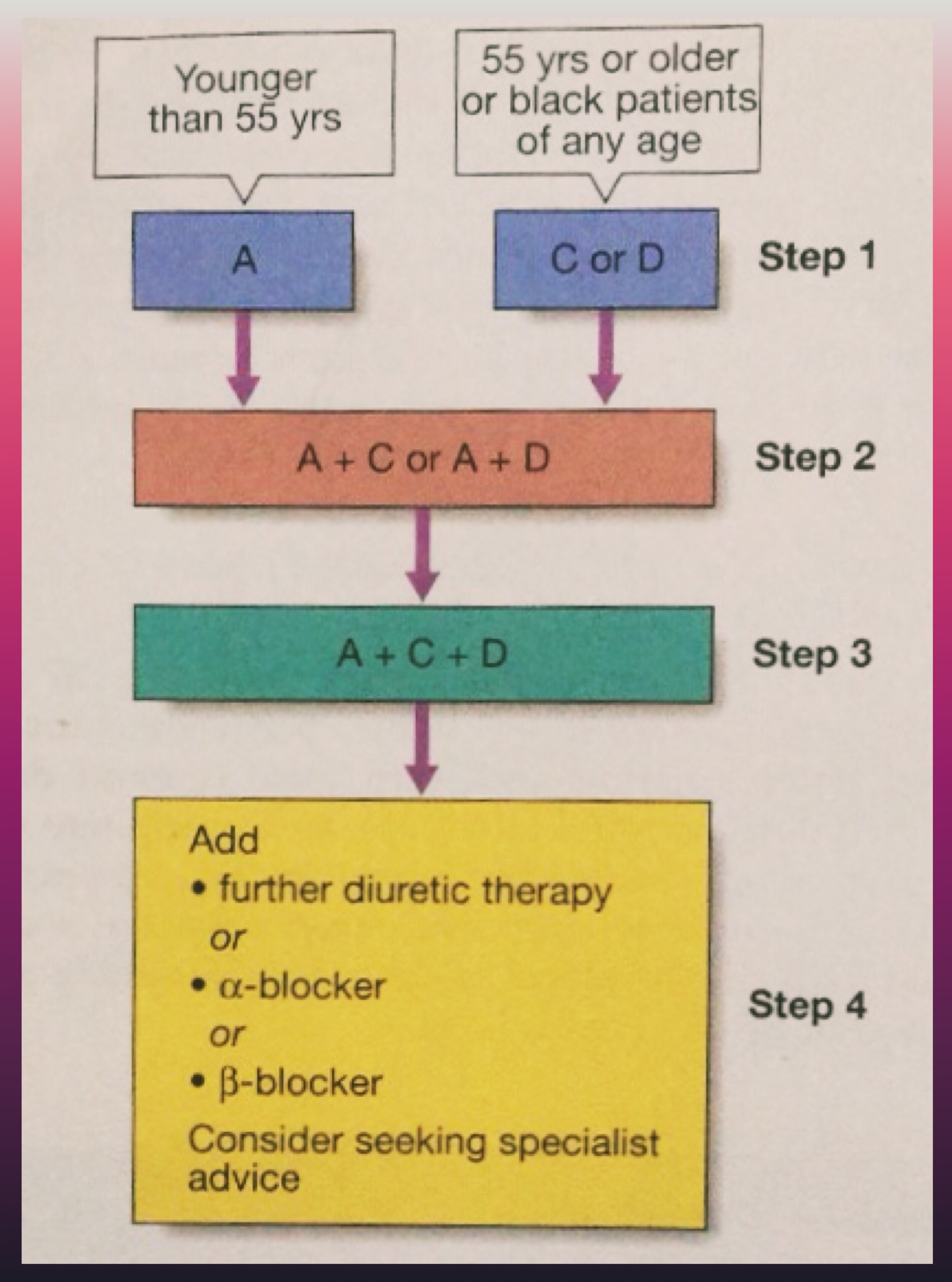
A = ACE inhibitor (consider AT-II receptor antagonist if ACE-intolerant); C = Calcium channel blocker; D = thiazide-type diuretic)
🔅 In accelerated phase HT, lowering BP too quickly may compromise tissue perfusion & can cause –
🔅150/90 mm Hg within 48 hours is ideal along with cardiac failure/hypertensive encephalopathy
🔅Avoid parenteral therapy
🔅Causes of treatment failure include:
📌Aspirin – Antiplatelet
📌Statins – Reduced risk by treating hyperlipidaemia
Dr. Mehnaz Memon🖊
References: Davidson’s Principles and Practice of Medicine Textbook
Tap to View in full size…⬇️
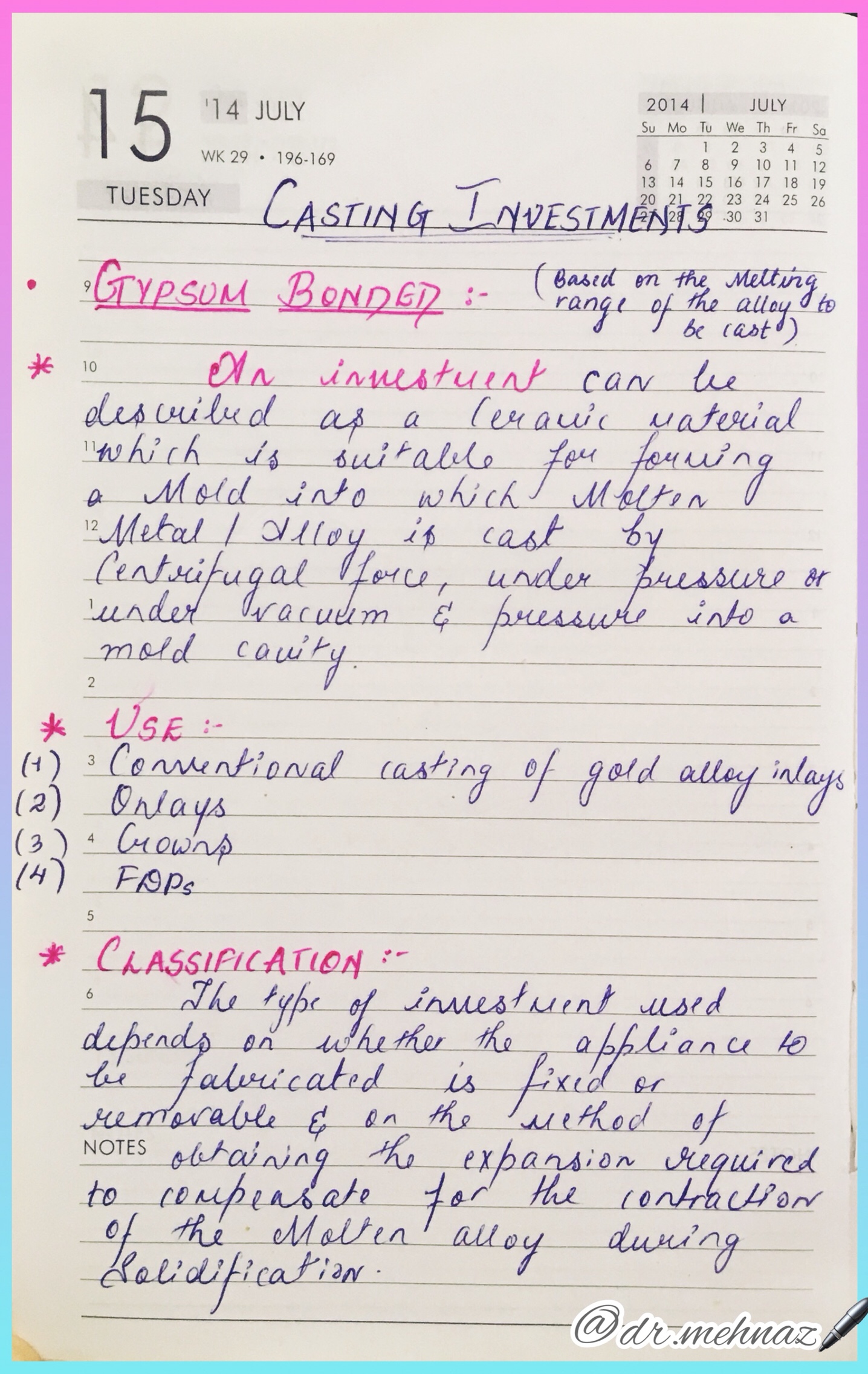
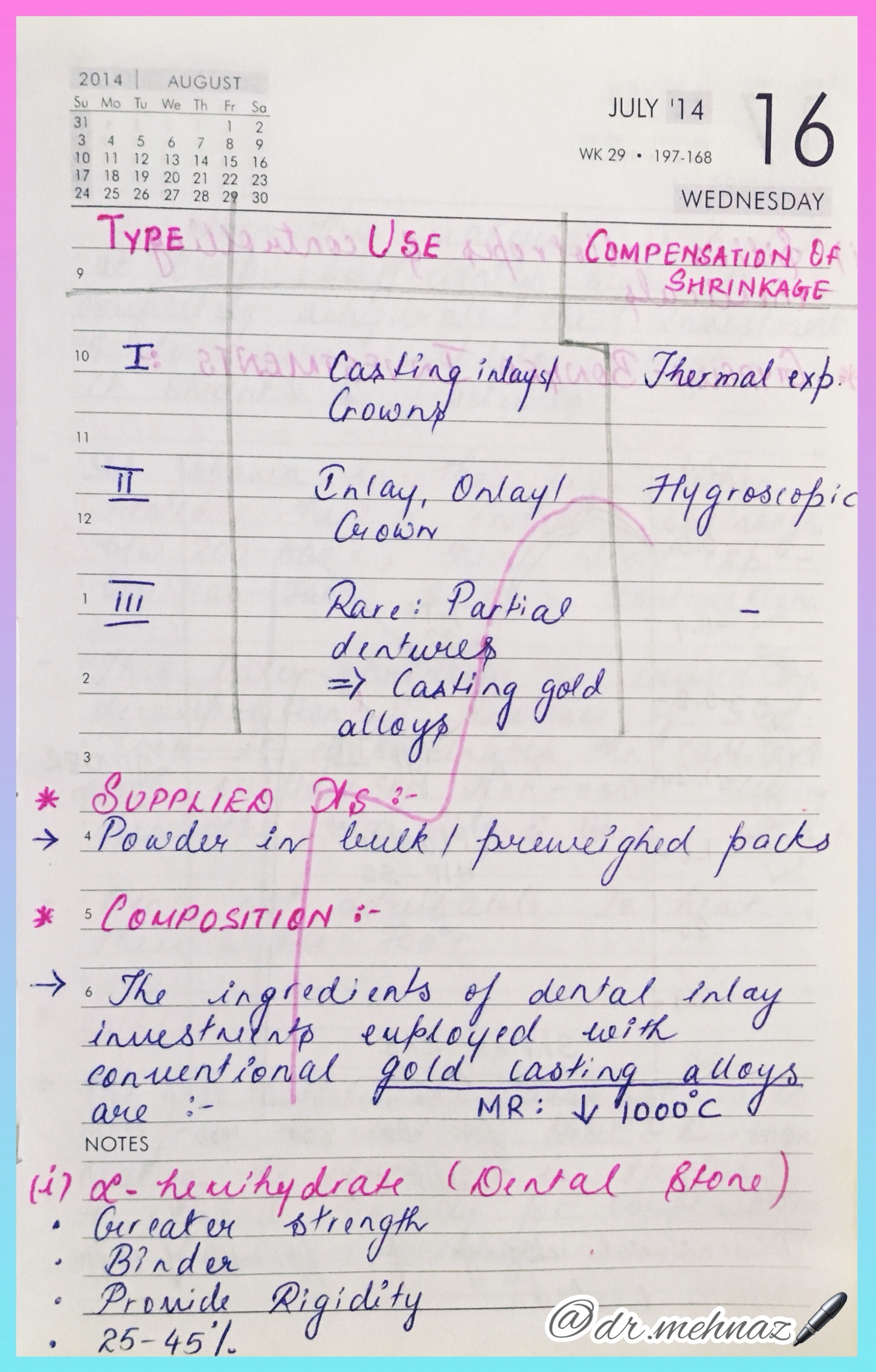


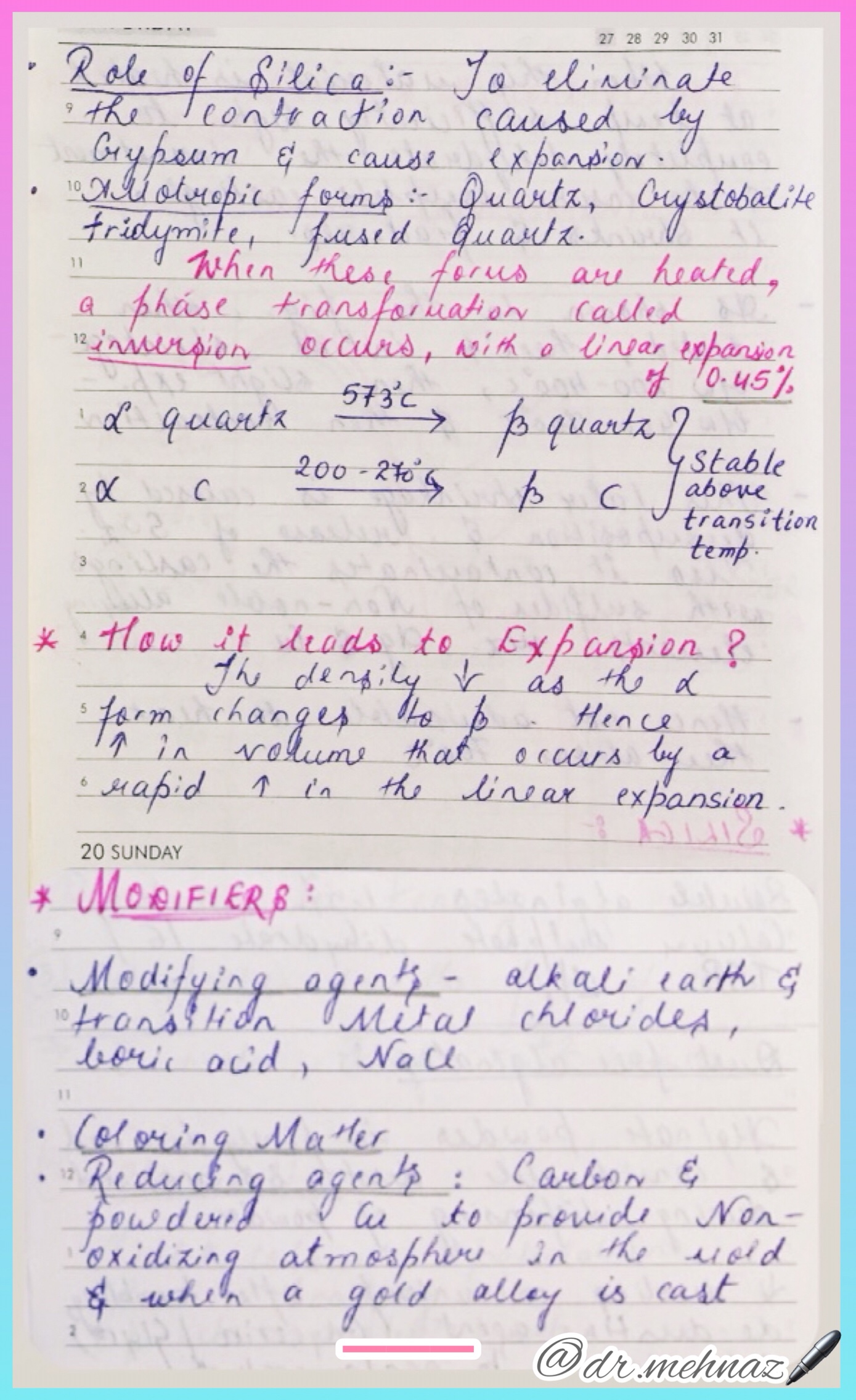
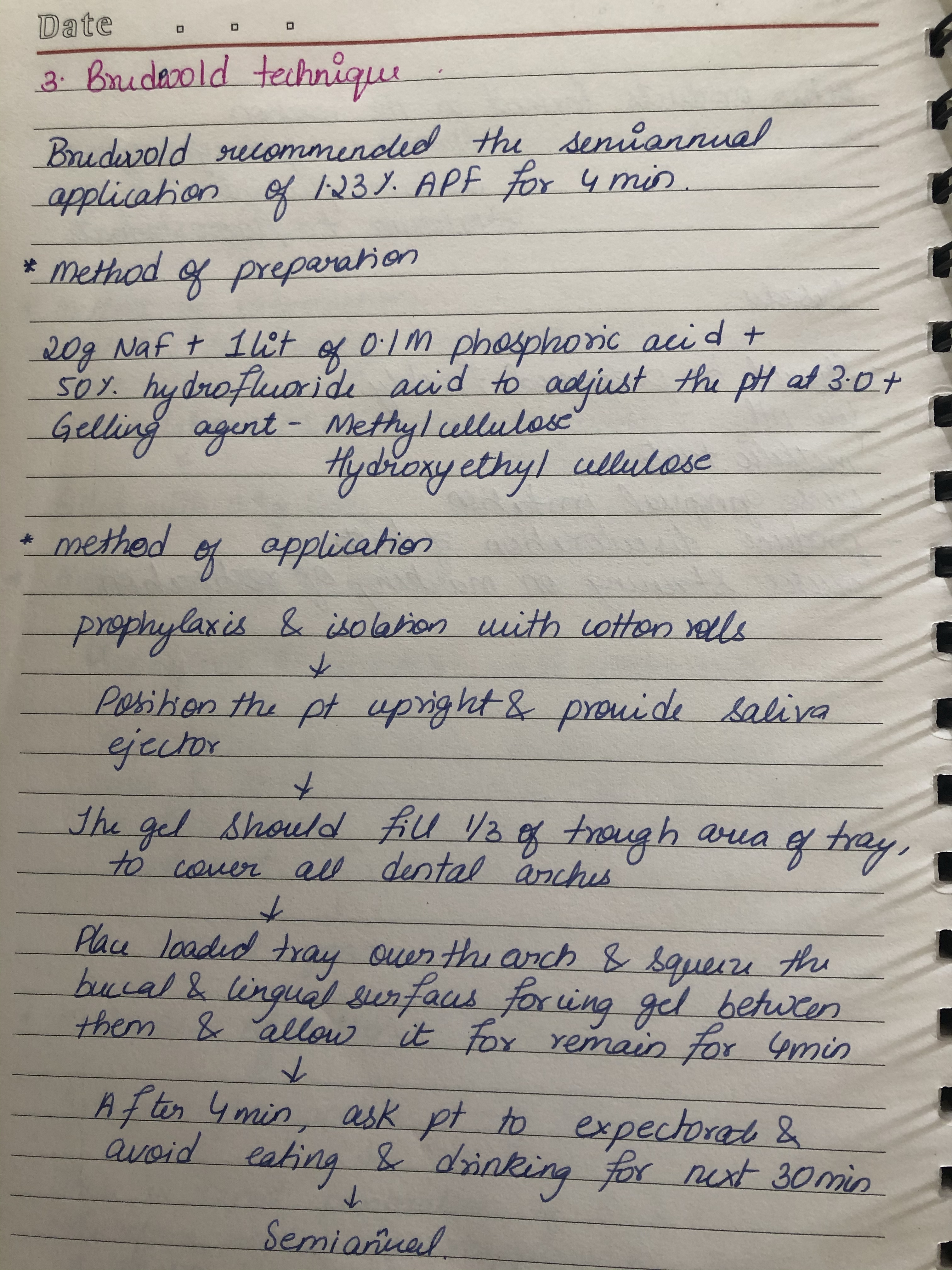
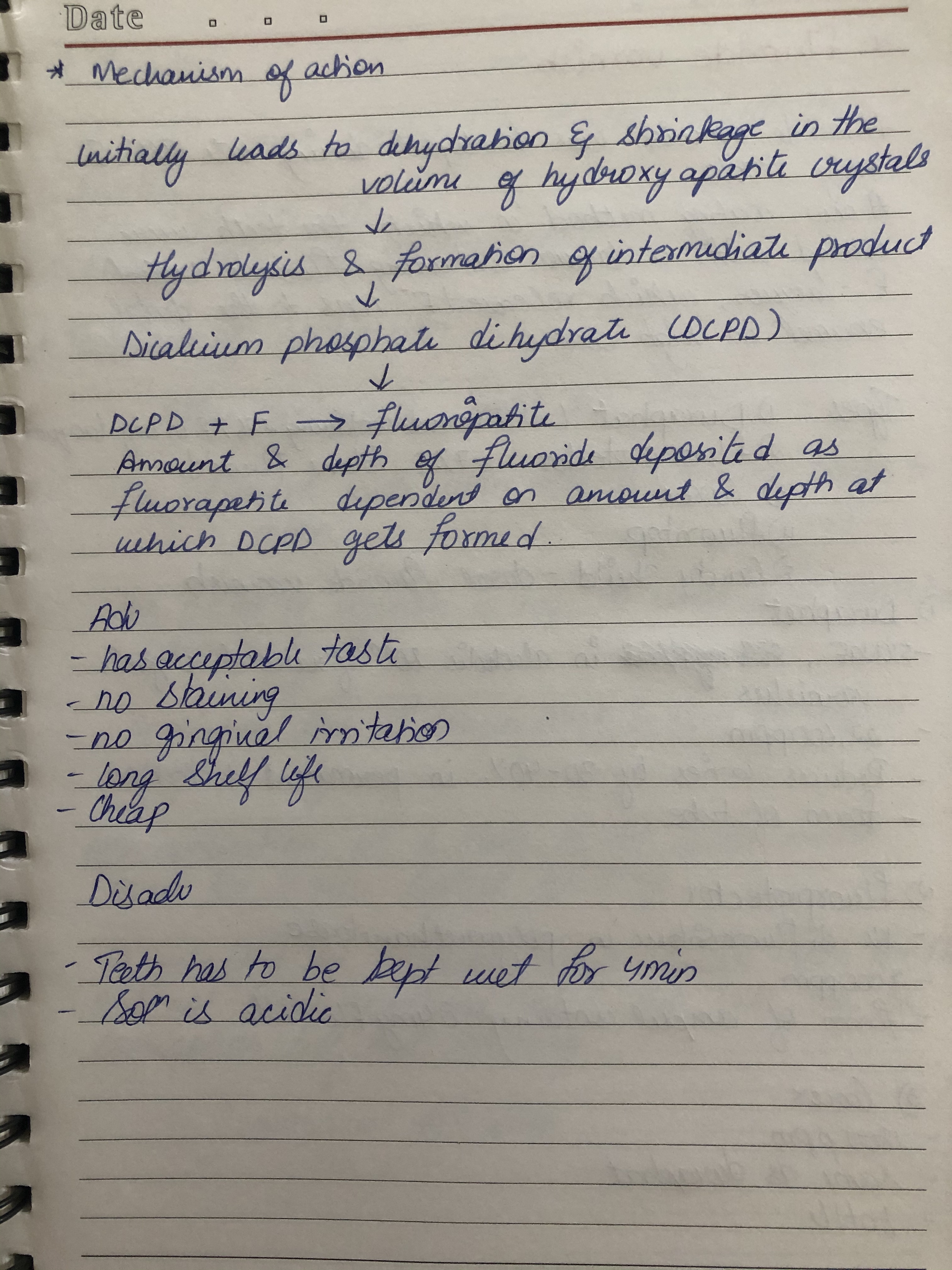
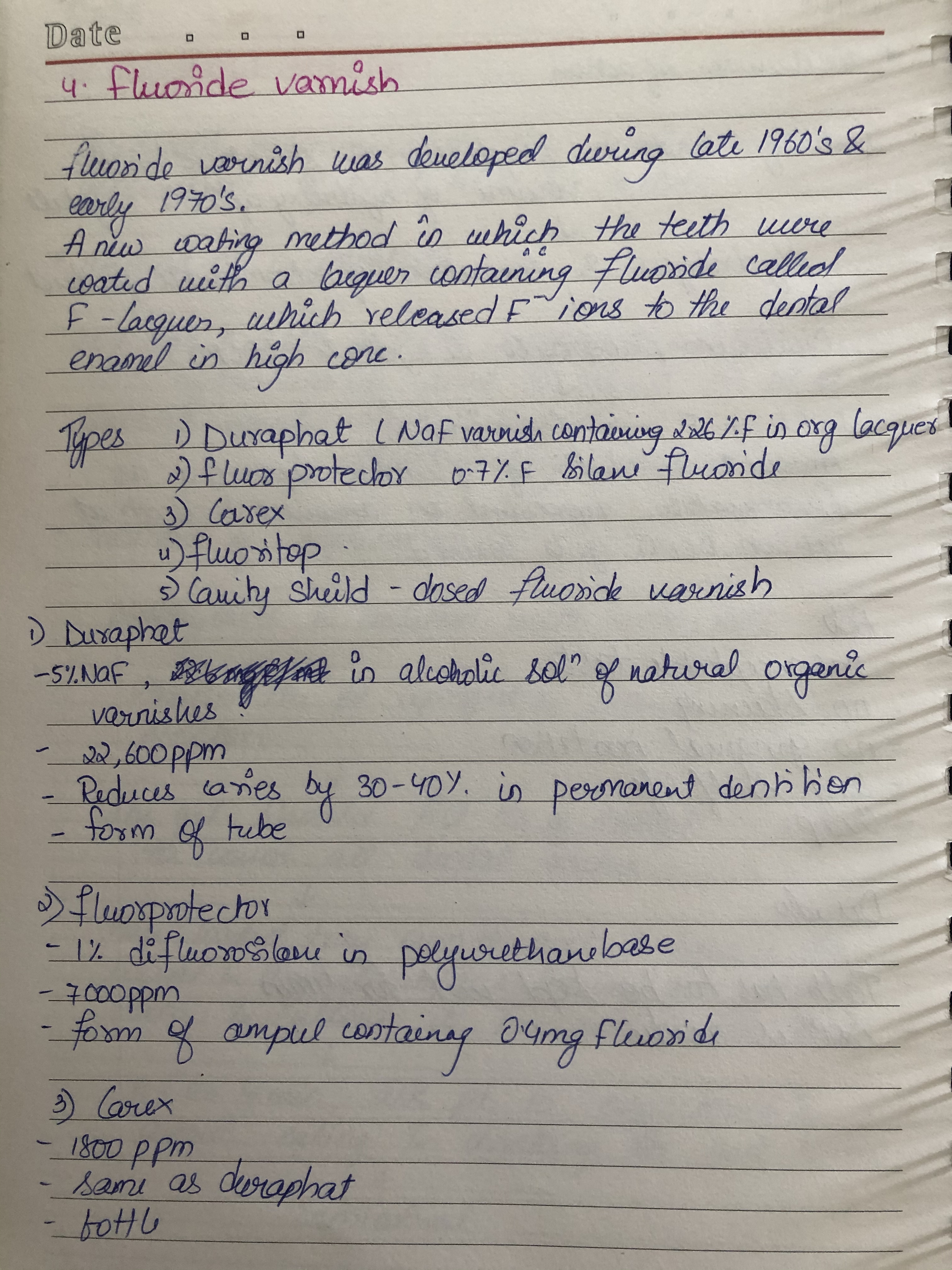
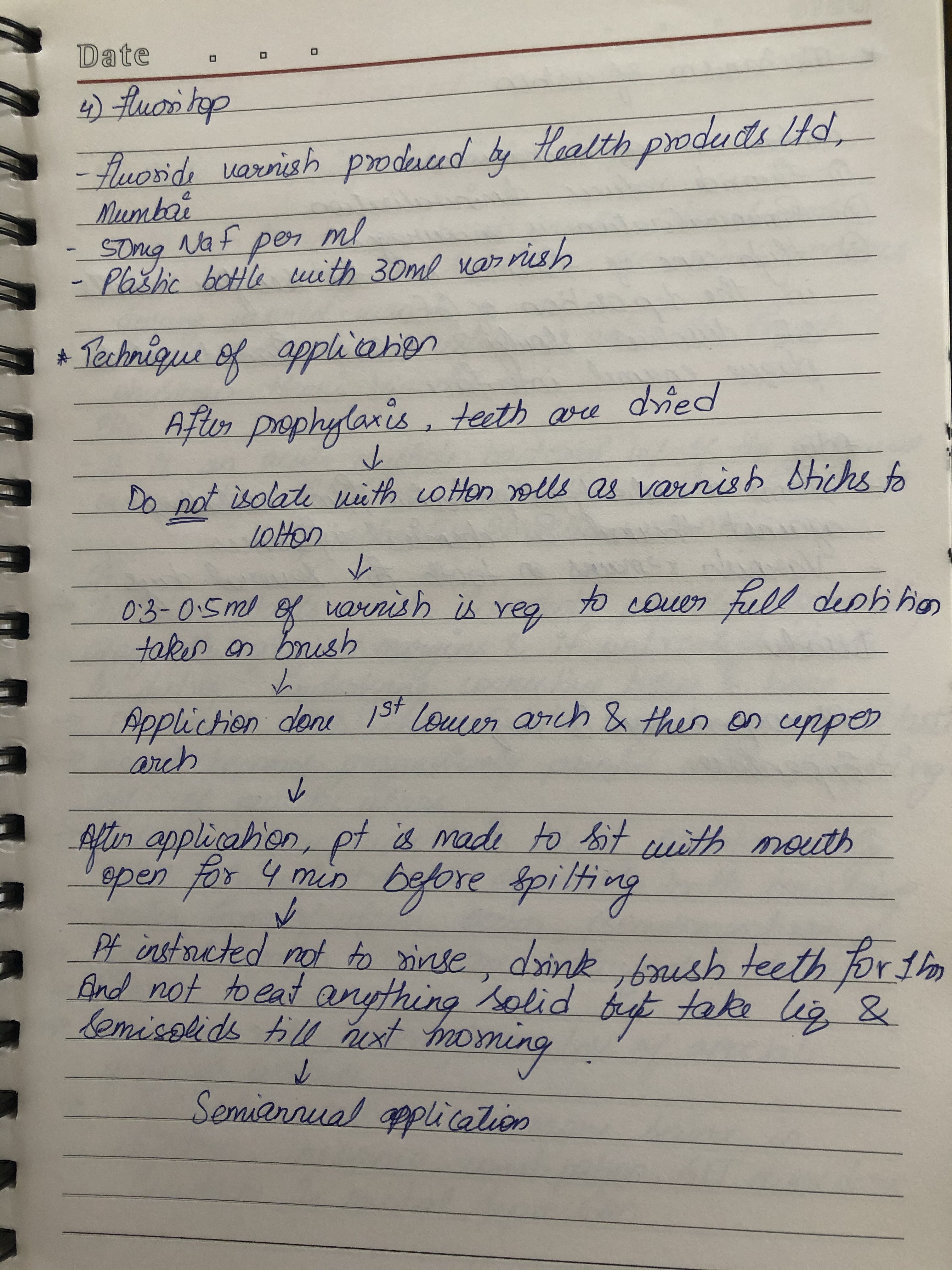
References: Phillips Science of Dental materials 12th Ed.

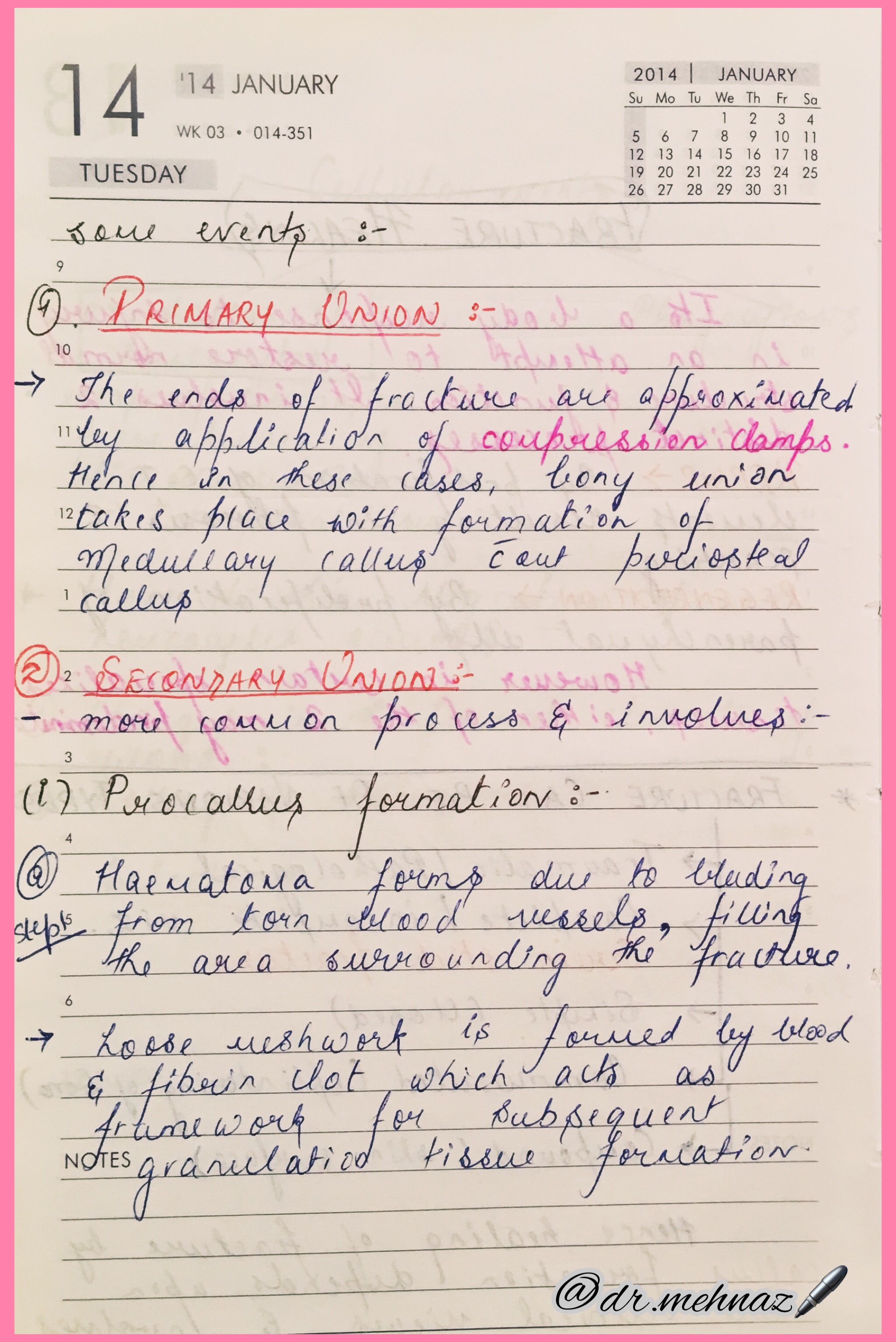
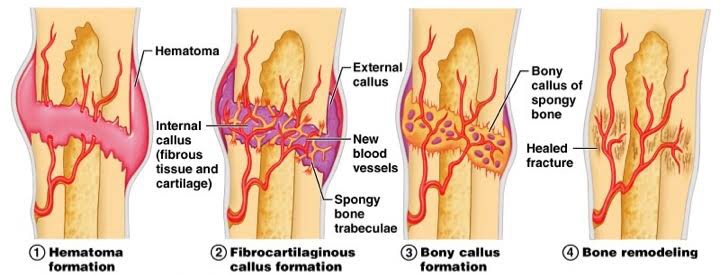
There are four stages in the repair of a broken bone:👇🏻😀




Dr. Mehnaz Memon🖊
Summary💡
🔅What are the 4 stages of bone healing?
•Hematoma formation
•Fibrocartilaginous callus formation
•Bony callus formation
•Bone remodeling
🔅What is callus formation in bone healing?
•Bone production begins when the clotted blood formed by inflammation is replaced with fibrous tissue and cartilage (known as soft callus). As healing progresses, the soft callus is replaced with hard bone (known as hard callus), which is visible on x-rays several weeks after the fracture.
🔅What foods heal bones faster?
•Iron helps your body make collagen to rebuild bone. It also plays a part in getting oxygen into your bones to help them heal.
•Good sources: Red meat, dark-meat chicken or turkey, oily fish, eggs, dried fruits, leafy green veggies, whole-grain breads, and fortified cereals.
🔅How long does it take for a broken bone to fully heal?
•A broken bone and the surrounding soft tissue damage need a minimum of six to eight weeks to heal. However, depending on your general health and the condition of your bone and soft tissue, healing can take much longer.
References:

🔍Tap to View in full size!



Dr. Mehnaz Memon🖊
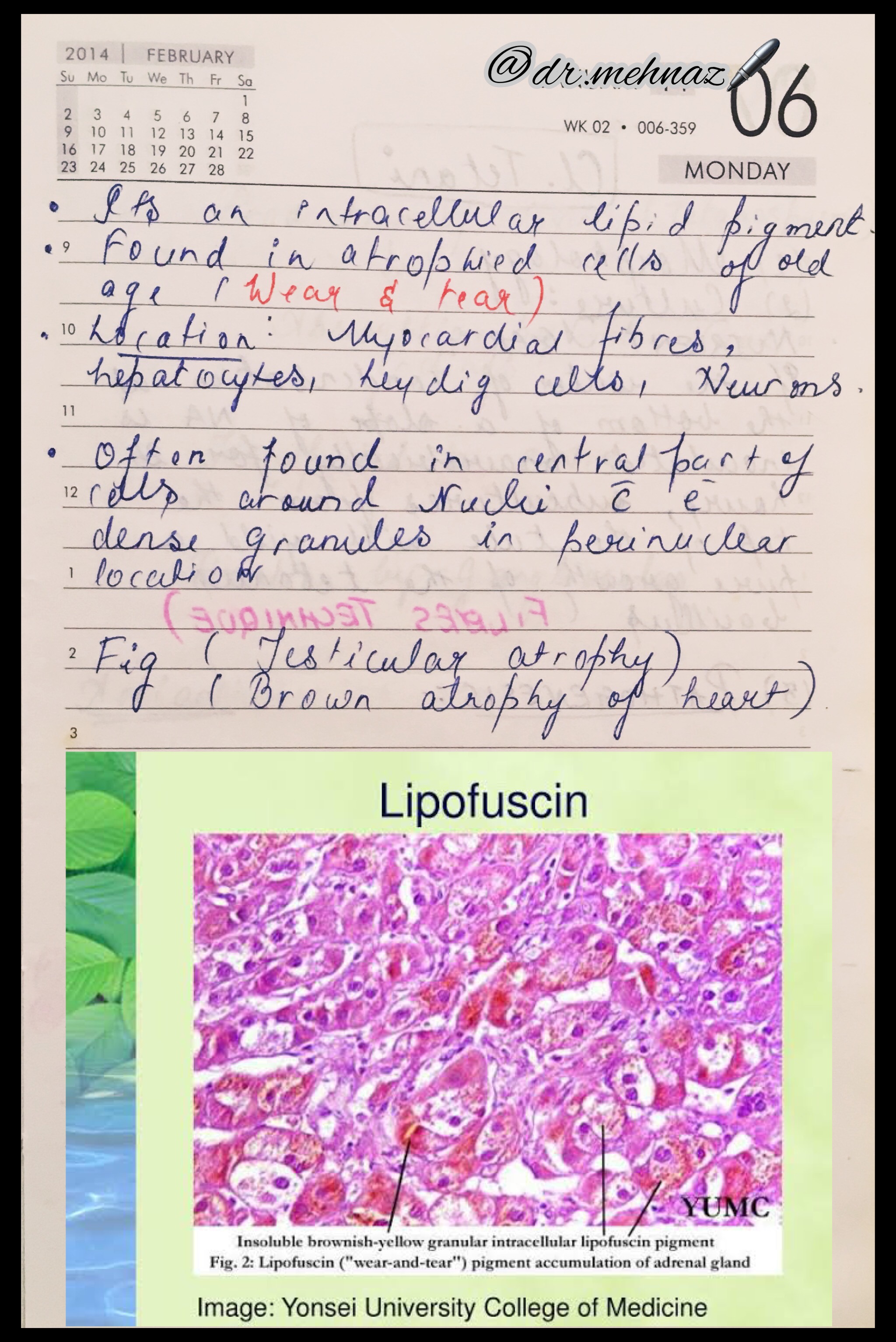
References: Textbook of Pathology, Harsh Mohan; Random google Images
Canine retractors are springs that are used to move canine in a distal direction.
1. Based on location
2. Based on presence of helix or loop
3. Based on mode of action
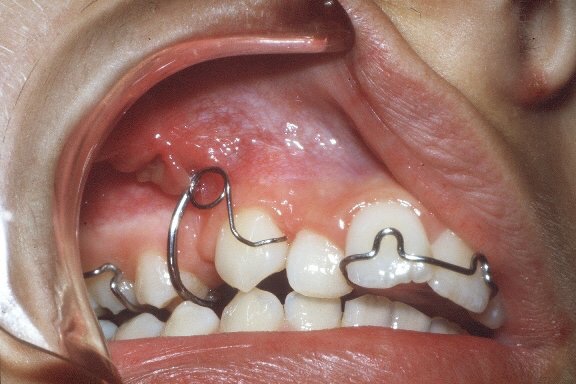
▪️BUCCAL CANINE RETRACTOR:
INDICATION: Is used where a buccally placed canine has to be moved palatally as well as distally.
TYPES:
• Self supporting or unsupported
• Supported
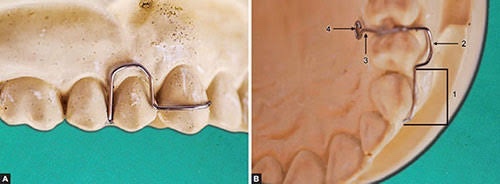
▪️SELF SUPPORTED BUCCAL CANINE RETRACTOR:

DESIGN & CONSTRUCTION
ACTIVATION
👉🏻The spring should be activated by only 1mm. Only spring which is activated by closing the coil
👉🏻Distal activation- It is effected at the coil by bending the anterior limb over the round beak of a pair of spring forming pliers
👉🏻Palatal activation- It is undertaken in the anterior limb after it emerges from the coil
DISADVANTAGES
▪️SUPPORTED BUCCAL CANINE RETRACTOR:

DESIGN
ACTIVATION
▪️AN APPLIANCE TO RETRACT BUCCAL CANINE
Indication
▪️SOLDERED AUXILIARY SPRINGS TO MOVE A CANINE PALATALLY
• It is possible to solder a spring{0.7mm wire} to the bridge of the adams clasp on a first molar.
• The spring can be used to tuck an outstanding canine
Advantages
Disadvantages
▪️REVERSE LOOP BUCCAL RETRACTOR:
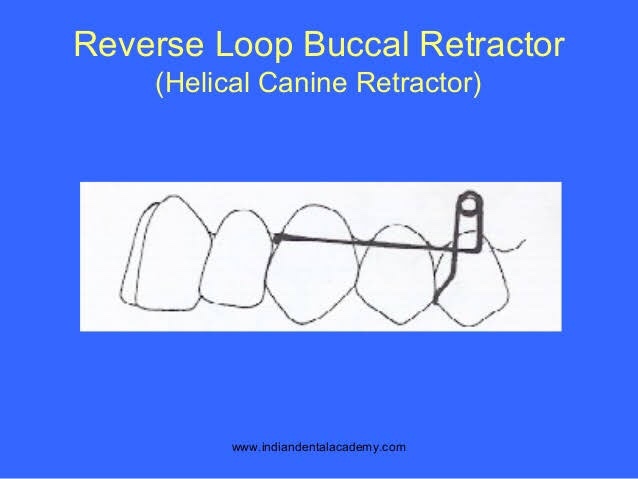
INDICATION
DESIGN
ACTIVATION
DRAWBACKS
• It is stiff in the horizontal plane yet very unstable vertically
▪️An appliance to retract lower canine
Indication
Anterior crowding
Active component
Reverse loop buccal retractor
Retention
Adams clasp on 6|6
Baseplate
A lingual bar rather than acrylic in the incisor region
Anchorage
Clasped teeth
Teeth and alveolar process contacted by the appliance
▪️U loop canine retractor
INDICATIONS
DESIGN
ACTIVATION – Close the loops by 1mm or free end is cut by 1mm & it is readapted on to the mesial side
DRAWBACKS – Requires frequent adjustments
▪️AN APPLIANCE TO MOVE A CANINE OCCLUSALLY
Indication – Partially erupted canine
Active component – U loop canine retractor, engages a hook bonded to the buccal surface of the canine
Retention – Adams clasp on 6|6
Baseplate – As much palatal coverage as the canine position permits to offer max. resistance to the occlusally directed force
Anchorage – Acrylic in the palate
▪️Buccal acrylic appliance to retract lower canine
Indication – To overcome the dual problems of limited space for tongue & poor retention provided by adams clasp
Active component – Buccal canine spring 0.7mm
Retention – Lingually placed jacksons clasp on the first molar [to overcome the problem of limited undercut on the buccal aspect of lower molars, appliances have been described with clasping on the lingual aspect of molars BELL 1983]
Baseplate – 2 segments of acrylic 1-2mm from the buccal mucosa. These are connected in the midline by a heavy ss bar, {2mm x 1mm}oval in cross section lying close to buccal mucosa below the lower incisors
Anchorage – First molar, with minimal anchorage effect from acrylic
▪️PALATAL CANINE RETRACTOR:
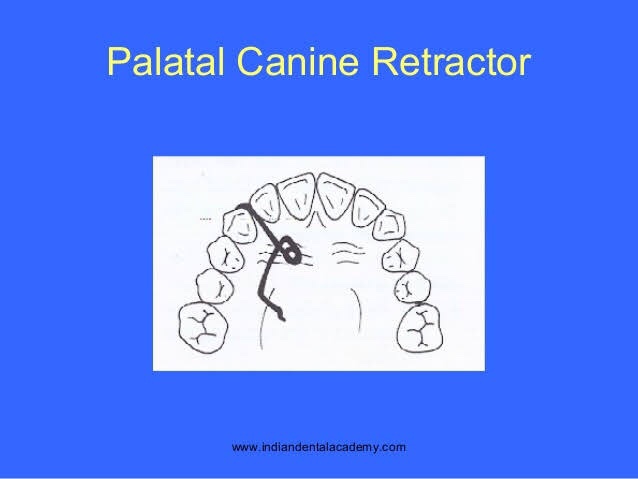
INDICATIONS – In cases where canine is placed palatally & requires distal & buccal movement
DESIGN
ACTIVATION – By opening the coil by 2-3mm where the active arm emerges out of the coil
▪️CONCLUSION:
• For canine retractors whether buccal or palatal to be successful, it is important for the canines to be mesially angulated prior to treatment
• If the canine is normal & distally angulated prior to treatment, a removable canine retractor will cause an unsightly distal angulation of the canine at the completion of retraction which in turn will take a long time to correct with fixed appliance
• For this reason, use of removable appliance for canine retraction is declining as fixed appliance have greater control over tooth movement
References:
A chronic, autoimmune, sub-epidermal blistering skin disease that rarely involves mucous membrane.

Age: Elderly (>60 years)
Skin Lesions:
Oral Manifestations:
Vesicles appear gingivally👇🏻

Erythematous & desquamate as result of minor frictional trauma
👉🏻 Oral lesions comprise of bullae/vesicle that rupture to form erosions and ultimately leave out ulcerations
👉🏻 Other sites:

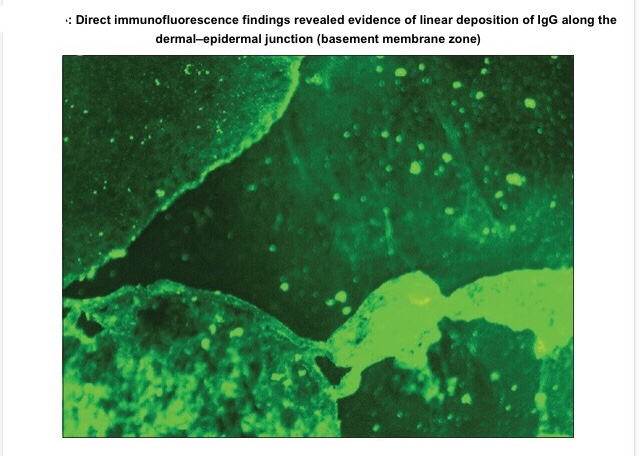
Apart from evaluating history, clinical presentation, histopathological analysis is carried out followed by direct immunofluorescence study for the differential diagnosis and confirmation of the condition.
👉🏻Histopathology:
👉🏻Direct immunofluorescence is found to be the gold standard test. Deposition pattern of different types of immunoreactants differentiates the various immune-mediated diseases. Direct immunofluorescence shows presence of IgG and C3 deposits along the basement membrane zone.
👉🏻Electron Microscopy: In bullous pemphigoid (BP), the 180 kD antigen (BPAG2) was shown by immuno-EM to be a transmembrane molecule and to possess an autoantibody binding site outside the cell, suggesting a major pathogenic role for the BPAG2 in blister formation.
• Mucous membrane pemphigoid can be differentiated from BP by its predominant involvement of mucosal surfaces and positive Nikolsky’s sign.
• Lichen planus pemphigoides is clinically differentiated by the presence of lichen planus lesions in addition to tense blisters.
• Nikolsky’s sign is present in case of pemphigus and cicatricial pemphigoid, but not in the case of BP.
👉🏻Treatment is based on the degree of cutaneous and oral involvement. Mostly, topical steroid (clobetasol propionate) gives satisfactory result in case of smaller area of skin involvement, whereas larger area of skin involvement and recurrent cases are treated satisfactorily with systemic steroids and immunosuppressive agents.
👉🏻Recommended dosage for oral prednisolone is 0.3–1.25 mg/kg body weight/day, controls disease within 1–2 weeks, followed by which the dose is tapered. Dexamethasone (100 mg in 500 mL 5% dextrose i.v. over 2–3 h for three consecutive days) is the preferred steroid for pulse therapy, either administered alone or in combination with cyclophosphamide.
Other drugs for treating BP include new antibody modulators, rituximab 375mg/m2weekly over 4 weeks and omalizumab subcutaneously 300–375 mg for every 6 weeks.
👉🏻Higher doses of systemic corticosteroids seem to be associated with higher mortality rates, which led to the addition of corticosteroid-sparing agents to the treatment of BP. The most frequently used immunosuppressive agent is azathioprine (0.5–2.5 mg/kg body weight/day). Others being cyclophosphamide, methotrexate, cyclosporine A, combination tetracycline/minocycline along with nicotinamide, and more recently, mycophenolate mofetil, a DNA synthesis inhibitor, and methotrexate, a folate antagonist.
👉🏻IVIg – A dose of 1–2 g/kg for five consecutive day cycle of 0.4 g/kg/day, although a 3-day cycle may be used in cases that are nonresponsive to conventional therapy.
Dr. Mehnaz Memon🖊
References:
🔖 Acrocephalosyndactyly. The condition is autosomal dominant i.e, one copy (out of 2) of the defective gene is sufficient to cause the abnormality in the offspring.
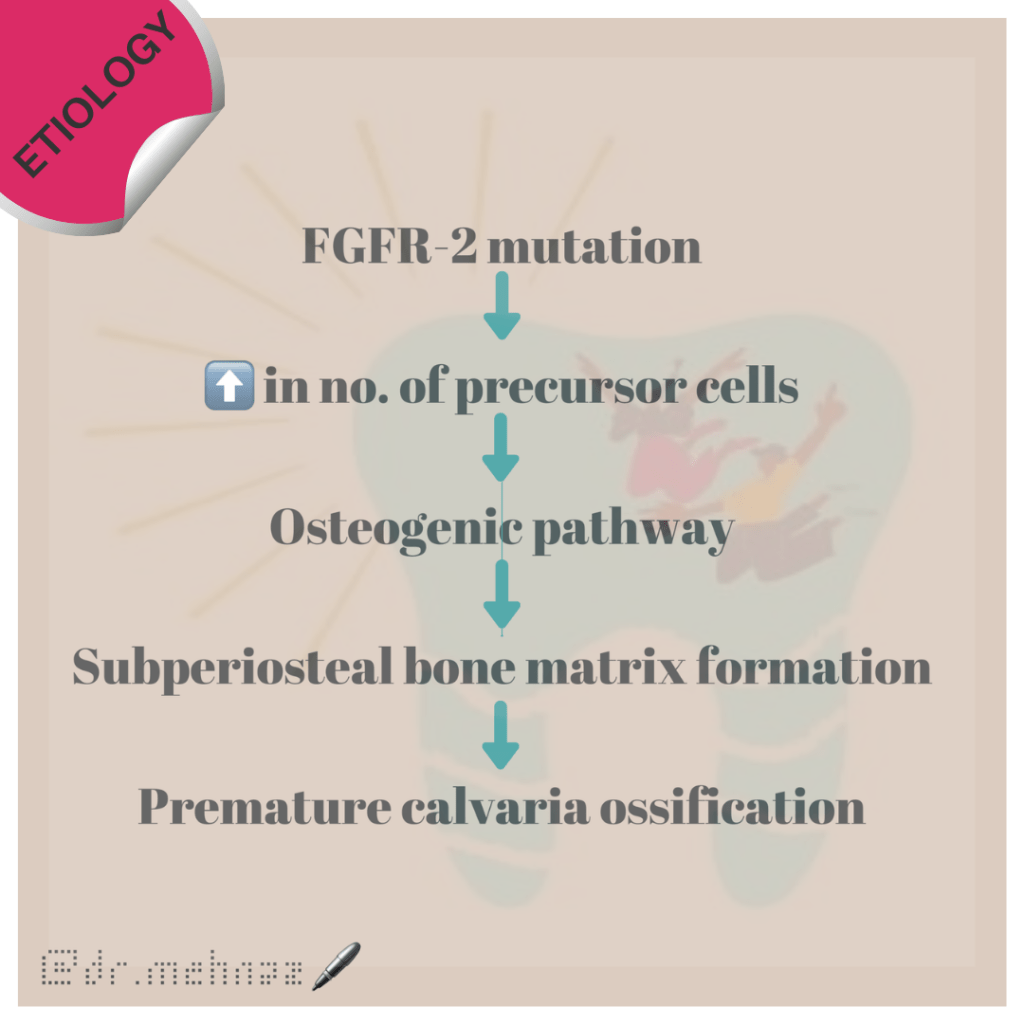
The various clinical features include:

8. Partial to complete fusion of digits: 2-4th digits – MITTEN HANDS & SOCK FEET; Sole – supinated
9. Intelligence – Normal
10. ⬆️ intracranial pressure – optic atrophy, papilledema
11. Hyperhidrosis
12. Cardiovascular system: Atrial Septal defect, Ventricular septal defect, Patent ductus Arteriosus
Standard Therapies
The treatment of Apert syndrome aims at addressing the specific symptoms that may be present in the particular individual. Treatment is usually symptomatic and supportive.
Dr. Mehnaz Memon🖊
References:
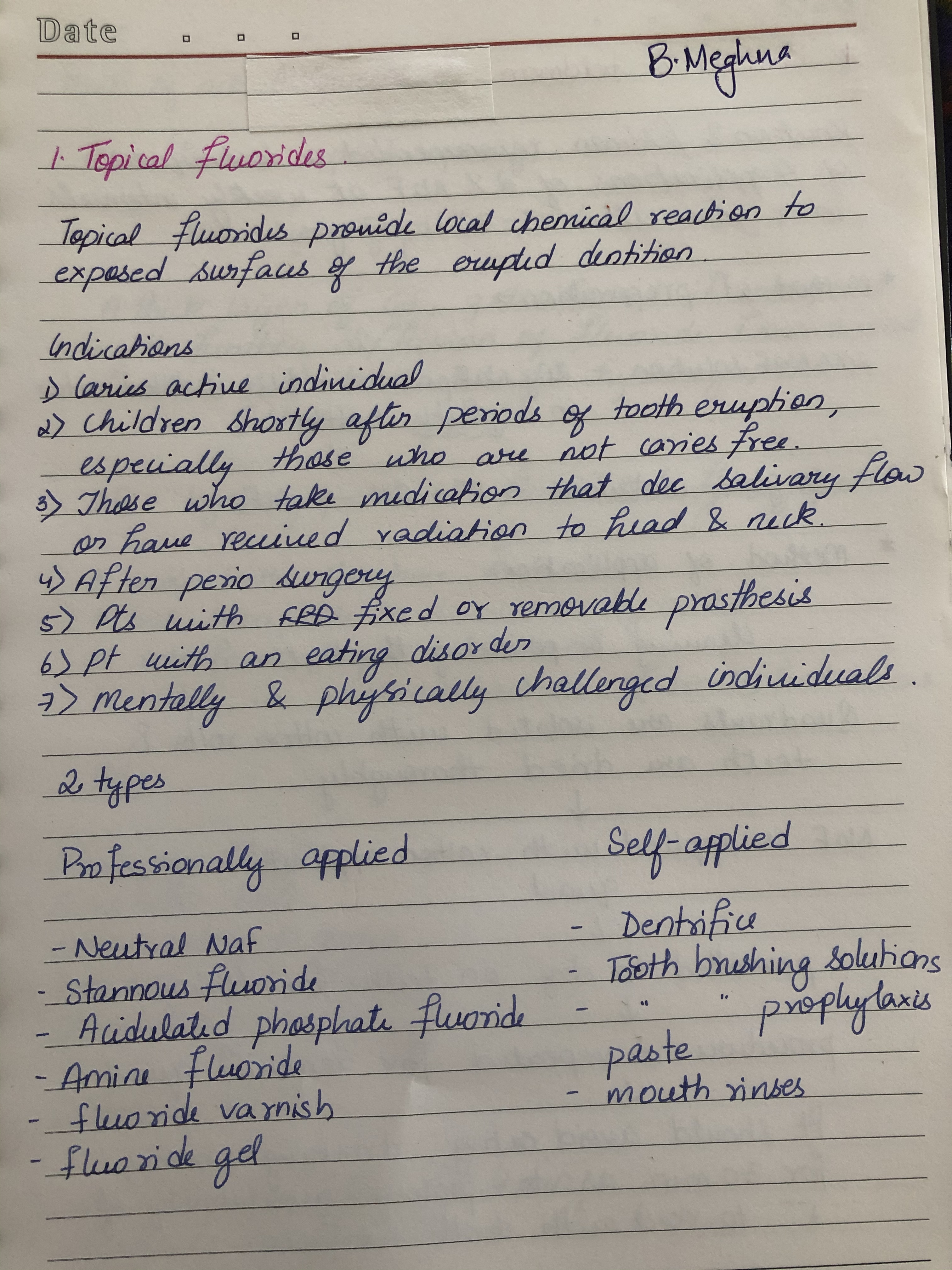
Written by-B Meghna
Source- Nikhil Marwah textbook of pedodontics and soben peter textbook of public health dentistry
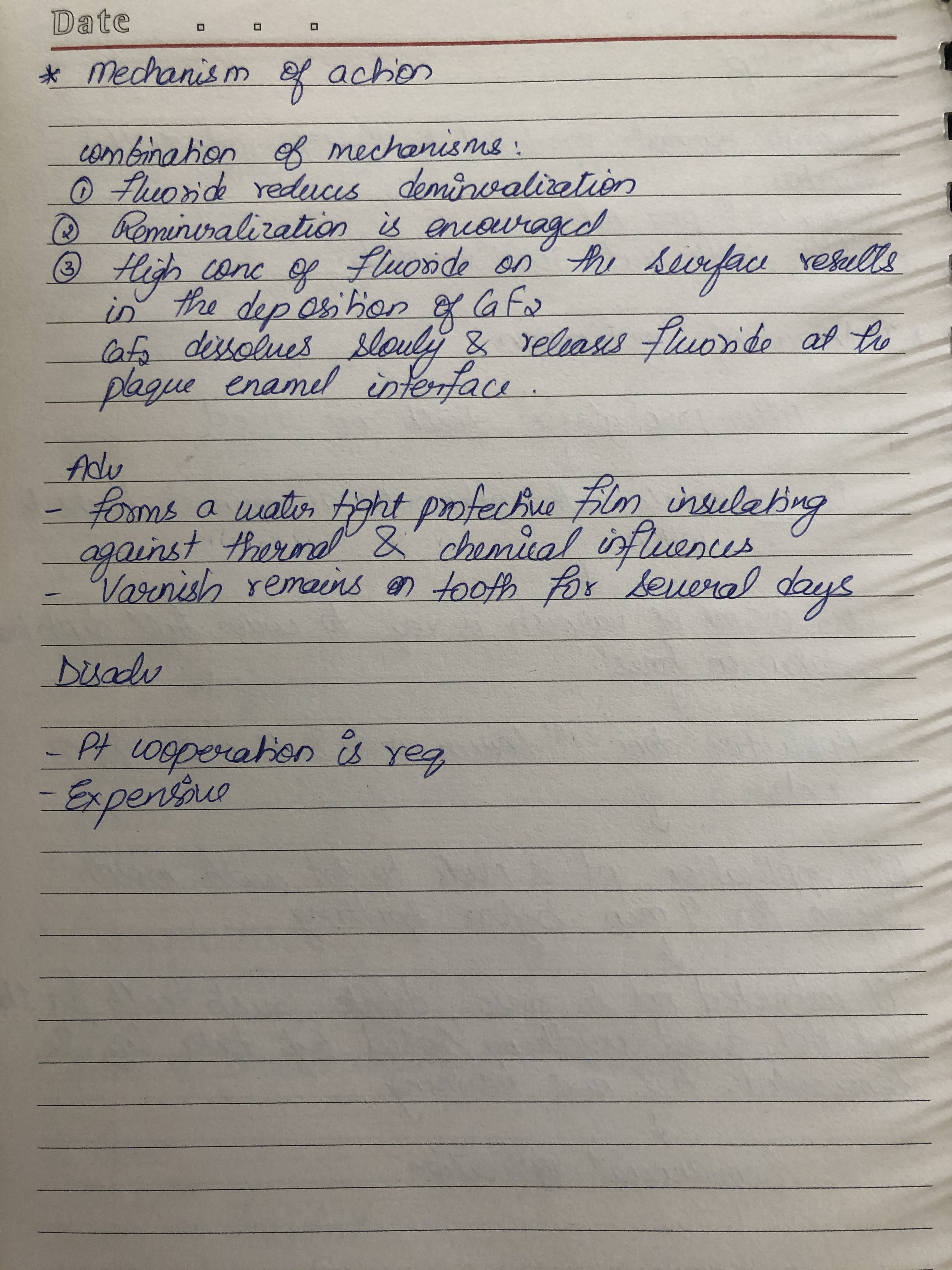
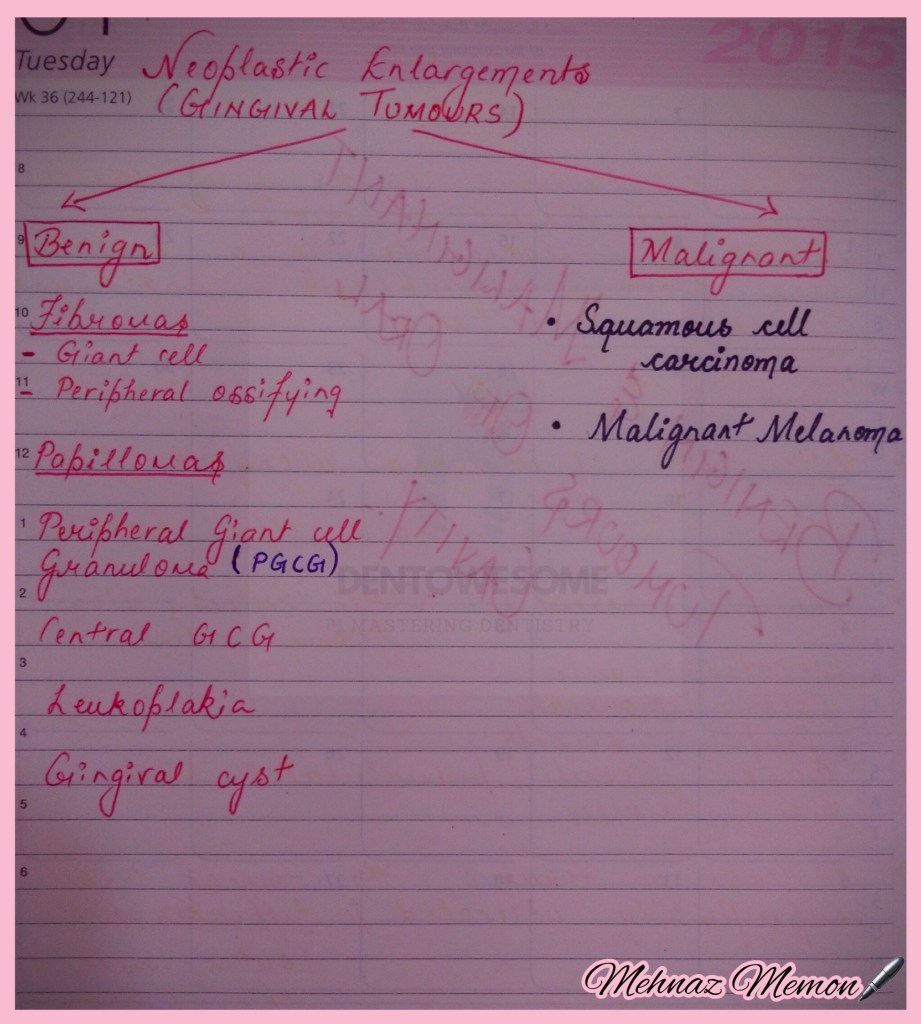
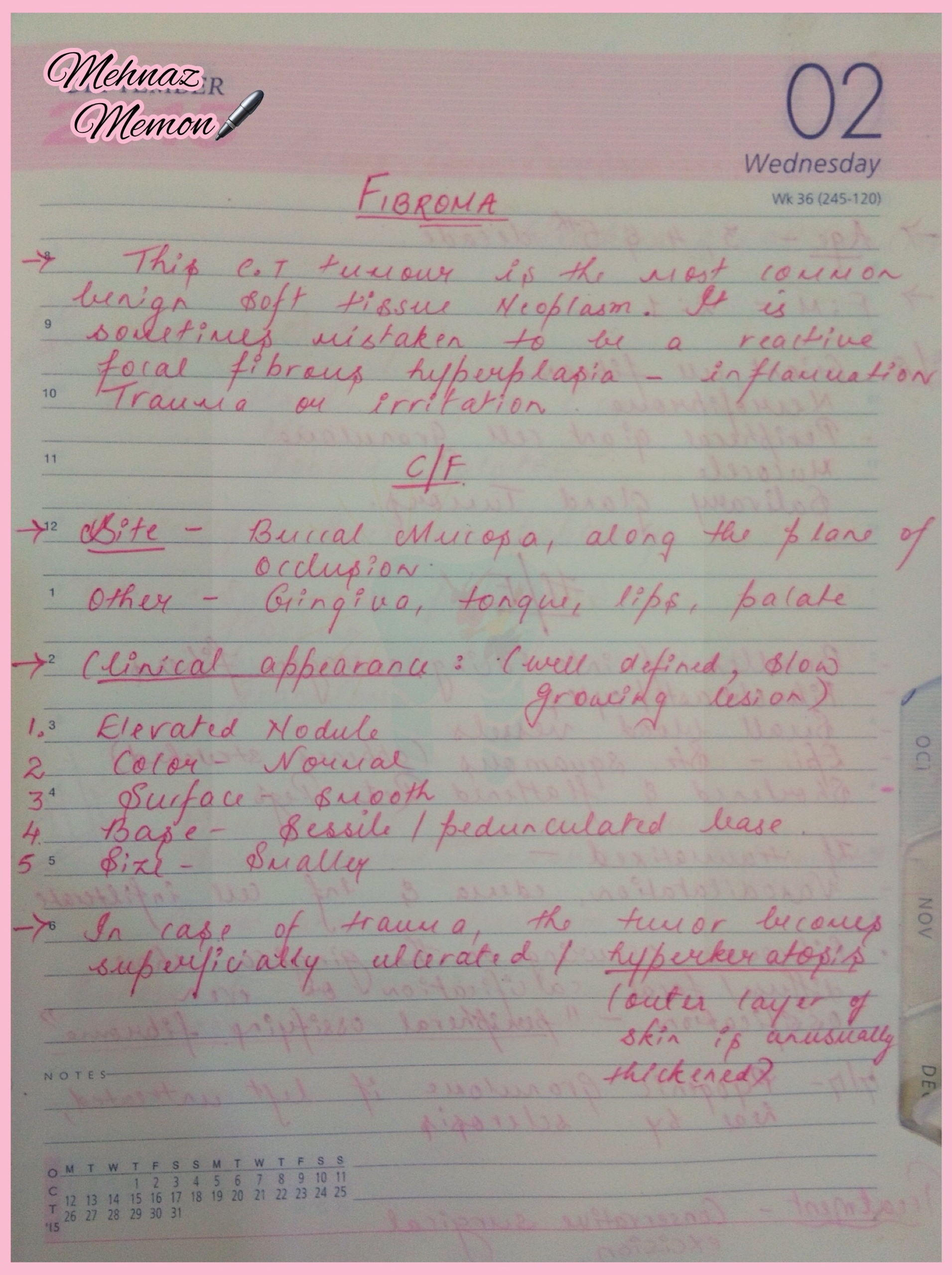
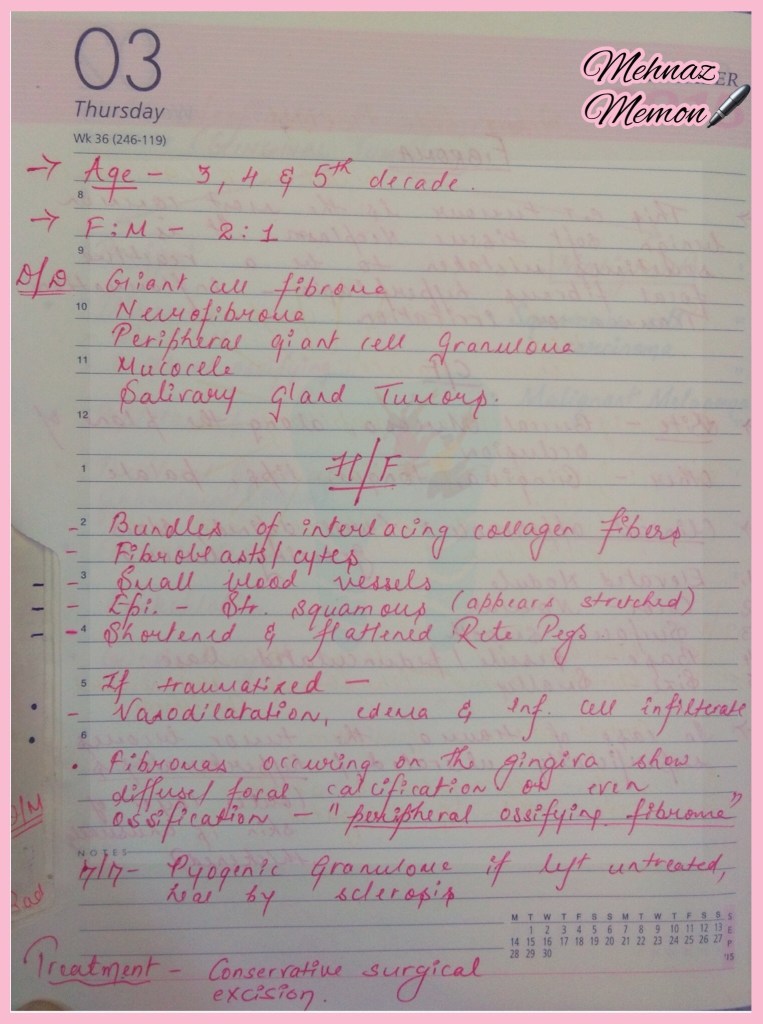
a. Fibromas

Page 1 of 3
Read More »