Highlights (You will learn) ⬇️
1. Trigeminal Neuralgia
2. Post-herpetic Neuralgia
3. Giant-cell Arteritis
4. Other causes of facial pain
5. Approach to facial pain diagnosis
LINK:⬇️

1. Trigeminal Neuralgia
2. Post-herpetic Neuralgia
3. Giant-cell Arteritis
4. Other causes of facial pain
5. Approach to facial pain diagnosis
LINK:⬇️

PA radiolucencies identification made easy! Happy learning..😀📖
When formulating radiological differential diagnosis, features should be evaluated carefully, such as
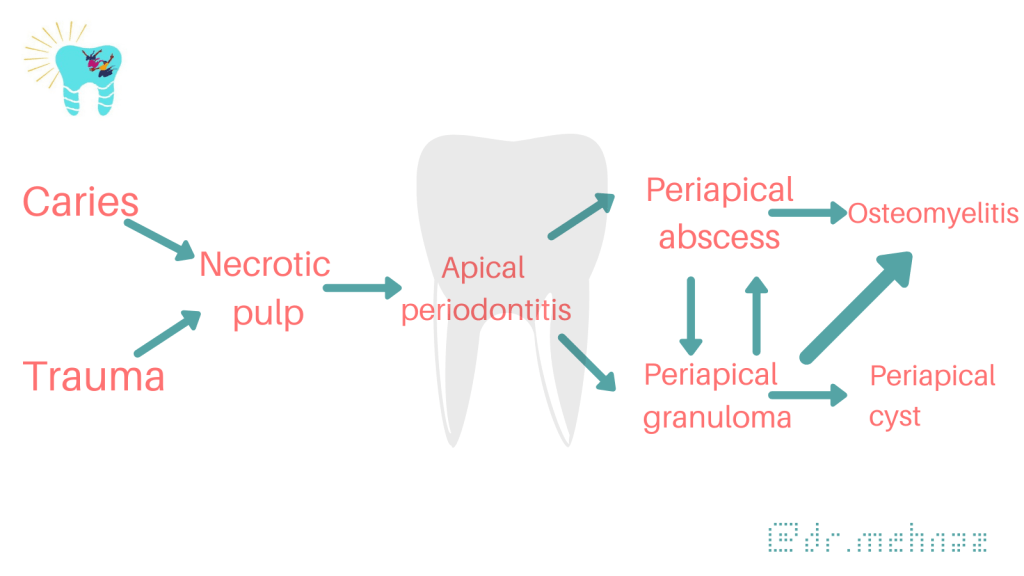
• Location: With periapical inflammatory lesions, which are pathological conditions of the pulp, the epicenter typically is located at the apex of a tooth.
• Periphery: Ill defined
• Effects on surrounding structures: Periapical lesions cause widening of PDL space at apical region of the root.

PERIAPICAL RADIOLUCENCIES
Developmental
Lateral periodontal cyst

Inflammatory Lesions
Apical periodontitis, periapical abscess


Cystic Lesions
Periapical (radicular) cyst

Odontogenic keratocyst

Glandular odontogenic cyst
Benign Tumors
Ameloblastoma

Malignant Tumors
Ameloblastic carcinoma


Dentowesome|@drmehnaz🖊
References:
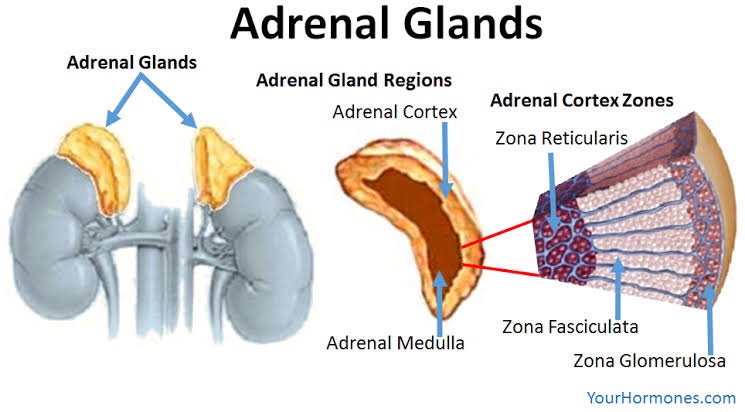
Steroids are a group of hormones produced naturally in the body.
The adrenal cortex consists of 3 zones:
• Glucocorticoid secretion is regulated by ACTH produced in the anterior pituitary. Cortisol has a -ve feedback on ACTH production.
• In Addison diseases, Glucocorticoid secretion impaired & ACTH is ⬆️
Stress
⬇️
Release of cytokines (IL-1)
⬇️
⬆️ cortisol levels

The substrate for steroid production is cholesterol. It is mobilized from the outer to the inner mitochondrial membrane by the steroidogenic acute regulatory (StAR) protein.
• Action: Anti-allergy, anti-inflammatory
• Therapeutic Uses:
Action: Fibrinolytic,Anti-allergic, anti-inflammatory*
It causes ⬇️ fibroblastic production & deposition of collagen*
• Trade Name: CORTEF, ORABASE-HCA
• Preparation:
• Hydrocortisone acetate 25-50 mg/mL for soft tissue suspensions
• Hydrocortisone sodium phosphate: 50mg/mL IV, IM, SC
• Uses:
• Action: Anti-allergic, anti-inflammatory, immunosuppressive
• Uses:
• Trade name: DELTA-CORTEF, PRELONE
• Uses:
• Trade name: Kenolog cream
• Uses:
👉🏻Mainly used for adrenal cortical suppression
• Trade name: DECADRON
• Action: Anti-allergy, anti-inflammatory
• Uses: Lichen planus, pemphigus, Aphthae ulcer
Dr. Mehnaz Memon🖊
References: Self Notes, Image chart source: Classification of Drugs with DOC by Vikas Seth (Third Edition)

🔍Tap to View in full size!



Dr. Mehnaz Memon🖊
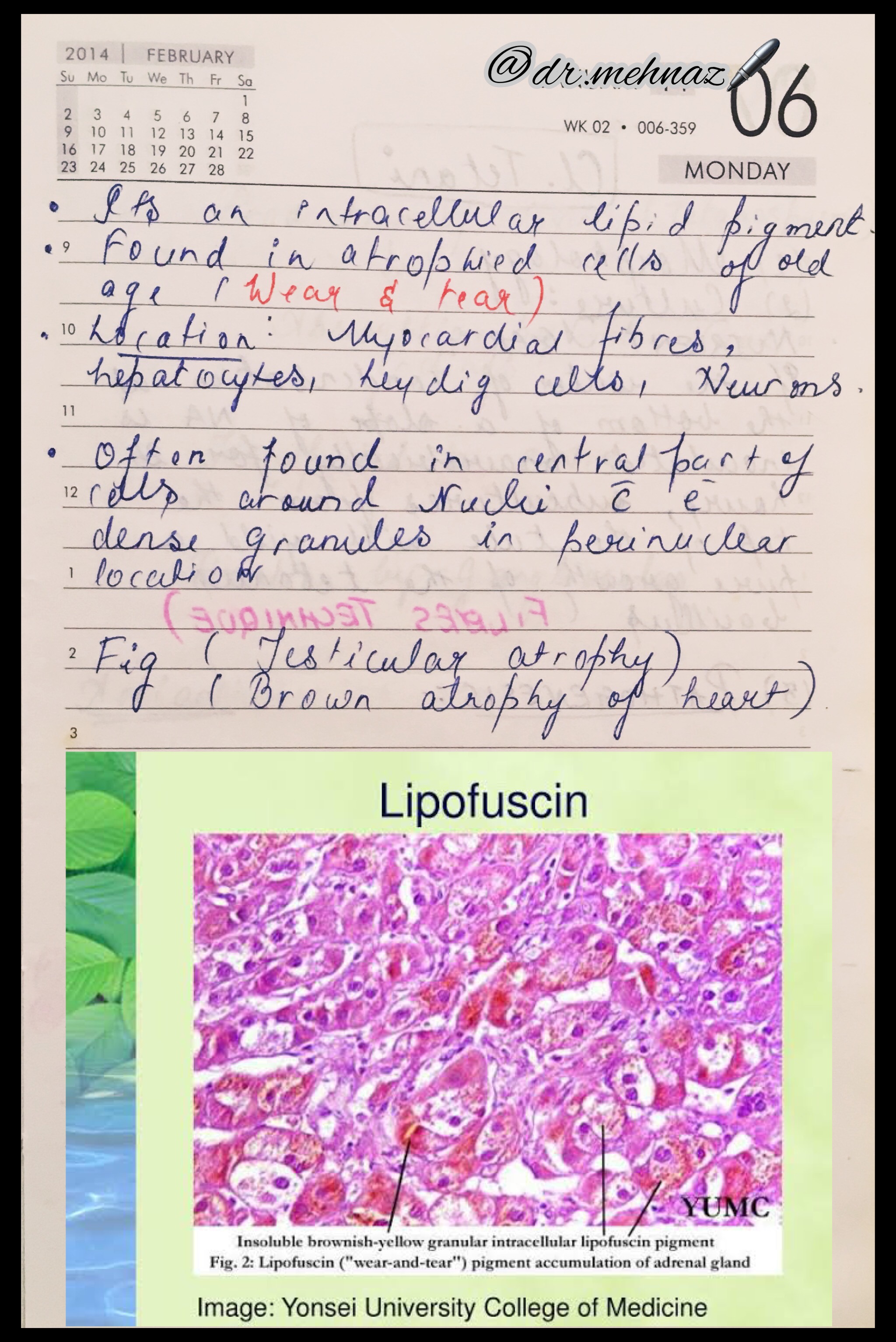
References: Textbook of Pathology, Harsh Mohan; Random google Images
A chronic, autoimmune, sub-epidermal blistering skin disease that rarely involves mucous membrane.

Age: Elderly (>60 years)
Skin Lesions:
Oral Manifestations:
Vesicles appear gingivally👇🏻

Erythematous & desquamate as result of minor frictional trauma
👉🏻 Oral lesions comprise of bullae/vesicle that rupture to form erosions and ultimately leave out ulcerations
👉🏻 Other sites:

Apart from evaluating history, clinical presentation, histopathological analysis is carried out followed by direct immunofluorescence study for the differential diagnosis and confirmation of the condition.
👉🏻Histopathology:
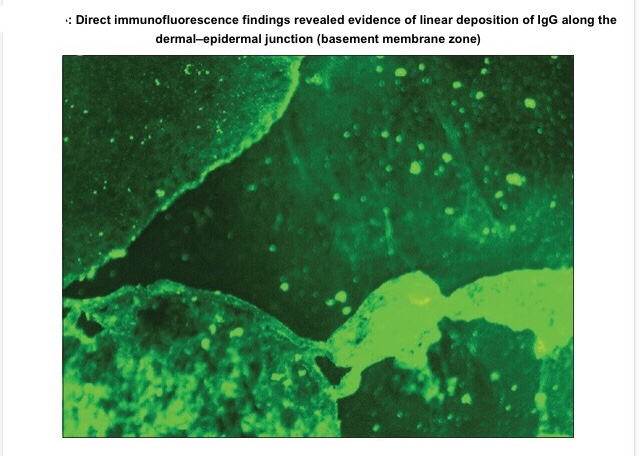
👉🏻Direct immunofluorescence is found to be the gold standard test. Deposition pattern of different types of immunoreactants differentiates the various immune-mediated diseases. Direct immunofluorescence shows presence of IgG and C3 deposits along the basement membrane zone.
👉🏻Electron Microscopy: In bullous pemphigoid (BP), the 180 kD antigen (BPAG2) was shown by immuno-EM to be a transmembrane molecule and to possess an autoantibody binding site outside the cell, suggesting a major pathogenic role for the BPAG2 in blister formation.
• Mucous membrane pemphigoid can be differentiated from BP by its predominant involvement of mucosal surfaces and positive Nikolsky’s sign.
• Lichen planus pemphigoides is clinically differentiated by the presence of lichen planus lesions in addition to tense blisters.
• Nikolsky’s sign is present in case of pemphigus and cicatricial pemphigoid, but not in the case of BP.
👉🏻Treatment is based on the degree of cutaneous and oral involvement. Mostly, topical steroid (clobetasol propionate) gives satisfactory result in case of smaller area of skin involvement, whereas larger area of skin involvement and recurrent cases are treated satisfactorily with systemic steroids and immunosuppressive agents.
👉🏻Recommended dosage for oral prednisolone is 0.3–1.25 mg/kg body weight/day, controls disease within 1–2 weeks, followed by which the dose is tapered. Dexamethasone (100 mg in 500 mL 5% dextrose i.v. over 2–3 h for three consecutive days) is the preferred steroid for pulse therapy, either administered alone or in combination with cyclophosphamide.
Other drugs for treating BP include new antibody modulators, rituximab 375mg/m2weekly over 4 weeks and omalizumab subcutaneously 300–375 mg for every 6 weeks.
👉🏻Higher doses of systemic corticosteroids seem to be associated with higher mortality rates, which led to the addition of corticosteroid-sparing agents to the treatment of BP. The most frequently used immunosuppressive agent is azathioprine (0.5–2.5 mg/kg body weight/day). Others being cyclophosphamide, methotrexate, cyclosporine A, combination tetracycline/minocycline along with nicotinamide, and more recently, mycophenolate mofetil, a DNA synthesis inhibitor, and methotrexate, a folate antagonist.
👉🏻IVIg – A dose of 1–2 g/kg for five consecutive day cycle of 0.4 g/kg/day, although a 3-day cycle may be used in cases that are nonresponsive to conventional therapy.
Dr. Mehnaz Memon🖊
References:
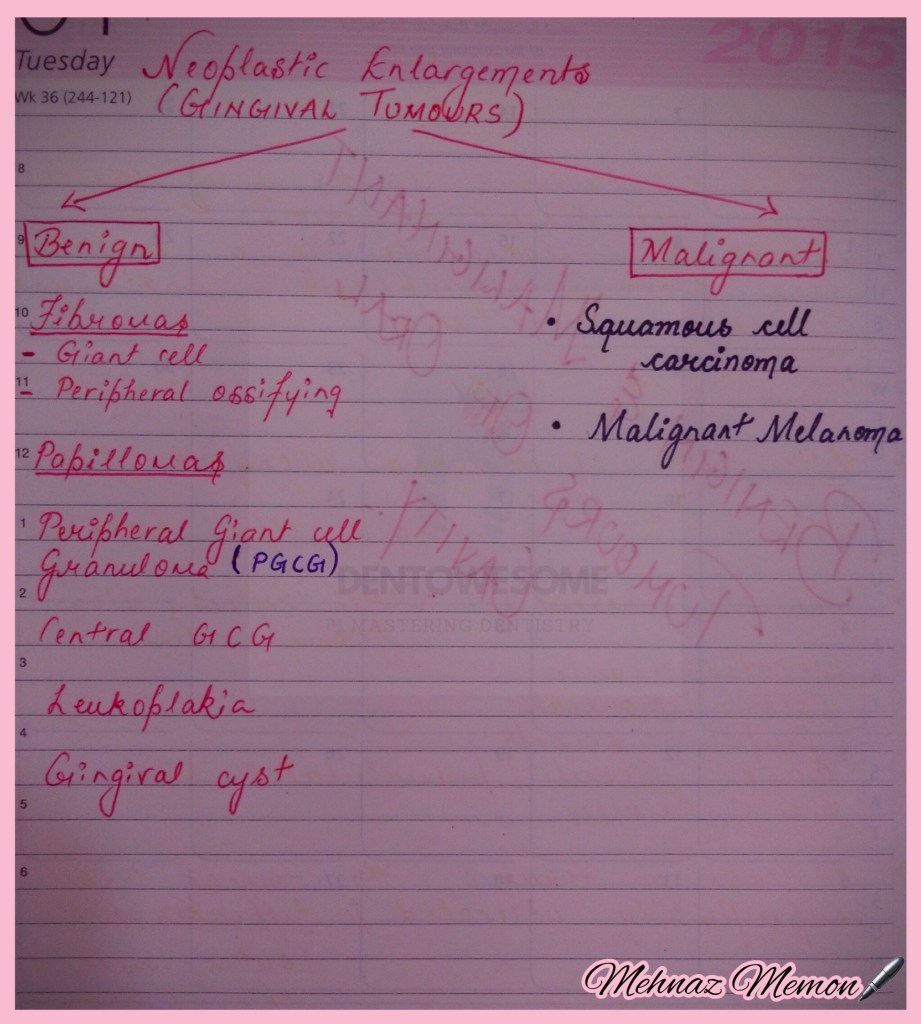
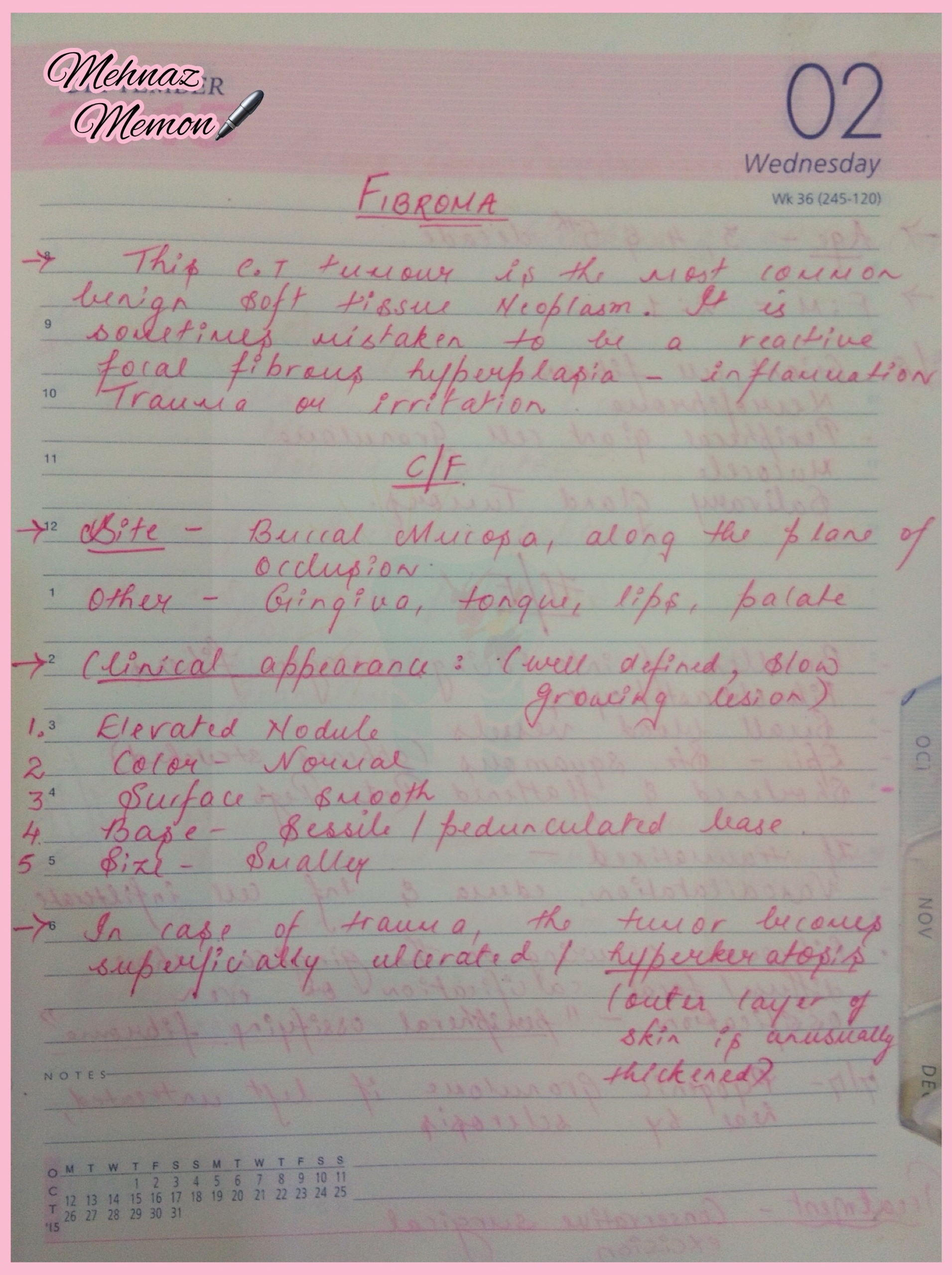
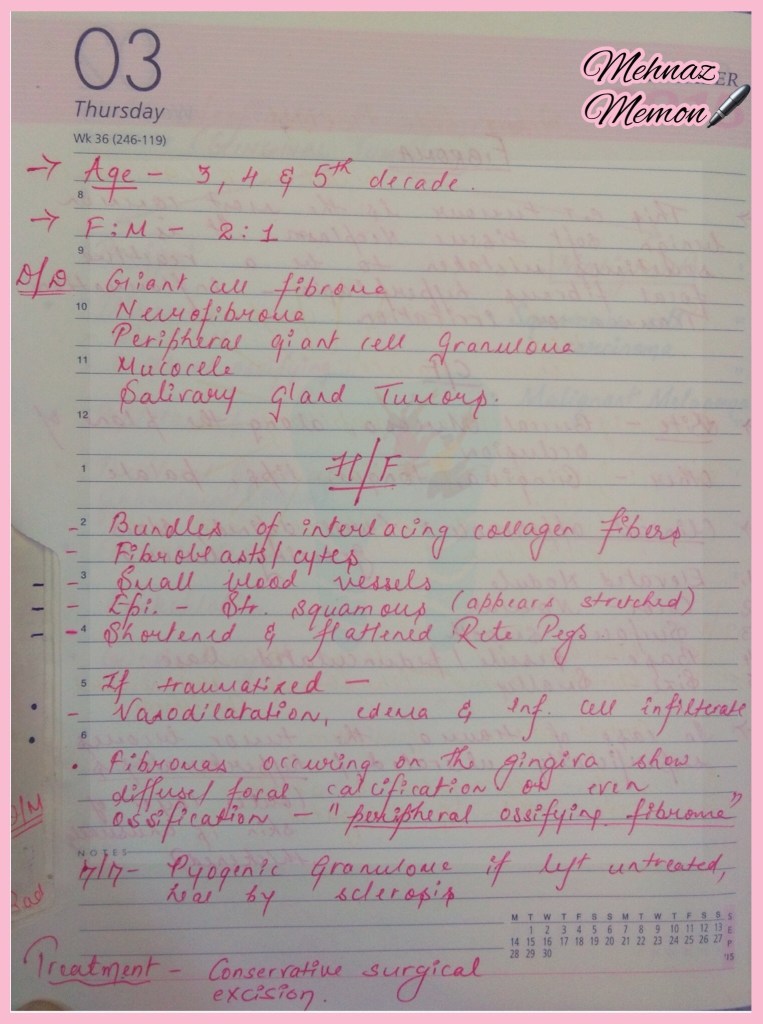
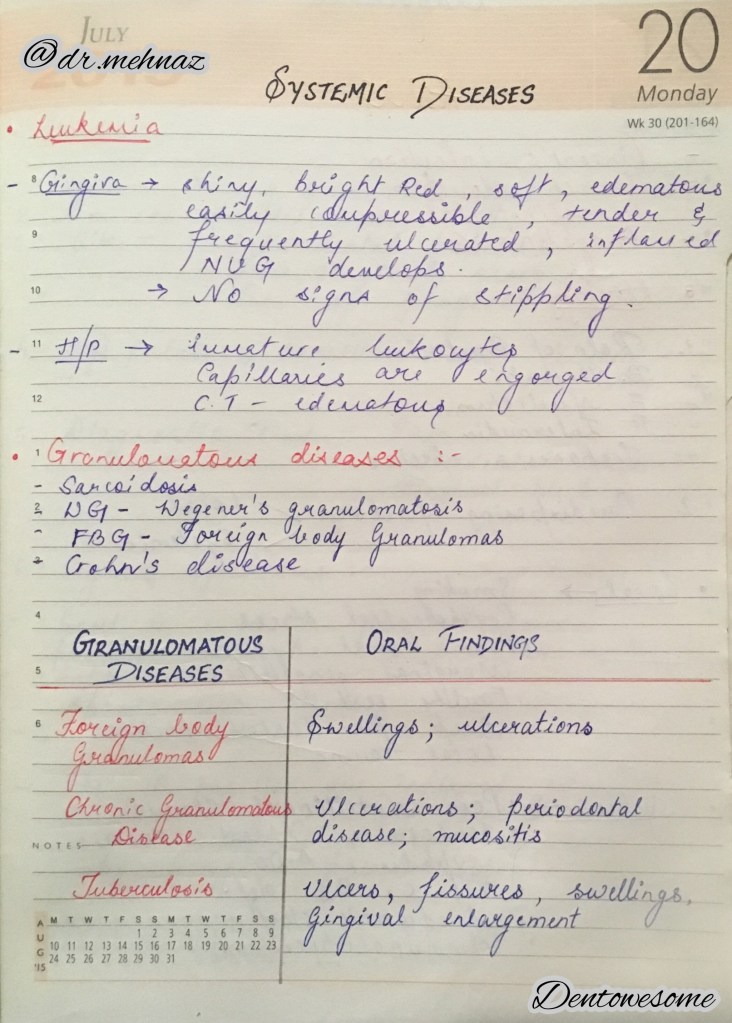
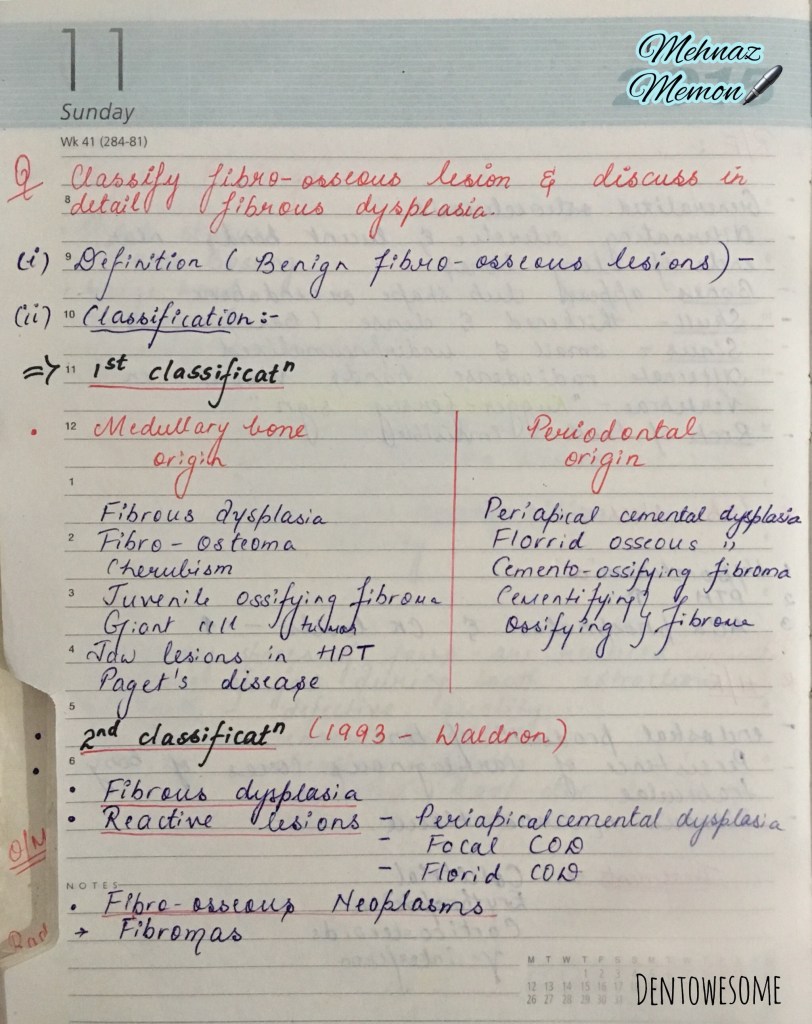
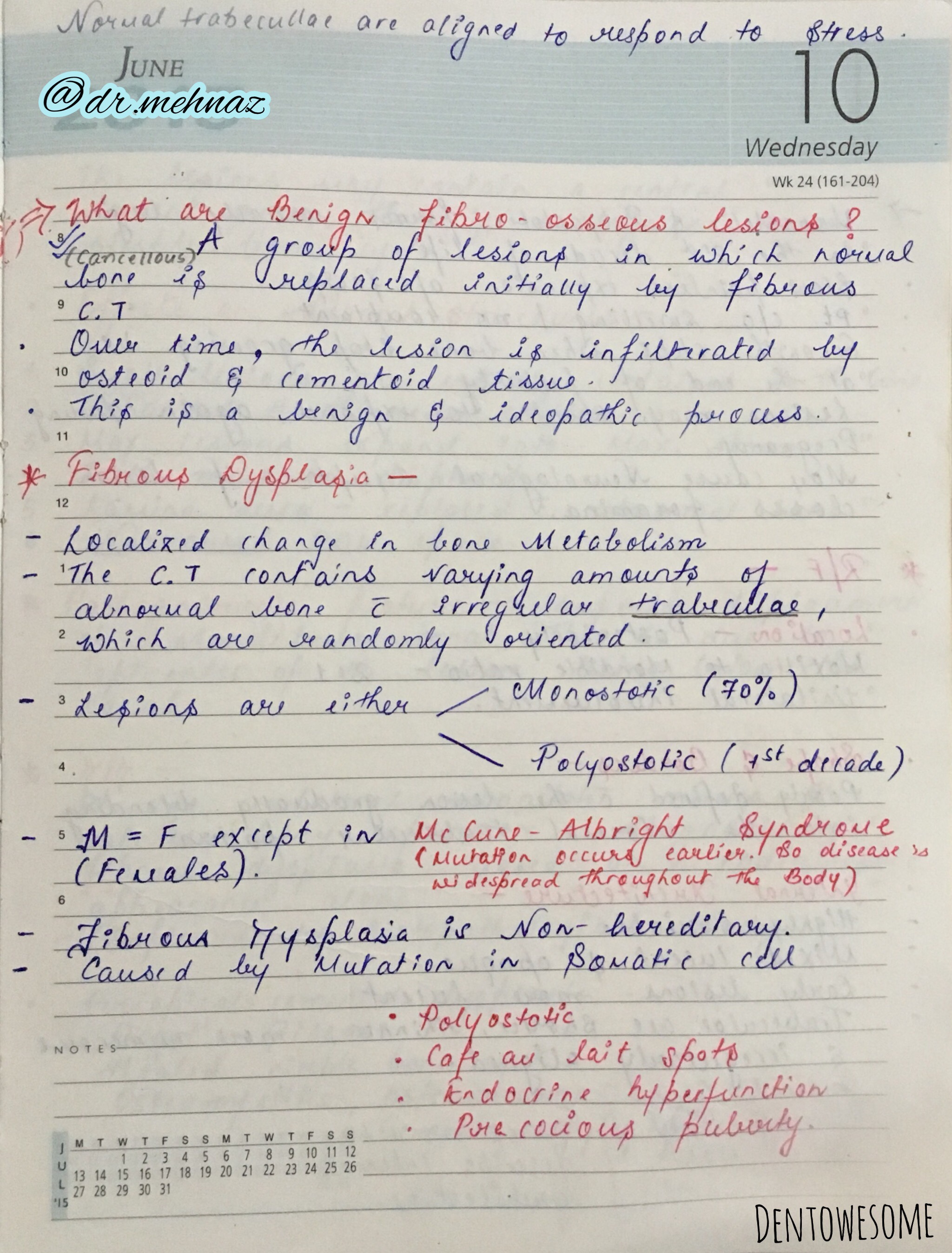
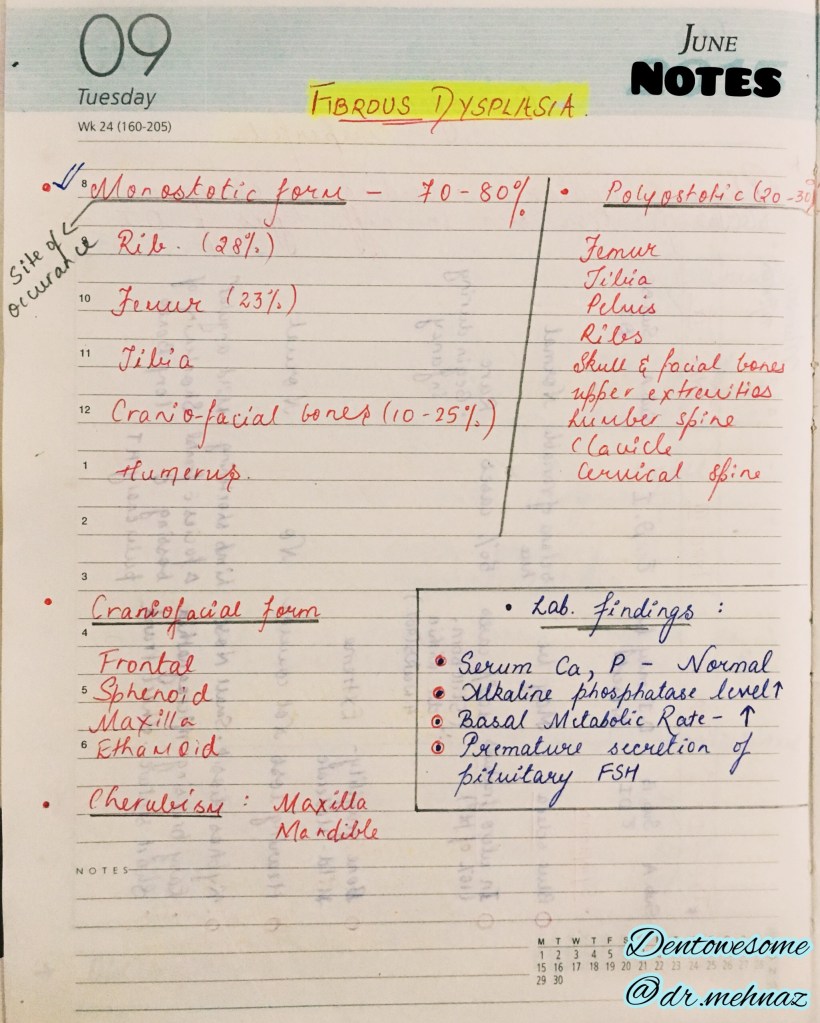
a. Fibromas

Page 1 of 3
Read More »
Nancy 13th edition

Source: Internet






References: Essentials Of Periodontology by S Sahitya Reddy; Shafer’s Oral Pathology; Carranza’s clinical periodontology; Internet
Dr. Mehnaz Memon🖊
