1. How did your journey in the dental profession begin, and what were the milestones that shaped it?
From the very beginning, I knew I didn’t just want to be a dentist — I wanted to be a holistic dentist. For me, that meant stepping into every kind of setup possible. I’ve worked in super glam, high-end clinics where patient detailing and experience matter the most, in fast-paced corporate chains where efficiency and systems rule, and in CGHS/government setups where limited resources challenge your creativity and compassion.
Each of these experiences shaped me in unique ways — teaching me empathy, precision, and adaptability — lessons I carry into my practice every single day.
2. What inspires you to stay passionate and committed to dentistry, even during challenging times?
People inspire me. Over the years, I’ve noticed a beautiful shift — patients today are genuinely curious about their smiles. They ask questions, they care about their oral health, and they’re invested in improving it. Seeing how a small change — sometimes as simple as aligning a tooth or improving a shade — can completely transform someone’s confidence is what keeps me going. And of course, dentistry allows me to be my own boss — a privilege that pushes me to stay committed and creative, even during tough days.
3. Who is your role model in dentistry, and how have they influenced your professional journey?
My biggest inspiration is Dr. Shruti from MAIDS. She’s done both her BDS and MDS there, and what amazes me most is her discipline. Even today — while managing family life and raising two kids — she studies for a few hours every single day. That level of dedication reminds me that dentistry isn’t a career you complete; it’s a lifelong learning journey. I aspire to bring that same philosophy to my practice — to always stay updated so my patients receive care that’s rooted in both compassion and the latest science.
4. How do you balance academics, work, and personal interests?
For me, balance isn’t optional — it’s essential. Dentistry can be intense, so I make sure to pause and recharge when needed. I’ve even taken two-month breaks between jobs just to travel, rest, and reset before starting fresh. Some people might think that’s unconventional, but that balance fuels my best work. When you’re happy and fulfilled outside the clinic, you naturally become a more patient, empathetic, and focused dentist inside it.
5. What advice would you give to dental students and young professionals?
The early stages can be tough — there’s little earning, lots of expenses, and often a sense of uncertainty. But don’t let that phase define you. Use that time to learn, document, and grow. Keep updating your skills and build expertise in areas your peers might overlook. When you do that, you create your own niche — and patients will value that uniqueness. Remember, confidence comes from competence. Keep learning, and everything else will follow.
💎 A Smile That Reflects a Life Well-Lived
Dr Himani Hasaji’s story is more than a professional journey — it’s a lesson in purpose, balance, and evolution. She’s not just crafting smiles; she’s crafting a philosophy that blends science, art, and humanity.
From wax carvings to real-life artistry — Dr Janhavi Bangar’s journey through dentistry is a story of growth, grit, and genuine passion. In this candid interview, she opens up about the milestones that shaped her, the mentors who molded her mindset, and the balance between precision and play in her life as a young dentist.
Beginnings: Finding Meaning in Every Milestone
1️⃣ Can you share how your path in the dental profession began and the key milestones that shaped it?
Honestly, my path started a bit like a wax carving — rough at the edges but shaping into something meaningful. One of my earliest “wow” moments was assisting in an implant surgery. I remember thinking, “We literally put screws into bone and call it art — this is wild and fascinating!” Another turning point was getting 73% in my first year. It wasn’t just a grade; it was proof that I could actually be good at this. Then came the decision to pursue masters and later my internship at GDC Mumbai as an extern — that’s where it clicked: Yes, MDS is my road. Each of these milestones felt like building blocks, shaping not just my career, but also my confidence in it.
Passion That Persists: Finding Joy in Every Smile
2️⃣ What inspires you to stay passionate and committed to dentistry, even during challenging times?
For me, it’s simple — dentistry gives me the rare privilege of seeing the impact of my work almost instantly. A patient walks in hiding their smile, and after treatment, they walk out grinning ear to ear. That transformation, that joy — it’s addictive. It reminds me every day why I chose this. Sure, there are tough times — long hours, endless reading, sometimes frustrating cases — but then I remember what Dr. G.V. Black, the father of modern dentistry, once said: “The professional man has no right to be other than a continuous student.” So even when I’m tired, the idea that I’m constantly learning while helping someone regain their smile keeps me moving.
Mentorship and Inspiration: The People Behind the Progress
3️⃣ Who is your role model in the dental field and how has this person influenced your approach to patient care, academics, or professional growth?
It’s impossible to pick just one — every mentor I’ve had has shaped me in some way, like different teeth in the same arch, each serving its unique function.
Dr. Swati Pustake has been my guiding light. Her calmness in difficult situations taught me lessons that no textbook ever could.
Dr. Bikash Pattnaik inspires me daily with his combination of brilliance and humility — he’s living proof that academics, health, and fun can coexist beautifully.
Dr. Komal Majumdar and Dr. Moez are orators who can hold a room’s attention like no one else — they’ve shown me that communication is just as vital as clinical skill.
Together, they’ve shaped my philosophy: dentistry isn’t just about perfecting your hand skills — it’s about shaping your mindset, resilience, and ability to connect with people.
Balance Beyond the Clinic: Living Life Fully
4️⃣ Could you discuss the strategies you use to manage academic responsibilities alongside your personal interests or hobbies?
My strategy is simple: dentistry is a part of my life, not my entire life. On most days, I’m the dedicated student, clinician, and resident — working 12–13 hours if needed. But I’ve also promised myself that I won’t lose out on living. That one free day or Sunday, I make sure I really live — whether it’s brunch with friends, a trek, volleyball, painting, creating content, or even participating in college fests and fashion shows. After all, what’s the point of being a prosthodontist if you don’t know how to fix the “missing tooth” of fun in your own life? As the saying goes, “Don’t get so busy making a living that you forget to make a life.”
Words of Wisdom: Lessons for Aspiring Dentists
5️⃣ What advice would you give to current dental students and aspiring dentists?
My biggest advice is have clear intent, stronger than your luting cement. Dentistry is demanding, yes, but if your values are strong ,whether it’s honesty in studies, compassion in patient care, or integrity in friendships , you’ll stand strong no matter what. Patients can always sense genuine energy; if you’re invested in them, half the treatment is already successful.
And don’t forget to have fun along the way , pursue the things you’re passionate about outside dentistry too, because that joy will reflect in the kind of dentist you become. Like Dr. William Osler said: “The good physician treats the disease; the great physician treats the patient who has the disease.” I’d like to believe the same applies to us: “The good dentist restores the tooth; the great dentist restores the smile — and the person behind it.”
🎙️ From Scalpel to Spotlight: A Candid Chat with Dr. Karthik
MDS Periodontology | Educator | Host of the India’s Most Famous Dentist Podcast | Winner of the Golden Mic Award for Best Dental Podcast
If you’ve scrolled through dental Instagram lately or tuned into any student-friendly podcast, chances are you’ve come across Dr. Karthik. Known for his calm voice, creative visuals, and deep conversations on the India’s Most Famous Dentist Podcast, he’s someone who makes dentistry feel a little less intimidating—and a lot more inspiring.
We caught up with him to talk about his journey, his motivation, and his advice for the next generation of dentists.
🦷 Q1. So, Dr. Karthik—where did it all begin? What pulled you into dentistry?
I think I was always inclined toward the artistic side of things. Even before dentistry, I’ve had this natural urge to focus on precision and the smaller details – whether it was sketching, filmmaking, or editing. I’ve always believed that creativity and precision go hand in hand. Those who’ve seen my videos or podcast visuals probably notice that – my team and I put a lot of thought into how things look and feel, because I think dentistry is also an art form.
So for me, it wasn’t a trickle-down choice or a backup plan. Dentistry – and especially periodontics matched that part of me that loves design, structure, and creating something that lasts. It gave me a space where art, science, and communication meet – and that’s what continues to drive me every day.
I think I’ve always had this curiosity to understand how things work – especially the human body. During my early years, I could spend hours with anatomy, physiology, pharmacology, or medicine textbooks. They completely fed that curiosity of knowing how the body is designed and how it functions.
But soon, I realized that knowing wasn’t enough – I had this restless urge to do something with that knowledge. I’m a very hands-on, high-energy person, so I naturally gravitated toward dentistry. The pre-clinical labs – wax patterns, tooth carvings, crown preparations – all of that gave me a creative outlet.
Then came the clinical years – Conservative Dentistry, Prosthodontics, Periodontics, Oral Surgery, Orthodontics, Oral Medicine and Radiology, Pedodontics and Public health Dentistry – and that’s when I really found my rhythm. Periodontics especially connected deeply with me because it’s where precision meets biology. You can see what you’re working on, and every millimetre matters – it matched my personality perfectly.
Over time, those experiences shaped how I approach not just treatment, but also communication whether it’s through my podcast, my content, or my work with students and clinicians. Each phase was a milestone that built both the clinician and the creator in me.
💪 Q2. What keeps you going when the days get tough?
I always start with history. When you stay connected to your roots, it gives you a deep sense of value for what you have today.
If you look back, the pioneers of dentistry – the scientists, clinicians, researchers – they built this field with almost no resources. They worked for patient welfare, comfort, accessibility, and affordability, long before we had the kind of technology and conveniences we rely on now.
That perspective really keeps me grounded. Whenever I go through a challenging phase, I remind myself – we are walking on a path that so many before us have built through pure dedication and passion. All we need to do is keep that spirit alive.
In fact, this is something I often tell students: value what you have today, because it’s the result of decades of evolution. On my podcast, we’ve done a few episodes on the History of Dentistry -featuring experts and curators from dental museums, and even conversations on how dentistry was practiced in the 1950s compared to now. Those episodes truly help you appreciate how far we’ve come as a profession.
So, whenever I feel tired or demotivated, revisiting that history – the legacy of our field – reignites my purpose. It reminds me that being part of dentistry itself is a privilege.
🌟 Q3. Do you have a role model—or many?
Well, for me, it’s hard to name just one person as a role model. I’ve been fortunate to meet and learn from so many incredible dentists throughout my journey.
During my undergraduate days, I was very active in both curricular and extracurricular activities -which gave me the chance to interact with dentists who were doing outstanding work, nationally and internationally. Then in post-graduation, I think I must have attended over fifty national and international dental education programs. Each of those experiences connected me with mentors, clinicians, and researchers who were masters in their domains.
So for me, keeping just one role model has always been difficult. I try to stay alert and absorb something valuable from everyone I meet – because sometimes a small line of advice from an experienced dentist can be worth more than what you find in textbooks.
And on top of that, my podcast journey has been a huge source of learning. Every guest I’ve hosted – whether it’s Dr. Anuj Agarwal, Dr. Ashish Jain, Dr. Suresh Ludhwani, Dr. Moez Kahkiani, or someone like Dr. Sandesh Mayekar who’s contributed in all aspects – each of them has left a strong impression on me. I’ve learned a lot from their experiences, their perspectives, and even their attitude toward growth.
So, rather than one role model, I’d say I have many – and collectively, they keep me grounded, curious, and inspired to do better every day.
🎬 Q4. How do you juggle academics, practice, and content creation?
Yes, it has been challenging – but not because of lack of time or multitasking. The real challenge often comes from the mindset around us. Many people assume that if you’re doing something beyond your main work – like pursuing hobbies, content creation, or any parallel interest – you’re somehow not focused on your core field.
But that’s not true at all. That’s just a shallow perception. I genuinely believe that your hobbies and creative skills can strengthen your main profession, if you channel them in the right way. For me, filmmaking, editing, communication – all of these have actually helped me explain dentistry better and connect with people more effectively.
I once asked a very well-known businessman of our country – whose discussion will soon be out on my page – about how he managed to stay focused amid so much noise. He gave a brilliant analogy. He said, ‘In your generation, you have noise-cancellation headphones. I naturally developed the ability to switch my ears on and off – to only listen to what truly matters.’ That line really stayed with me.
And honestly, that’s the key. You have to learn to tune out the outer noise. Focus only on what adds value. Everyone has immense creativity, energy, and potential – it’s just the distractions that pull you back. If I have to put it as a strategy – I’d say: eat, sleep, do one thing for yourself, one for your family, and one for society – and repeat.
🪥 Q5. What’s your advice for dental students and young clinicians?
My advice would be simple – don’t just study dentistry, live it. Dentistry today isn’t only about clinical skills; it’s about how you think, how you communicate, and how you keep learning every single day. Be curious – not just about treatments, but about people. Understand your patients, listen to them, and value the privilege of being trusted with their health.
Secondly, don’t compare your journey with others. Everyone’s timeline is different. Some people bloom early, some take time – and both are absolutely fine. What matters is that you stay consistent and keep improving your craft.
Also, take your creative side seriously. Whether it’s content creation, design, research, or patient communication – your ideas and hobbies can actually strengthen the field if you channel them with purpose.
And lastly, always remember – this profession was built on service and sincerity. So stay grounded, stay ethical, and contribute back in your own way.
If I had to sum it up in one line, I’d say: Keep learning, stay curious, do good work – and life will give you more than you ever expected.
And yes, I’d genuinely encourage students and young dentists to watch my show – the guests we’ve had share incredible insights that can really shape how you look at the profession. And feel free to connect with me if you ever want to discuss ideas, to learn, or just want to talk – I’m always happy to interact with passionate minds. Thank you.
🎧 Before We Sign Off…
Dr. Karthik’s journey reminds us that being a dentist isn’t only about perfect crowns or precise sutures—it’s about storytelling, service, and staying curious.
If you’re ever in need of a dose of inspiration, tune in to his award-winning with India’s Most Famous Dentist (IMFD) Podcast—a space where students, clinicians, and even parents discover what the world of dentistry really looks like.
If bones could talk, they’d probably say, “Hey, stop pulling me!” But in the world of distraction osteogenesis (DO), that’s exactly what we do—intentionally stretch bone tissue to create new growth. Think of it as the orthodontic equivalent of a yoga instructor telling your jaw to lengthen and breathe.
While orthognathic surgery has been the gold standard for skeletal corrections, DO has stepped in as the cool new kid, especially for cases that were once deemed untreatable. But is it really the superior method, or just a fancier way to move bones? Let’s break it down.
Since its first craniofacial application by McCarthy et al. in 1992, DO has come a long way from being an experimental idea to a widely used technique for maxillary and mandibular expansion. But, like any orthodontic superhero, it comes with its strengths, weaknesses, and a history of trial-and-error that reads like a medical thriller.
The Origins: From Soviet Leg Braces to Jawline Makeovers
DO owes its roots (pun intended) to Ilizarov’s principles—a Russian orthopedic surgeon who figured out that bone can be stretched and tricked into regenerating. What started as a method for limb lengthening soon found its way into orthodontics when McCarthy et al. used it to lengthen hypoplastic mandibles in children.
Once researchers saw potential in midface and maxillary distraction, it became a game-changer for patients with clefts and severe maxillary hypoplasia—especially when traditional orthognathic surgery wasn’t an ideal option.
With miniature distraction devices, rigid external distraction (RED) systems, and intraoral appliances, the orthodontic world saw an explosion (well, controlled expansion) of techniques:
🔹 Cohen et al. (1997) – Introduced maxillary distraction in young children. 🔹 Polley & Figueroa (1997) – Used the RED device to treat severe maxillary hypoplasia. 🔹 Molina et al. (1998) – Tried a mix of facial masks and intraoral appliances for mixed dentition cases.
So, Does It Work? The Numbers Speak!
Swennen et al. (2001) reviewed 16 studies spanning 33 years (1966-1999) and found that maxillary advancements ranged from 1 mm to 17 mm. Not bad for a non-surgical approach, right?
Well, not so fast—relapse was reported in 50.4% of cases. That’s like getting a six-pack after months of workouts only for it to disappear when you eat one slice of pizza.
Rachmiel et al. (2005) reported stable results in 12 cleft patients after two years, showing that maxillary length (Condylion to A point) held its ground. But Krimmel et al. (2005) later threw a wrench into that optimism, noting a decrease in SNA and ANB angles just one year after distraction.
Cheung & Chua (2006) conducted a meta-analysis of 26 studies (1966-2003) on 276 cleft patients, revealing:
📌 Most maxillary advancements were between 5-9 mm. 📌 External distractors (68.8%) were more common than internal distractors (2.17%) and facial masks (25.72%). 📌 Maxillary relapse? 5.56% within two years—but only one study provided actual numbers.
One thing is clear: distraction osteogenesis works, but long-term stability is still a mixed bag.
The Study: Six Patients, One Mission—Expand That Maxilla!
Meet our VIPs: six Chinese patients (3 boys, 3 girls, average age 10.5 years), all of whom had: ✔ Cleft lip and palate (two unilateral, four bilateral) ✔ Primary lip and palate repair in infancy ✔ Anteroposterior maxillary hypoplasia (aka, their upper jaw was slacking) ✔ Class III malocclusion with a negative overjet (translation: their lower teeth were winning a battle they shouldn’t even be fighting)
These kids weren’t just getting braces—they were about to experience controlled bone expansion, courtesy of the Rigid External Distraction (RED) device.
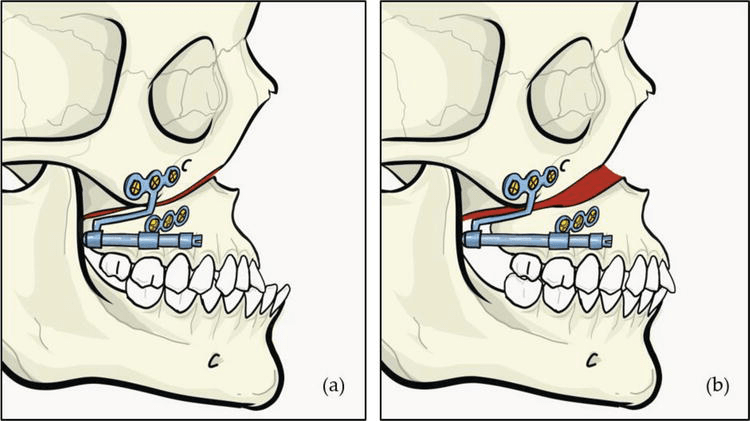
1️⃣ Pre-Orthodontic Preparation – Because even bone stretching needs a good warm-up. 2️⃣ Complete High Le Fort I Osteotomy – A fancy way of saying, “Let’s surgically cut the upper jaw so we can move it.” where the maxilla was delicately detached with septal and pterygomaxillary disjunction. (Translation: we made it mobile but still attached—think of it as unlocking a door, not knocking it down.) 3️⃣ RED Device Installation – Think of this as the orthodontic version of a headgear, but instead of just pushing teeth, it’s stretching the entire upper jaw. 4️⃣ Latency Period (5 Days) – Let the jaw marinate before we start stretching it. 5️⃣ Active Distraction (1 mm/day) – The screws on the RED device were adjusted daily to pull the maxilla forward. (It’s like a gym for your bones—except you don’t have to do the work; your jaw does.) 6️⃣ Overcorrection Achieved! 🎉 – Because we know relapse is real, we stretched the maxilla a little extra to compensate for future setbacks. 7️⃣ Consolidation (6-8 Weeks) – The RED device stayed put to let the new bone solidify. 8️⃣ Device Removal & Orthodontics – After the expansion was done, the real party started: braces to fine-tune everything.
The study wasn’t just about making kids look less Class III—it was about proving that DO actually works (and hopefully, stays that way). Here’s how they did it:
📸 Lateral Cephalographs were taken at four key points: 🔹 T0 (Before Distraction) – “This is your jaw on cleft-induced hypoplasia.” 🔹 T1 (Immediately After Distraction) – “Congratulations, your maxilla has entered the chat.” 🔹 T2 (6 Months Later) – “Let’s see if your jaw likes its new position.” 🔹 T3 (1+ Year Later) – “Did it stay put, or did it sneak back?”
Instead of using simple before-and-after pictures (this isn’t a weight loss commercial), the researchers mapped out skeletal and dental landmark positions using a cranial base reference system.
How, you ask?
🔹 First, skeletal landmarks were pinpointed on the T0 cephalogram. 🔹 Then, these landmarks were transferred onto T1, T2, and T3 cephalograms using a best-fit method—aligning surrounding bone structures and trabecular patterns (Huang & Ross, 1982). 🔹 To keep things precise, an x-y coordinate system was created:
Y-axis: A perpendicular line intersecting the X-axis at sella 🔹 This coordinate system was then transferred onto each cephalogram for standardized measurements.
X-axis: Drawn 7° below the sella-nasion plane
Key Takeaways
✅ Overjet increased (yay, no more Class III woes!). ✅ Overbite decreased—except for our rebellious Case 5. ✅ Maxilla went forward (woo-hoo!) but then took a casual retreat backward over a year (boo!). ✅ Some vertical movement—first up, then down (the maxilla, not our enthusiasm). ✅ Teeth tagged along for the ride, moving anteriorly and inferiorly. ✅ Relapse? Oh yeah—about 9.6% at 6 months, increasing to 24.5% by a year.
Orthodontic treatment often requires space creation to align teeth properly. One effective way to achieve this is through molar distalization—moving the upper first molars backward to make room for crowding or to correct bite discrepancies. Traditionally, orthodontists have relied on headgear, Class II elastics, and removable appliances, all of which require patient compliance (and we all know how reliable that is! 🙄).
But what if there was a more predictable, fixed alternative?
Enter the Jones Jig Appliance—a fixed, non-compliance-based distalizing appliance designed to move molars efficiently without relying on patient effort.
How Does the Jones Jig Work?
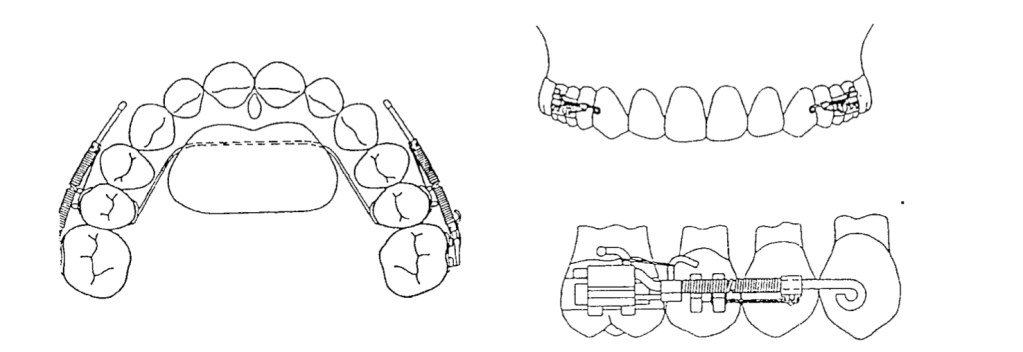
✔ Palatal Button – A 0.5-inch diameter acrylic button, anchored to the maxillary second premolars using a 0.036-inch stainless steel wire for stability. ✔ Jones Jig Arms – One arm fits into the 0.045-inch headgear tube, while the other fits into the slot of the first molar band. ✔ Nickel-Titanium Spring – A 0.040-inch coil spring delivers a controlled force of 70-75 g to push the molars backward.
Once the Jones Jig is cemented, it is activated by tying the activation loop with a 0.010-inch ligature off the bracket of the anchoring tooth. This ensures continuous force application.
The coils are then reactivated every 4 to 5 weeks until the desired molar movement is achieved.
Once activated, the appliance applies a gentle but continuous distal force on the upper first molars, moving them backward over time. The best part? Since it’s fixed, patients don’t have to remember to wear it, making treatment more reliable.
Advantages of the Jones Jig
✅ No Patient Compliance Needed – Unlike headgear, patients don’t have to wear or adjust it. ✅ Continuous Force Application – The coil spring ensures a steady force for predictable movement. ✅ Faster Treatment Time – Studies show that molars can be distalized in 4-6 months.
While the Jones Jig is highly effective, it does come with some considerations: 🔹 Molar Tipping – Instead of bodily movement, molars may tip distally, requiring additional mechanics for uprighting. 🔹 Anchorage Loss – The anterior teeth may shift forward slightly, which may need to be controlled with TADs (temporary anchorage devices) or a transpalatal arch (TPA).
Does the Eruption of Second Molars Affect Treatment?
When using the Jones Jig Appliance for molar distalization, orthodontists must consider various factors that can influence treatment outcomes. One key question is: Does the eruption of second molars impact molar movement and anchorage loss?
A study evaluating 72 patients explored this question by comparing cases with erupted vs. unerupted maxillary second molars to determine how they affected the type and amount of molar movement and anchorage loss.
Study Findings: Second Molar Eruption and Its Effects
Researchers divided the patients into two groups:
Group
Condition of Second Molars
Key Observations
Group 1 (28 patients)
Unerupted second molars (below the cementoenamel junction of the first molar)
Less anchorage loss in premolars and incisors, potentially more controlled molar movement.
Group 2 (44 patients)
Erupted second molars (not banded or bonded)
More anchorage loss observed, possibly due to resistance from the second molars.
The presence or absence of second molars plays a significant role in the effectiveness of molar distalization. Patients with unerupted second molars may experience better molar movement with less anchorage loss, while those with erupted second molars may require additional anchorage support. In cases with erupted second molars, additional anchorage reinforcement (e.g., TADs or a transpalatal arch) may be necessary to prevent undesired movement.
Study Findings: How Far Did Those Molars Go?
A retrospective study of 72 patients using the Jones Jig showed:
Tooth Movement
Mean Change
Tipping Angle
Comparison to Other Appliances
Maxillary First Molar
2.51 mm distal movement
7.53° distal tipping (meaning they didn’t just move—they leaned back like someone dodging responsibility. 😅)
Similar to Herbst, Wilson Mechanics, and Pendulum Appliance 📏
Maxillary Second Molar
1.79 mm distal movement (Not as much as the first molar, but still making progress! 🔄)
8.03° distal tipping (tipped even more than first molars)
0.71 mm extrusion observed 📉 (suggests that second molars are like that one friend who always stands out in group photos. 📸)
Overjet
Increased 0.45 mm
If necessary, J-hook headgear or Class II elastics can help maintain anchorage.
2.21° incisor proclination
(much less than the 6° seen in other studies. So, while there’s some flaring, it’s not enough to make your patient look like Bugs Bunny. 🐰)
Less flaring than with Pendulum & Repelling Magnets 😎
Less than the 1.30 mm increase seen with the Pendulum appliance and the 1.60 mm increase with repelling magnets.
Overbite
Decreased 1.28 mm
—
Improved vertical control compared to other appliances 📊
Anchorage Control: Because We Don’t Want Molar Tipping Running the Show
Distalizing molars is great, but uncontrolled tipping? Not so much. Here’s where anchorage control steps in like a responsible chaperone at a high school dance.
✅ Use a Nance holding arch, utility archwire, or stopped archwire to keep those molars in check. ✅ Short Class II elastics can help move the premolars and incisors back once the molars are in position. ✅ J-hook headgear can reinforce anchorage (for the brave souls who still prescribe it).
Molar Extrusion: Is It a Big Deal?
One concern with distalization is molar extrusion—but does the Jones Jig make teeth “float away”? Not really.
🔹 Jones Jig Patients:
Males:3.17 ± 1.79 mm of extrusion
Females:1.33 ± 1.38 mm of extrusion
🔹 Untreated Class I Patients (for comparison):
Males:4.1 ± 3.1 mm
Females:1.9 ± 2.2 mm
📌 Takeaway? The extrusion in Jones Jig patients is within normal growth changes. So, unless your patient is trying to float their molars into the stratosphere, this isn’t a major concern. 🚀
Jones Jig vs. Headgear: Any Real Difference?
The study found no statistically significant differences between the Jones Jig group and a matched Headgear groupwhen evaluating:
✅ Maxillary first molar position ✅ Maxillary central incisor angulation ✅ Linear position of incisors ✅ Overjet & Overbite changes
So, if you’re an orthodontist who loves avoiding unnecessary patient lectures about compliance, the Jones Jig might be your new best friend. 🎉
Treatment Comparison: Who Wins?
Treatment Modality
Patient Compliance Needed?
Molar Distalization (mm)
Overjet Change (mm)
Overbite Change (mm)
Jones Jig Appliance
❌ No compliance needed
2.51 mm
+0.45 mm
-1.28 mm
Cervical Headgear
✅ Requires compliance 😬
2.50 mm
+0.40 mm
-1.30 mm
Class II Elastics
✅ Requires compliance 🙄
Varies (depends on use)
Greater risk of overjet increase
Less predictable molar control
📌 Takeaway? The Jones Jig does everything headgear does—without the compliance drama. It’s like getting straight A’s without ever studying (if only life worked that way 😆).
Final Verdict: Is the Jones Jig Worth It?
✔ YES! If you want a fixed, predictable, non-compliance-dependent way to correct Class II malocclusions, the Jones Jig is a great choice.
✔ Same results as headgear—without the teenage rebellion.
✔ Minimal anchorage loss compared to other distalization appliances (no crazy overjet increase).
✔ Less annoying for patients = less annoying for you. 😆
Promote beneficial dentoskeletal changes during growth periods (Bell, 1982).
Posterior cross-bites develop early and are not self-correcting (Moyers & Jay, 1959; Thilander et al., 1984).
Orthodontic Response to Expansion
Initial response completed within a week (Storey, 1973; Cotton, 1978; Hicks, 1978).
Subsequent movements occur as compressed buccal alveolar plate resorbs at the root-periodontal interface due to continued force (Storey, 1973).
Orthopaedic Effects of Expansion
Sufficient transverse forces can overcome bioelastic strength of sutural elements, causing:
Orthopaedic separation of maxillary segments (Storey, 1973; Chaconas & de Alba y Levy, 1977; Cotton, 1978; Hicks, 1978).
Palatal segment repositioning continues until force is reduced below sutural tensile strength.
Stabilization involves reorganization and remodeling of sutural connective and osseous tissues (Storey, 1973; Ekstrom et al., 1977).
Increased Maxillary Arch Width
Linked to orthodontic and/or orthopaedic effects of expansion (Ficarelli, 1978; Moyers, 1984).
Initial changes involve lateral tipping of posterior maxillary teeth due to compression and stretching of periodontal and palatal soft tissues.
Midpalatal Sutural Opening and Maxillary Displacement
Expansion leads to:
Downward and forward displacement of the maxilla with bite opening (Haas, 1961).
Downward and backward rotation of the mandible, increasing the vertical dimension of the lower face (Haas, 1970).
Subsequent recovery of mandibular posture noted in most cases (Wertz, 1970).
Rate of Expansion and Dental Arch Width Increase
Rapid Maxillary Expansion (Krebs, 1959, 1964):
Subjects aged 8–19 years showed an average dental arch increase of 6.0 mm (range: 0.5–10.3 mm).
Skeletal changes accounted for:
~50% of the arch width increase in 8–12-year-olds.
~33% of the increase in 13–19-year-olds.
Slow Maxillary Expansion (Hicks, 1978):
Subjects aged 10–15 years showed a dental arch width increase of 3.8–8.7 mm.
Skeletal response ranged from 16–30%, with lower skeletal response in older patients.
Buccal tipping of molars and skeletal segments contributed to arch width increase.
Asymmetrical angular changes between left and right molars and maxillary segments were observed.
Removable Plates and Sutural Growth (Skieller, 1964):
In subjects aged 6–14 years:
20% of dental arch widening was attributed to sutural growth.
Sutural growth rate during expansion was significantly greater than during follow-up, indicating stimulated growth during expansion.
Removable Plates and Sutural Growth (Skieller, 1964):
Study on 20 subjects aged 6–14 years:
20% of dental arch widening was attributed to sutural growth.
Growth rate at the mid-palatal suture was significantly higher during expansion compared to the follow-up period.
Suggests that sutural growth is stimulated during the expansion period.
Histologic Findings in Slow Expansion Procedures:
Sutural separation occurs at a controlled rate, maintaining tissue integrity during maxillary repositioning and remodeling (Storey, 1973; Ekstrom et al., 1977; Cotton, 1978).
Relapse Tendency During Post-Retention Period:
Relapse potential is reduced in slow expansion procedures due to:
Introduction Malocclusion, characterized by changes in teeth positioning and skeletal growth, represents a global public health concern.
Historical Context: Correction attempts date back to at least 1000 BC.
Prevalence: Class II malocclusion affects one-third of the population and is categorized as skeletal or dental in origin.
Etiology:
Only 20% of Class II Division 1 cases are due to maxillary protrusion.
The majority stem from mandibular retrusion.
This prevalence has led to the development of functional appliances aimed at stimulating mandibular growth. These devices are divided into removable and fixed functional appliances.
Fixed Functional Appliances
Types:
Rigid: Herbst appliance, MARA (Mandibular Advancement Repositioning Appliance).
Flexible: Jasper Jumper, Scandee tubular jumpers.
Hybrid: Forsus Fatigue Resistant Device (FFRD).
Forsus Fatigue Resistant Device (FFRD):
A telescoping spring mechanism for Class II correction.
Provides moderate patient tolerance with initial discomfort that subsides over time.
PowerScope Appliance:
Latest addition, introduced by Dr. Andy Hayes in 2016 in collaboration with American Orthodontics.
Features a telescopic mechanism with a nickel-titanium (NiTi) spring delivering 260 g constant force.
Designed as a preassembled, one-size-fits-all appliance for easy chairside application.
Study Rationale While Forsus FRD is extensively studied, limited literature evaluates and compares the skeletal, dental, and soft tissue effects of PowerScope. This study bridges that gap by conducting a cephalometric evaluation and comparison of these two fixed functional appliances.
Both appliances are effective in correcting Class II discrepancies caused by retrognathic mandibles. However:
Forsus FRD is superior in achieving skeletal changes, particularly maxillary retrusion and mandibular advancement.
PowerScope shows more pronounced effects on dentoalveolar and soft tissue parameters, especially upper incisor inclination correction and facial convexity improvement.
Molar distalization is a crucial technique in orthodontics, particularly for patients with Class II malocclusion. Thanks to advancements in biomechanics, materials, and technology, orthodontists now have access to a variety of intramaxillary intraoral appliances that can apply light, continuous forces for effective molar distalization. These appliances have become a game-changer, providing us with more precise control and predictable results.
Types of Intramaxillary Appliances
The application of forces in molar distalization can come from two primary areas: the buccal or the palatal region. Depending on where the force is applied, appliances can be categorized into two broad groups:
Buccal Force Application: These appliances apply force from the outside of the dental arch.
Palatal Force Application: These appliances exert force from the roof of the mouth.
Additionally, the force mechanisms can be divided into two categories:
Friction-Free Mechanism: This type involves appliances like the pendulum, which are designed to move the molars without causing significant friction.
Sliding Mechanism: Appliances like nickel-titanium (NiTi) coil springs use a sliding mechanism to apply force, creating a more dynamic force delivery system.
Each of these appliance types has its own set of advantages and drawbacks, and comparing their efficiency in achieving molar distalization is key to making evidence-based treatment decisions. However, due to the limited number of randomized clinical trials, a meta-analysis is often not possible. That said, a comprehensive analysis of existing studies can still offer valuable insights into how these appliances work.
Treatment Outcomes: Overall Effects
When all intramaxillary appliances were considered together, some general findings emerged:
First Molar Movement: On average, first molars moved 2.9 mm distally, but this came with a 5.4° of distal tipping.
Incisor Movement: The incisors shifted mesially by 1.8 mm with 3.6° of mesial tipping.
Premolar Movement: Premolars showed a mesial shift of 1.7 mm, though tipping was less pronounced.
Vertical movements were generally extrusive for incisors and premolars, with incisors showing an average extrusion of 0.4 mm and premolars 1.1 mm. Interestingly, molar vertical movements were not statistically significant, indicating that the main effect on molars was distal movement and tipping rather than vertical displacement.
Treatment Effects: Buccal vs. Palatal Appliances
Now, let’s delve into the specific effects of buccal and palatal appliances. These results highlight the different ways these appliances move teeth:
Buccal Appliances:
Molar Movement: Molar distal movement was 2.6 mm, with a more significant tipping of 8.3°.
Incisor Movement: Incisors moved mesially by 1.9 mm with 5.0° of mesial tipping.
Premolar Movement: Premolars demonstrated a 2.0 mm mesial shift, accompanied by 7.0° of mesial tipping.
Vertical Movement: Premolars showed a slight extrusion of 0.7 mm, while incisors had a more modest extrusion of 0.2 mm.
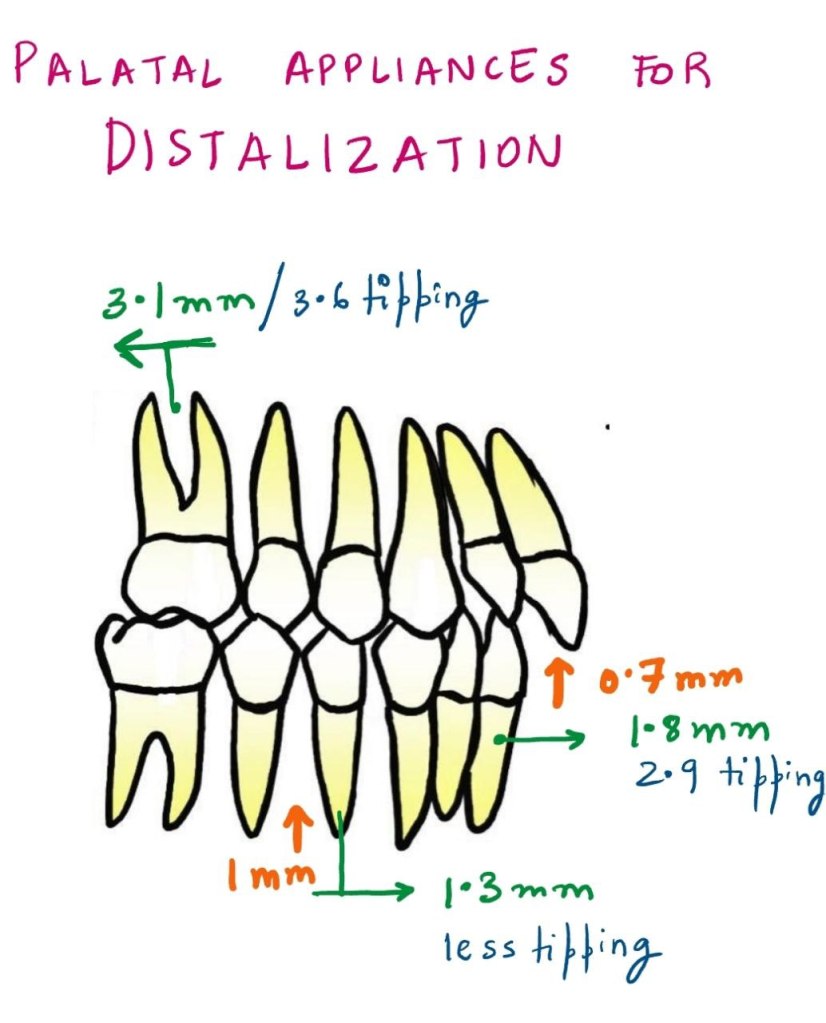
Palatal Appliances:
Molar Movement: Molar distalization was slightly more pronounced, with 3.1 mm of movement and 3.6° of tipping.
Incisor Movement: Incisors exhibited a mesial shift of 1.8 mm with 2.9° of mesial tipping.
Premolar Movement: Premolars moved mesially by 1.3 mm with less tipping than buccal appliances.
Vertical Movement: The extrusion for incisors was 0.7 mm, and premolars showed an extrusion of 1.0 mm.
Molar Distalization and Anchorage Loss
The primary effect of noncompliance intramaxillary appliances is molar distalization, which is typically achieved through a combination of crown distal movement and tipping. While distalization is the goal, a common side effect observed is loss of anchorage. This loss can be seen in the mesial movements and extrusions of incisors and premolars.
Key Findings:
Molars: Show a combination of distal crown movement and distal tipping.
Incisors: Exhibit mesial movement, tipping, and extrusion.
Premolars: Display mesial crown movement and extrusion.
As with any treatment modality, careful planning is required to manage these unintended side effects and achieve the best possible clinical outcomes.
Buccal vs. Palatal Appliances: Tipping and Force Mechanics
One interesting observation in the study was the difference in tipping effects between buccal and palatal acting appliances. Palatal appliances consistently resulted in less tipping of teeth compared to buccal appliances, as indicated by the non-overlapping confidence intervals.
Why the Difference?
The key reason for this difference lies in the moment arm of the force. In palatal appliances, the line of action of the force is closer to the center of resistance of the tooth, leading to less tipping and more controlled molar movement.
Table 1: Comparison of Tipping between Buccal and Palatal Appliances
Appliance Type
Molars Distal Movement (mm)
Molars Tipping (°)
Incisor Mesial Movement (mm)
Incisor Tipping (°)
Premolar Mesial Movement (mm)
Premolar Tipping (°)
Buccal Appliances
2.6
8.3
1.9
5.0
2.0
7.0
Palatal Appliances
3.1
3.6
1.8
2.9
1.3
3.0
This table highlights the greater tipping observed with buccal appliances compared to palatal appliances, as well as the differences in molar distalization and mesial movement of incisors and premolars.
The Nance Button: Anchorage Considerations
Another point of discussion is the use of the Nance button to reinforce anterior anchorage during molar distalization. While it can support anchorage to some extent, it does not provide absolute anchorage. This is because the Nance button, as part of the anchorage unit, cannot completely resist mesial forces during molar distalization. Clinically, this often results in an increased overjet and proclination of maxillary incisors.
Clinical Tip:
For patients already presenting with an increased overjet, orthodontists must proceed with caution when prescribing these appliances. These cases may require additional measures to control the overjet and manage incisor proclination.
The Pendulum Appliance: A Look at Tipping and Movement
The pendulum appliance, a popular friction-free appliance, was noted in the study to cause the greatest distal tipping of molars. However, this tipping was correlated with a larger amount of distal crown movement. Interestingly, this tipping can often be corrected with the use of molar uprighting bends.
Table 2: Molar Distalization and Tipping with the Pendulum Appliance
Movement Type
Molar Distal Movement (mm)
Molar Tipping (°)
Pendulum Appliance
3.4
9.0
This table shows that the pendulum appliance can achieve significant molar distalization but at the cost of increased tipping. These tipping movements can be addressed with molar uprighting bends, which can help reduce the tipping angle.
Factors Affecting Molar Distalization
Several factors can influence the effectiveness of molar distalization, including:
Teeth Used for Anchorage: Different anchorage setups can affect the extent of distal movement.
The Type of Appliance Used: Whether the appliance uses a sliding mechanism or a friction-free mechanism plays a role.
Patient Factors: Age, initial molar relationships, and the eruption of second and third molars all contribute to how effectively molars are distalized.
In studies that focus on growing patients, mean ages ranged from 11.2 to 14.9 years, which is crucial because the growth phase can significantly impact the effectiveness of treatment. For example, molar distalization is often more effective before the second molars have erupted. When second molars are erupted, more force may be required, and the treatment time may increase.
Table 3: Influence of Molar Eruption on Distalization Efficiency