Muhad Noorman P, Final year Team dentowesome.
CLASSIFICATIONS OF CLEFT LIP AND PALATE
Davis & Ritchie classification (1922)
Veau’s (1931)
Harkins and associates(1962)
Kernahan’s Classification (1971)
Spina (1974)
Tessiers’s Classification.
VEAU’S CLASSIFICATION
Group 1- Cleft of soft palate only
Group 2 – Cleft of hard and soft palate extending
no further extending than involving incisive foramen, (secondary palate only)
Group 3 – Complete unilateral cleft, extending from uvula
to incisive foramen in the midline, then deviating the one side and usually extending through the alevolus at the position of the future lateral incisor
Group 4- Complete bilateral cleft, extending forward through incisive foramen to alevolus. Premaxilla, suspended from the nasal septum .
Asian population have highest frequency often
CLINICAL FEATURES:-
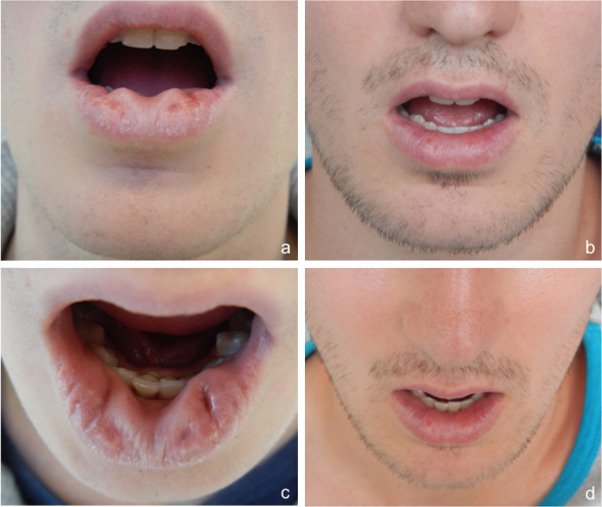
Incidence- 1in 500,With african population the lowest at 1in 250. Cleft lip alone more common in males. Isolated Cleft palate more common in female. 50% are syndromic, and are born with other congenital abnormalities.Cleft lip appear as unilateral / bi lateral. Line of cleft start on lateral part of upper lip and continues through philtrum of alveolus between lateral incisor and canine. When cleft lip continues from incisive foramen through palatal suture middle in palate,cleft lip with palate (unilateral/bilateral) present . . Cleft palate appears with involving soft palate only, involving uvula (bifid uvula),isolated cleft palate also.
.Patient have significant physical and physiological effects like, difficulty in eating and drinking with regurgitation of food to nose.
. Speech problem
. Ear infection: Malposition of Eustachian tubes result in middle ear infection
.Cosmetic deformities.
MANAGEMENT
Management of Cleft lip and palate require, multidisciplinary coordinated approach by specialist including maxillofacial surgeon, pediatric surgeon, anesthetist, Prosthodontist, Orthodontist, Speech pathologist, otolaryngology ,audiologist etc..
Management is aimed at closure and correction of lip and palate, secondary correction of palatal fistulae, orthodontic management of malocclusion, Orthognathic surgery, Rhinoplasty,and providing prosthesis for patients.
Pre operative criteria selected by physicians for surgery is Millards Rule of 10’s
1) 10lb weight
2) 10mg/l of haemoglobin
3) 10 weeks of age
SURGICAL MANAGEMENT
1) Primary : Closure of lip & palate
2) Secondary : Closure of palatal fistula, Pharygoplasty ,Bone grafting, orthodontic management Rhinoplasty and Scar revision.
Reference: Oral and Maxillofacial surgery, Balaaji. Textbook of general surgery for dental students, SRB