Before placement of rubber dam, following procedures should be done:
Thorough prophylaxis of the oral cavity.
Check contacts with dental floss.
Check for any rough contact areas.
Anesthetize the gingiva if required.
Rinse and dry the operated field.
Methods of Rubber Dam Placement.
Method I: Clamp placed before rubber dam
Select an appropriate clamp according to the tooth size.
Tie a floss to clamp bow and place clamp onto the tooth
Larger holes are required in this technique as rubber dam has to be stretched over the clamp. Usually two or three overlapping holes are made.
Stretching of the rubber dam over the clamps can be done in the following sequence:
– Stretch the rubber dam sheet over the clamp
– Then stretch the sheet over the buccal jaw and allow tosettle into place beneath that jaw
– Finally, the sheet is carried to palatal/lingual side andreleased. This method is mainly used in posterior teeth in both adults and children except third molar.
Method II: Placement of rubber dam and clamp together
Select an appropriate clamp according to tooth anatomy.
Tie a floss around the clamp and check the stability.
Punch the hole in rubber dam sheet.
Clamp is held with clamp forceps and its wings are insertedinto punched hole.
Both clamp and rubber dam are carried to the oral cavityand clamp is tensed to stretch the hole.
Both clamp and rubber dam is advanced over the crown.First, jaw of clamp is tilted to the lingual side to lie on thegingival margin of lingual side.
After this, jaw of the clamp is positioned on buccal side.
After seating the clamp, again check stability of clamp.
Remove the forceps from the clamp.
Now, release the rubber sheet from wings to lie around thecervical margin of the tooth.
Method III: Split dam technique: This method is split dam technique in which rubber dam is placed to isolate the tooth without the use of rubber dam clamp. In this technique, two overlapping holes are punched in the dam. The dam is stretched over the tooth to be treated and over the adjacent tooth on each side. Edge of rubber dam is carefully teased through the contacts of distal side of adjacent teeth.
Split dam technique is indicated:
• To isolate anterior teeth • When there is insufficient crown structure • When isolation of teeth with porcelain crown is required. In such cases placement of rubber dam clamp over the crown margins can damage the cervical porcelain. • Dam is placed without using clamp. • Here two overlapping holes are punched and dam is stretched over the tooth to be treated and adjacent tooth on each side.
• Fluoride can be toxic, if administered in excess quantity. • The toxic effects of fluoride can be either acute or chronic. • Acute toxicity occurs due to a single ingestion of large amount of fluoride. • Chronic toxicity occurs dụe to long-term ingestion of small amounts of fluoride excessive than the required optimal level.
Acute Fluoride Toxicity: • Acute fluoride poisoning can occur either as a result of accidental ingestion or from deliberate attempts like suicide • This can be from the use of fluoride containing products such as toothpaste, mouth rinse, tablets or household insecticides. • Acute fluoride poisoning can also occur from overfeeds in community and school water fluoridation systems. • Most of the time overfeeds occur in small water supplies.
Terms used in relation to fluoride toxicity: Safely Tolerated Dose (STD): Dose below which symptoms of toxicity are unlikely to occur (1 mg/kg of body weight).
Potentially Lethal Dose (PLD): Lowest dose associated with a fatality.
(5 mg/kg of body weight).
Certainly Lethal Dose (CLD): Survival after consuming this amount of fluoride is unlikely (32-64 mg/kg of body weight).
Features of acute toxicity of fluorides are:
Nausea
Vomiting
Diarrhoea
Abdominal pain
Hypocalcaemia
Acidosis
Progressive hypotension
Ventricular tachycardia and fibrillation.
The ingested fluoride combines with hydrochloric acid in the stomach to form hydrofluoric acid which exhibits a corrosive effect on the gastric mucosa causing nausea, vomiting, diarrhoea and abdominal pain.
*Hypocalcemia is caused by the affinity of fluoride to cations in the serum. **Hypocalcemia is associated with paresthesia, paresis, muscle fibrillation, tetany, convulsions, decreased myocardial contractility and cardiovascular collapse.
Death usually occurs due to:
Convulsions
Cardiac arrhythmias
Coma.
Chronic Fluoride Toxicity: • Long-term ingestion of small amounts of excessive fluoride will lead to chronic fluoride toxicity which is often referred to as fluorosis. • Fluorosis usually affects the bones and the teeth. • Fluorosis of the bone is called as osteofluorosis and the fluorosis of the teeth is called as dental fluorosis.
MANAGEMENT:
REFERENCES:
Pediatric Dentistry: Principles & Practice, MS Muthu(2nd Edition)
NITROUS OXIDE & OXYGEN SEDATION Properties: • Nitrous oxide is a non-irritating, sweet smelling, colourless inorganic gas. • Specific gravity: 1.53 (heavier than air). • This allows nitrous oxide to occupy the region nearest to the alveolar basement membrane by displacing air. • Enables better absorption in the blood stream. • It has low gas partition coefficient i.e, remains insoluble in the blood stream. • Minimally (absorbed) metabolized by the body. • Rapid onset and recovery. • Is a weak anaesthetic with a Minimum Alveolar Concentration (MAC) of 105. • As MAC is 100, it is theoretically impossible to anaesthetize a patient with nitrous oxide alone.
OBJECTIVES: • To reduce or eliminate anxiety. • To reduce untoward movement and reaction to dental treatment. • To enhance communication and patient co-operation. • To raise the pain reaction threshold. • To increase tolerance for longer appointments. • To aid in treatment of the mentally/physically • To reduce gagging.
EQUIPMENT:
INDICATIONS: • Fearful/conscious patients for whom basic behaviour guidance technique have not been successful. • Patient unable to cooperate due to lack of physiological/emotional maturity. • To protect to developing patient’s psyche.(young children) • To reduce patient’s medical risk.
CONTRAINDICATIONS: • May be contraindicated in some chronic obstructive pulmonary diseases. • Patients with severe emotional disturbance or drug related dependencies. • Patients with sickle cell disease. • Patients treated with Bleomycin sulfate
PROCEDURE:
POTENTIAL COMPLICATIONS: • Nausea. • Vomitting • Diffusion Hypoxia. • Claustrophobia Effects Associated with Gas Accumulation: • Tooth pain due to accumulation of gas in sinus cavity. • Vertigo. • Middle Ear Pain.
REFERENCES: • Pediatric Dentistry: Principles and Practice, MS Muthu (2nd Edition). • Pedodontics: Practice and Management, Badrinatheshwar GV.
Wright’s Classification of Cooperativeness of Children in Dental Office (1975)
Wrights classification of children’s operative behaviour under the following categories: • Cooperative children • Children lacking cooperative ability • Potentially cooperative children
Uncontrolled behaviour
Defiant behaviour
Timid behaviour
Tense cooperative behaviour
Whining behaviour
COOPERATIVE CHILDREN: • Most of the children whom we see in day to day practice fall under this category. • They show minimal apprehension and are reasonably released. • These children usually have good rapport with the dentist and the dental team. • They show interest in the dental procedures and often enjoy the situation. • The dentist can work effectively and efficiently with these children. • They follow the guidelines established, perform within the framework provided and present reasonable level of cooperation.
CHILDREN LACKING COOPERATIVE: • Children lacking cooperative ability are in total contrast to the cooperative children as they lack the ability to cooperate because of their mental and physical immaturity due to age or some special condition. • This includes two group of children: One,being very young who are emotionally immature because of age (less than 2% years). These children can pose a major behavior problem and are often referred to as ‘preoperative children or children in pre-cooperative stage.
The second includes children with specific debilitating or handicapping conditions with mental and physical deficiencies. The severity of the condition will not allow them to cooperate like normal children of their same age. These are called special children’ and the number of these children you see in dental office is increasing recently.
POTENTIALLY COOPERATIVE CHILDREN: • These children are otherwise termed as ‘behaviour problem’ children. • They differ from the children lacking cooperative ability because they have the ability to cooperate but they do not. • This can be because of objective/subjective no other face which can influence behavior can children in dental setting. • The behaviour of these children can be modified by different techniques and can become operative children.
Uncontrolled behaviour: • This type of behaviour is seen in a young child of age to 6 years. • The reaction is seen in the form of a tantrum, which may begin at the reception area or even before the child enters the dental clinic. • This behaviour is also known as incorrigible. • It is characterized by tears, loud cry, physical lashing out, flailing of hands and legs. All are suggestive of a state of acute anxiety or fear. • These children are termed as hypermotive by Lampshire. • School age children tend to model their behaviour on adults or other older children. • Uncontrolled and immature behaviour is not seen in older children, but if it is seen there will be deep rooted reasons for it and these children may reveal adjustment problems in other settings. • Immediate measures to manage the uncontrolled behaviour is seen.
UNCONTROLLED BEHAVIOUR
2. Defiant Behaviour:
This behaviour is typical of the elementary school years but can be observed in other age groups also. • Defiant behaviour is controlled to an extent and is distinguished by “I don’t want to’, I don’t need to’, • They protest as they would do at home when they were brought to the dental office against their wish. • These children are often referred to as ‘stubborn’ or ‘spoiled’. • They frequently become highly cooperative after establishment of guidelines for their behaviour and gaining their confidence. • Defiance can be passive as seen in older children approaching adolescence. • Failure of communication results when the dentist tries to involve the child in the dental procedure and the youngster refuses to respond verbally. • He may avoid eye contact and also reject the situation by clenching his teeth when an intraoral exam nation is attempted. • Passive resistance is often observed in older children approaching adolescence. They have the freedom to express their likes and dislikes at home and when brought to the dental office unwillingly their self-image is affected and they rebel.
3.Tense cooperative behavior: • The behaviour of these children is termed borderline. • They accept the treatment and cooperate but are extremely tense, which is typical of these children. • The tension is often revealed by the body language. • The child patient’s eyes may follow the movements of both the dentist and the dental assistant. • A tremor in the voice heard when they speak, perspiration on the palms of the hands or the eye brows are some features of tense cooperative behaviour.
TENSE COOPERATIVE BEHAVIOUR
4. Timid Behaviour: • Timidity is milder when compared to uncontrolled and defiant behaviour but when managed incorrectly they may become uncontrolled. • The timid child may hide behind a parent but usually offers no physical resistance during the separation procedure. • Some may pause or hesitate when given directions. They may sob or whimper out but not cry hysterically. • They lift their hands occasionally to cry but withhold tears. • Reasons for timidity can overprotective home environment, living in isolated areas without any contact with strangers. • They are often overawed by strangers and strange situations.
TIMID BEHAVIOUR
5. Whining Behaviour: • Whining can be seen in timid or tense-cooperative children. • Since whining plays the prominent role in their behaviour, it is described as a separate entity. • They allow the dentist to perform the procedure but whine through out despite encouragement. • They frequently complain of pain. • Whining can be a compensatory mechanism to control their fear. • The cry is controlled, constant and not particularly loud, often without any tears. • Continuous whining can be a source of irritation and frustration to those involved in the treatment and great patience is required in dealing with whining children.
WHINING BEHAVIOUR
REFERENCES: • Pediatric Dentistry: Principles and Practice, MS Muthu (2nd Edition). • Slideplayer.com • Collegevillepediatricdentist.com • Wintergardensmiles.com • Shutterstock.com
THUMB & DIGIT SUCKING : • Digit Sucking is defined as the placement of the thumb/one or more fingers in varying depths into the mouth. • It may be practiced even during intra-uterine (IU) life. • Presence of this habit is quite normal till 3½ – 4 yrs.
ETIOLOGY: A number of theories have been put forward to explain why thumb sucking occurs. The following are some of the accepted ones:
Freudian theory: This theory was proposed by Sigmund Freud in the early part of this century. • He suggested that a child passes through various distinct phases of psychological development of which the oral and the anal phases are seen in the first three years of life. • In the oral phase, the mouth is believed to be an oro-erotic zone. • The child has the tendency to place his fingers or any other object into the oral cavity. • Prevention of such an act is believed to result in emotional insecurity and poses the risk of the child diversifying into other habits.
Oral drive theory of Sears and Wise: Sears and Wise in 1950 proposed that prolonged suckling could lead to thumb sucking.
Benjamin’s theory: • Benjamin has suggested that thumb sucking arises from the rooting or placing reflex seen in all mammalian infant. • Rooting reflex is the movement of the infant’s head and tongue towards an object touching his cheek. • The object is usually the mother’s breast but may also be a finger or a pacifier. • This rooting reflex disappears in normal infants around 7 – 8 months of age.
Psychological aspects: Children deprived of parental love, care and affection are believed to resort to this habit due to a feeling of insecurity.
Learned pattern: According to some authors, thumb sucking is merely a learned pattern with no underlying cause or psychological bearing.
CLASSIFICATION:
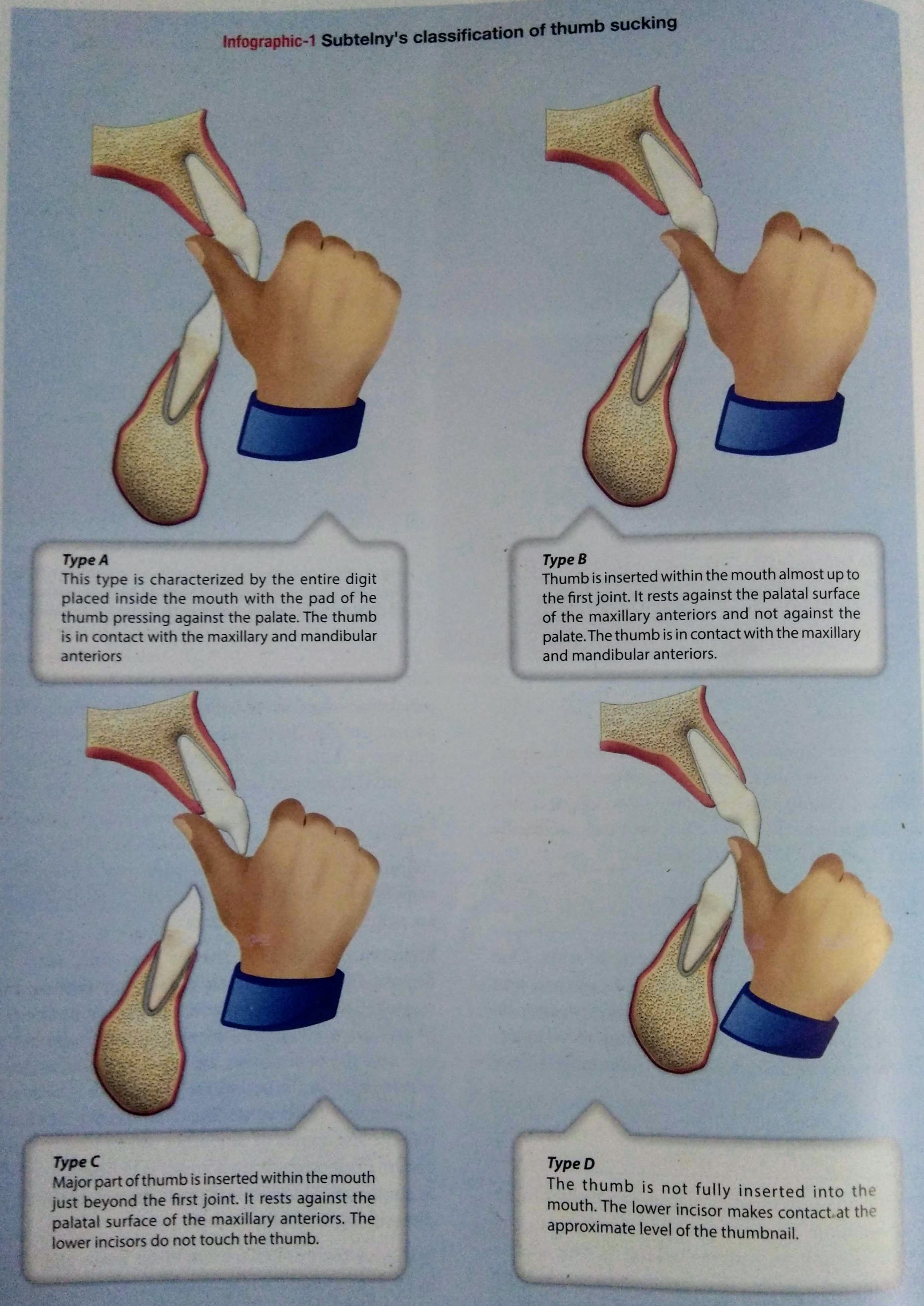
SUBTELNY’ S CLASSIFICATION OF THUMB SUCKING
EFFECTS : The severity of malocclusion caused by thumb sucking depends on:
DURATION: Amount of time spent indulging in the habit.
FREQUENCY : The number of time the habit is activated in a day.
INTENSITY: Vigour with which the habit is performed. The following are some effects:
Effects on Maxilla • Constricted maxilla due to lowered tongue position + buccinator action, while sucking. • V-shaped narrow palate. • Posterior cross-bite may occur. • Increased SNA angle.
2. Effects on Maxillary Teeth: • Spacing in maxillary anterior teeth. • Increased maxillary arch length. • Labial flaring of maxillary anterior teeth.
4. Effects on Thumb: • Presence of clean nails & callus on fingers.
5. Effects on the Lower lip: • Hyperactive lower lip with increased mentalis activity.
6. Effects on the Mandibular Teeth: • Retroclination of lower teeth.
7. Effects on Inter-arch Relationship: • Increased overjet due to flaring of maxillary incisors • Spacing of maxillary anterior teeth. • Increased maxillary arch length. 8. Effects on Tongue: • Lowered tongue position. • Increased chance of developing tongue thrust habit.
MANAGEMENT:
PSYCHOLOGICAL APPROACH: • Parents should be counseled to provide child with adequate love, affection and spend quality time with the child. • Success of any habit interception largely depends on the subject’s willingness to be helped to discontinue his/her habit.
Dunlops Theory of Beta Hypothesis States that the best way to break a habit is by conscious purposeful repititions, i.e the child should be made to sit in front of a large mirror &asked to observe himself as he indulges in the habit.
POSITIVE REINFORCEMENT: • Keeping track of the habit free days and rewarding the child can give the child a sense of pride.
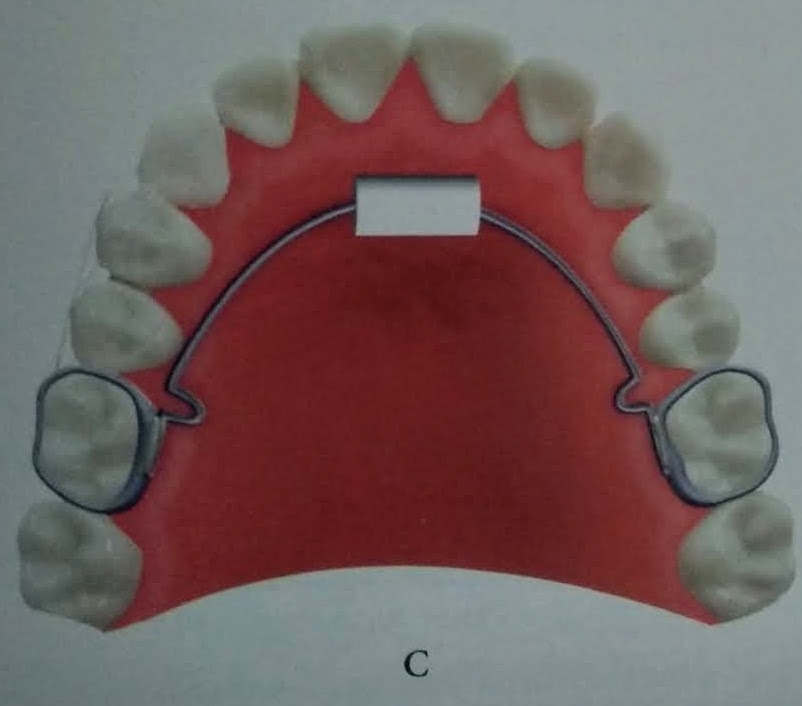
3. MECHANICAL AIDS: • Reminding appliances that assist the child who is willing to quit the habit but is not able to do as the habit has entered a subconscious level. • Following types of habit louis used as mechanical reminding aids in treatment of thumb sucking. REMOVABLE HABIT BREAKER Passive removable appliances, that consist of a crib &is anchored to the oral cavity by the means of clasps on the posterior teeth.
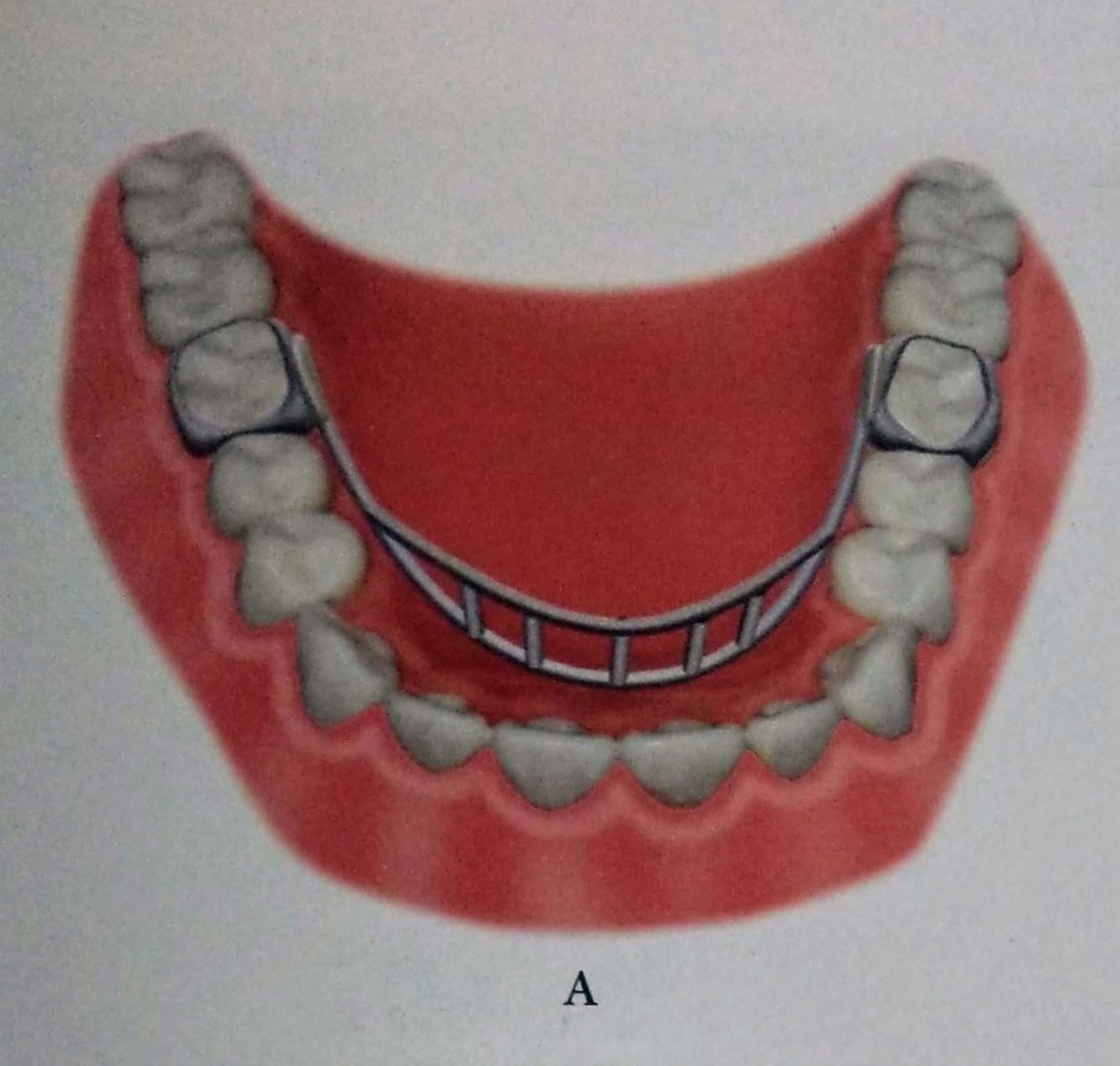
FIXED HABIT BREAKER Heavy gauge stainless steel wire can be designed to form a frame, that is soldered to bands in the molars.
FLAT CRIB THUMB SUCKING APPLIANCE
VERTICAL RAKE APPLIANCE
BLUE GRASS APPLIANCE
VERTICAL CRIB THUMB SUCKING APPLIANCE
4. CHEMICAL APPROACH:
Use of the bitter tasting/foul smelling preparation placed on the thumb, that is sucked can make the habit distasteful.
Pepper dissolved in volatile medium.
Quinine
Asafoetida
REFERENCES:
ORTHODONTICS:The Art & Science,S.I BALAJHI (7th edition)
: • Preventive resin restoration (PRR) is a thin, resin coating applied to the chewing surface of molars, premolars and any deep grooves of the teeth. • They are a natural extension of the use of occlusal sealants. • It consists of an enamel sealant with a resin filling. • If caries is present in one area or parts of pits and fissures, that particular area of caries is restored and fissures are protected with sealants. • It integrates the preventive approach of the sealant therapy for caries susceptible pit & fissure with therapeutic restoration incipient caries with composite resin that occur on the same occlusal surface. • They are the conservative answer to conventional extension for prevention” philosophy of Class I amalgam cavity preparation.
Preventive resin restoration(PRR) consists of a thin, resin coating applied to the occlusal surface of molars, premolars and deep grooves. Most decays begin in the deep grooves. Thus, teeth with this condition are difficult to clean and becomes more susceptible to caries. PRR protects the tooth by sealing the deep grooves and creating a smooth, easy to clean surface. By this way, the teeth is protected from decay for several years, provided they are checked for thinning and wear at regular dental check-ups.
Dental caries is due to the imbalance between loss & gain of
minerals from a tooth surface.
The loss of minerals from our teeth occurs from the bacteria from the foods and producing acids, whereas the tooth gains minerals from our saliva and fluoride that is present within our mouth which over a period of time becomes a tooth decay.
Fissure sealants are a preventive treatment that is part of the minimal intervention dentistry approach to dental care.
This approach facilitates prevention and early intervention, in order to prevent or stop the dental caries process before it reaches the ends stage of the disease.
CLASSIFICATION:
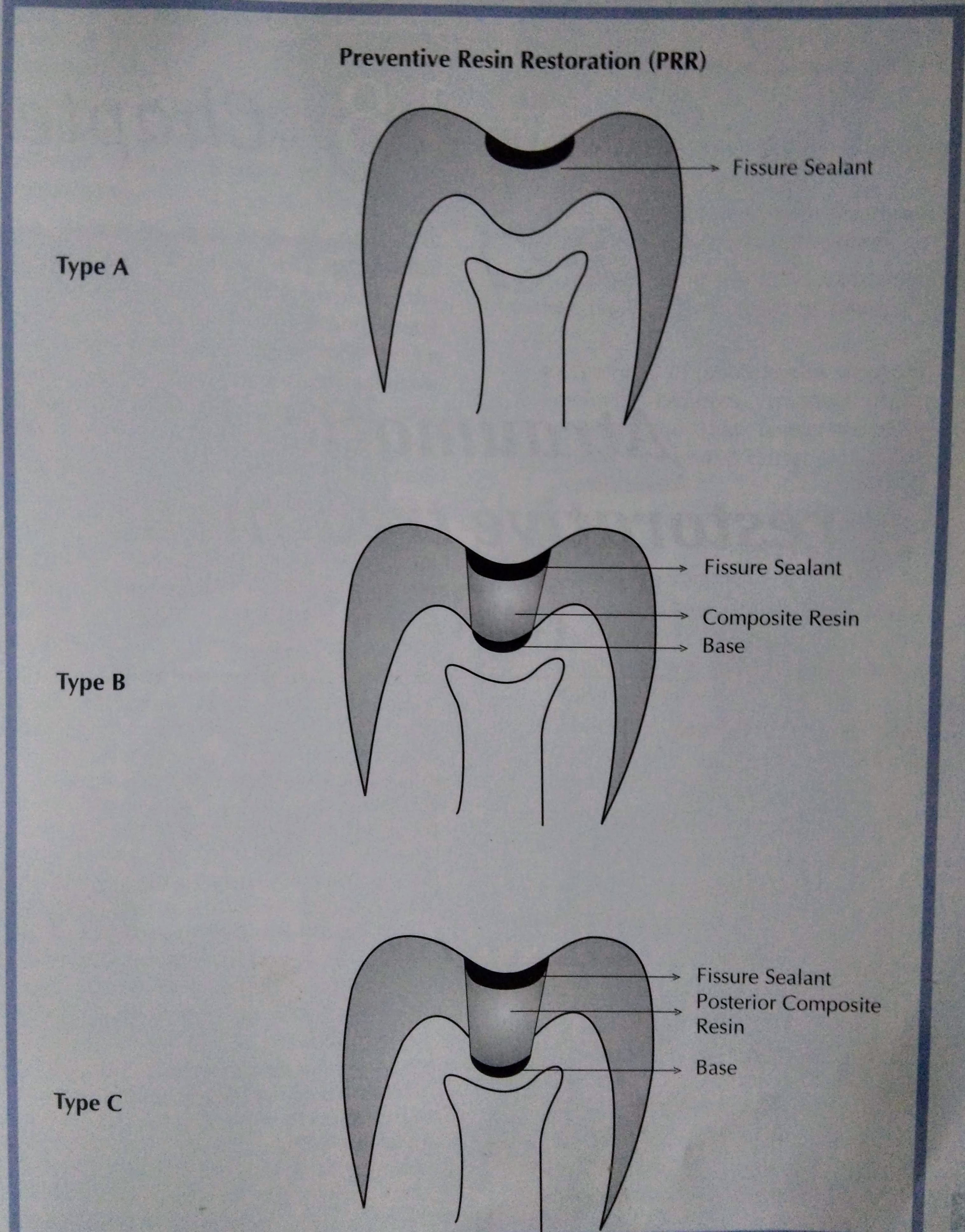
There are three types of preventive resin restoration based on the extent & depth of carious lesion as determined by exploratory preparation.
Simonsen (1978) has classified them:
TYPE A:
• Suspicious pits & fissures where caries removal is limited to enamel • Local anesthesia is not required. • A slow speed 4 or 2 round burs. used to remove decalcified enamel • Sealant is placed
TYPE B:
• Incipient lesion in dentin that is small & confined. • No local anesthesia is needed. • An appropriate base is placed in areas of dentin exposure, composite resin is placed & the remaining pit & fissure are covered with a sealant.
TYPE C: • More extensive dentinal involvement & requires restorations with posterior composite material • Appropriate base is placed over the dentin. • Pits & fissures are covered with sealant. • Local anesthesia is required.
PROCEDURE:
CONCLUSION: • Regular maintenance and sealant addition when necessary is important in long-term caries protection after sealant placement. • Much better effectiveness data will result if sealants are used on teeth with a true predilection to caries. • Better materials and better use of bonding agents with sealants will improve overall effectiveness on all teeth,particularly on those teeth now thought of as difficult to seal. • Use of sealants has proved to have good results. • For prevention of dental caries in pit and fissure, sealants were introduced. • There is evidence suggesting effectiveness of sealants. • Sealants prevent bacteria growth which causes caries. • Biomaterials to seal pit and fissure should present with the simple application method, biocompatibility, low viscosity and good surface retention and low solubility. • To improve this biomaterial, more laboratory should be developed.
REFERENCES:
Essentials of Public Health Dentistry, Soben Peter (6th Edition).
FENESTRA 2002-18, Dr. Bruno Jacquot(Bruno.Jacqout@odonto.u-nancy.fr)