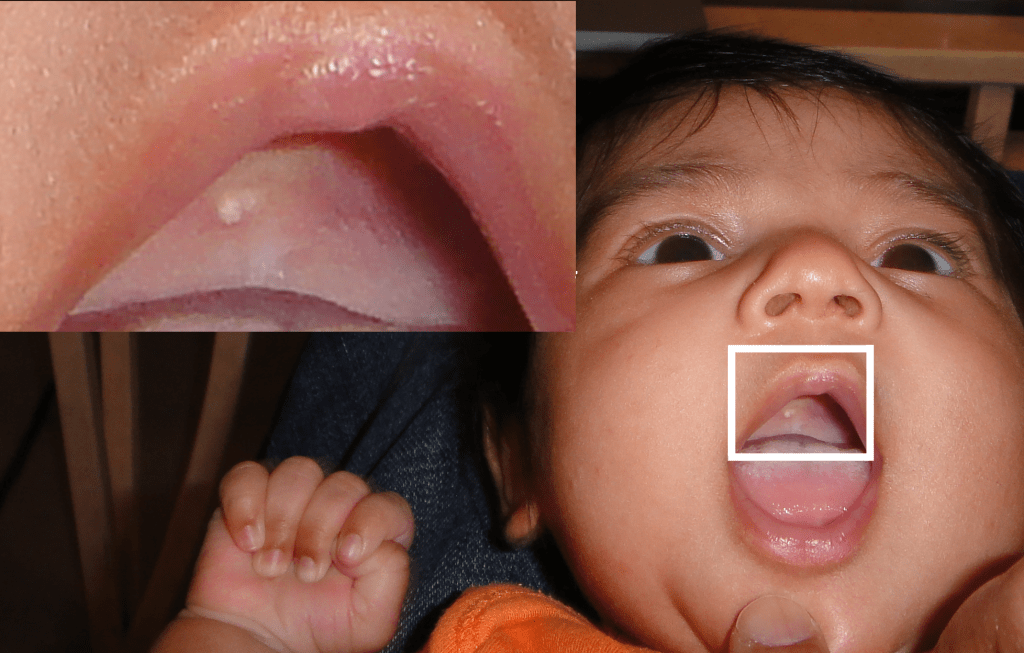
A 2-week-old child had a slow-growing cystic cervical mass. The lesion had been diagnosed by ultrasound before the child was born.

Lymphangiomatous malformations occur in the cervical region as cystic masses (cystic hygroma). The vast majority are diagnosed in the first 2 years of life.
Lymphangiomatous malformations are rare congenital tumors that primarily affect the lymphovascular system, particularly in the head and neck region [1]. These malformations can manifest as lymphangiomatous polypoid lesions, which have histological differences compared to typical lymphatic malformations [1][6]. Lymphangiomatous polyps of the palatine tonsils are particularly rare, with less than 30 reported cases in the literature [2].
When diagnosing lymphangiomatous malformations, it is essential to consider the differential diagnosis. Some conditions that may need to be distinguished from lymphangiomatous malformations include lymphangiectasia, hemangioma, arteriovenous malformation, juvenile nasopharyngeal angiofibroma, fibroepithelial polyps, and papilloma [2]. In rare cases, lymphangiomatous malformations may also present as retroperitoneal cystic lesions or vesicular oral lesions [3][5]. These malformations should be differentiated from retroperitoneal cystic lymphangiomatous malformations, retroperitoneal abscesses, ovarian neoplasms, cystic or necrotic solid tumors, and seminal vesicle cysts [3]. In some cases, lymphangiomatous malformations may be misdiagnosed as other conditions, such as benign cystic mesothelioma [7].
Lymphangiomatous malformations can present with various symptoms depending on the location and size of the lesion. For instance, lymphangiomatous polyps of the tonsils may present with sore throat and dysphagia [10]. Lymphangiomatous macroglossia, on the other hand, is characterized by the chronic enlargement of the tongue and does not spontaneously regress [8]. In terms of management, the treatment options for lymphangiomatous malformations depend on factors such as the location, size, and symptoms of the lesion. Bipolar radiofrequency-induced interstitial thermoablation has been found to be effective for the treatment of oral cavity vascular malformations, including lymphangiomatous lesions [9].
In conclusion, lymphangiomatous malformations are rare, benign tumors that primarily affect the lymphovascular system in the head and neck region. They can manifest as lymphangiomatous polypoid lesions or macroglossia and may present with various symptoms. Diagnosing these malformations can be challenging due to the differential diagnosis with other conditions. The management of lymphangiomatous malformations depends on factors such as the location and symptoms of the lesion. Further research is needed to better understand the pathogenesis and optimal treatment strategies for these rare tumors.
REFERENCES
[1] Park, E., Pransky, S., Malicki, D., Hong, P. (2011). Unilateral Lymphangiomatous Polyp Of the Palatine Tonsil In A Very Young Child: A Clinicopathologic Case Report. Case Reports in Pediatrics, (2011), 1-3. https://doi.org/10.1155/2011/451542
[2] Chen, H., Lovell, M., Chan, K. (2010). Bilateral Lymphangiomatous Polyps Of the Palatine Tonsils. International Journal of Pediatric Otorhinolaryngology, 1(74), 87-88. https://doi.org/10.1016/j.ijporl.2009.08.017
[3] Khan, R., Wahab, S., Chana, R., Fareed, R. (2010). Isolated Retroperitoneal Hydatid Cyst In a Child: A Rare Cause Of Acute Scrotal Swelling?. Journal of Pediatric Surgery, 8(45), 1717-1719. https://doi.org/10.1016/j.jpedsurg.2010.04.019
[4] Andac, S. (2022). Silhouette Lymphangioma: An Unknown Macular Form Of Cutaneous Lymphangioma. Arch Iran Med, 7(25), 456-459. https://doi.org/10.34172/aim.2022.75
[5] (2021). Newborn With Vesicular Oral Lesions. J Paediatr Child Health, 5(57), 759-759. https://doi.org/10.1111/jpc.2_15225
[6] Günbey, E., Gunbey, H., Dölek, Y., Karabulut, Y. (2014). A Rare Cause Of Dysphagia In Children. Journal of Craniofacial Surgery, 4(25), e346-e348. https://doi.org/10.1097/scs.0000000000000773
[7] Shakya, V., Agrawal, C., Karki, S., Sah, P., Poudel, P., Adhikary, S. (2011). Benign Cystic Mesothelioma Of the Peritoneum In A Child—case Report And Review Of The Literature. Journal of Pediatric Surgery, 4(46), e23-e26. https://doi.org/10.1016/j.jpedsurg.2011.01.004
[8] Kim, J., Kwon, H., Rhie, J. (2019). Reduction Glossectomy Of Congenital Macroglossia Due To Lymphangioma. Arch Craniofac Surg, 5(20), 314-318. https://doi.org/10.7181/acfs.2019.00220
[9] Civelek, S., Sayin, I., Ercan, I., Çakir, B., Turgut, S. (2012). Bipolar Radiofrequency-induced Interstitial Thermoablation For Oral Cavity Vascular Malformations: Preliminary Results In a Series Of 5 Children. Ear, Nose & Throat Journal, 11(91), 488-492. https://doi.org/10.1177/014556131209101111
[10] Bhat, S., Patla, S., Rent, N., Shetty, K. (2015). Lymphangiomatous Polyp Of the Tonsil: An Unusual Cause Of Snoring. Otorhinolaryngology Clinics – An International Journal, 2(7), 88-90. https://doi.org/10.5005/jp-journals-10003-1198