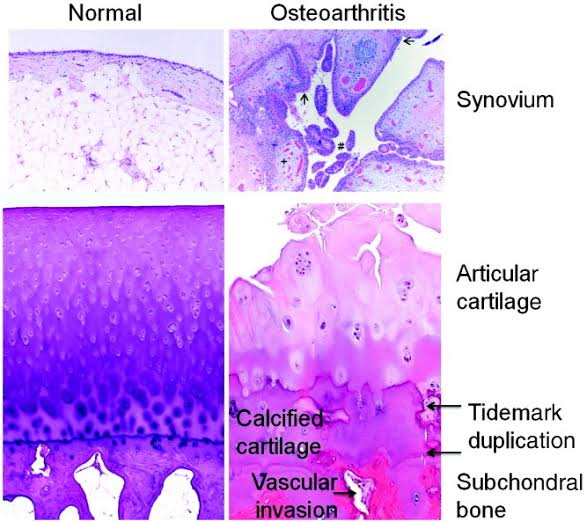
It is histological cannotation to premalignance marked by abbarent and uncoordinated cellular proliferation depicted at cellular level as atypia which is reflected as dysplasia.
An oral precancerous lesion, also called dysplasia, is a growth that contains abnormal cells confined to the lining of the oral cavity, or mouth. This lining is called the mucosa. It covers the inside of the cheeks, the inside of the lips, the gums, the tongue, and the roof and floor of the mouth.
Dysplasia can be mild moderate and severe.
Clinical features :-
Increased mitosis
Loss of basal polarity
Hyperchromatism of cell
Increased nuclear cytoplasmic ratio
Nuclear atypia
Large prominent nucei
Epithelial pearl
Individual cell keratinisation
Treatment :-
NSAIDs for pain and inflammation medical treatment.
Excision of the part which is affected along with some part of healthy tissue. This is done under anesthesia.
Reference :-
Image :- Google Writing :- notes made from mastering bds and Sanjay Kumar Purkait books
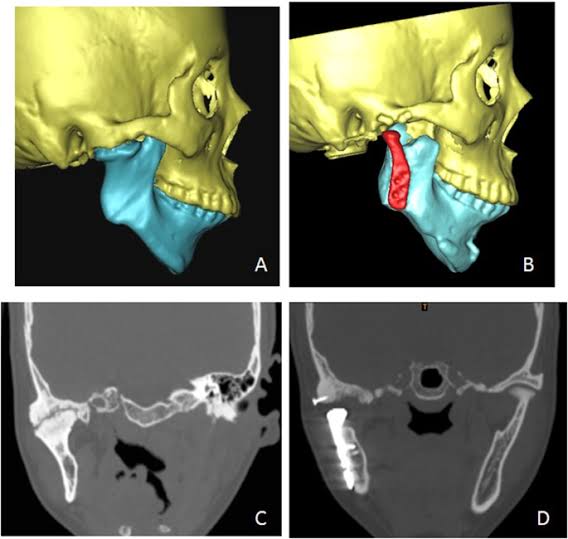
It is one of most incapacitating of all diseases involving this structure.
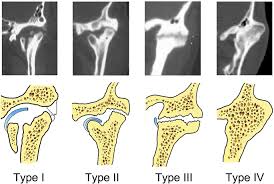
Types :-
In Complete Ankylosis i.e there is limitation of motion.
In Unilateral Ankylosis i.e chin is displaced.
In Intra-articular Ankylosis, joint undergoes progressive destruction.
In Extra-articular Ankylosis, splitting of TMJ.
Clinical features :-
Occurs before 10 years of age
Equal sex distribution
Restriction in opening of mouth
Injury at infancy or childhood, there is associated facial deformity.
Pain may occur in some cases
Inflammation may be seen
Treatment :-
NSAIDS can be use as medical treatment.
Surgical methods like condylectomy intraoral coronoidectomy, ramus osteotomy, high condylectomy, forceful opening of the jaw under general anesthesia, lysis of adhesions of the pterygoid space.
Reference :-
Image :- Google Writing :- notes made from mastering bds and Sanjay Kumar Purkait books
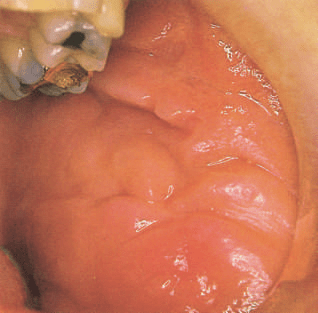
Crohn’s disease is an inflammatory bowel disease of unknown aetiology. However, it shares many features with the autoinflammatory diseases,and some cases are known to be associated with mutations in the gene NOD2 that controls inflammatory responses to bacteria. Mutations cause failure of the formation of the mucin and antimicrobial barrier lining the bowel and may also inhibit degradation of bacteria. Changes in bowel flora are probably also important. Granulomatous inflammation affects the ileocaecal region, causing thickening and ulceration. Symptoms vary with the severity of the disease, but effects can include abdominal pain, variable constipation or diarrhoea and, sometimes, obstruction and malabsorption. Repeated bowel resections may ultimately be needed. Many other sites can be affected including any part of the bowel, joints and skin. Treatment controls symptoms but is not curative. Dietary adjustment, corticosteroids, antibiotics, sulfasalazine or mesalazine, immunosuppressants and tumour necrosis factor (TNF)-alpha blockers (e.g. infliximab) are used.
Oral effects 1)Most patients have no oral signs, although aphthous ulcers and candidosis may be associated with anaemia.
2)When the disease process itself affects the mouth, the signs and symptoms are the same as those in orofacial granulomatosis.
3)Non-caseating granulomas resembling those in the intestine develop in the oral mucosa. The common sites of involvement are lips and buccal mucosa. These show prominent oedema with folds tethered to the underlying deeper tissues, producing the characteristic cobblestone mucosa appearance.
4)Linear ulcers often run along the buccal sulci, particularly the lower sulci, and have hyperplastic folds of inflamed mucosa along their margins. The gingiva show an erythematous nodular gingivitis with hyperplastic tags.
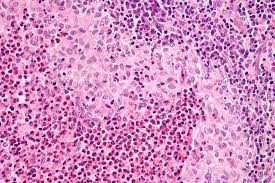
5)The granulomas are typically small, loose and contain few multinucleate giant cells and are often sited deeply in underlying muscle. They may be few in number, and a biopsy needs to extend unusually deeply to increase the chance of finding them because only by identifying granulomas can the diagnosis be made. The granulomas are associated with vascular dilatation and tissue swelling in early disease. Later, there is dense fibrosis that fixes the tissues in their distorted shape.
These features can be the presenting features of Crohn’s disease, and occasionally oral lesions precede gastrointestinal symptoms by a long period. Oral disease is much more likely to progress to bowel disease in children than when diagnosed in an adult.
Typical orofacial features of Crohn’s disease: • Diffuse soft or tense swelling of the lips, or mucosal thickening • Cobblestone thickening of the buccal mucosa, with fissuring and hyperplastic folds • Gingivae may be erythematous and swollen • Sometimes, painful mucosal ulcers, linear in sulci or resembling aphthae • Mucosal tags in sulcuses • Glossitis due to iron, folate or vitamin B12 deficiency can result from malabsorption • Orofacial granulomatosis shares many features
Management
Oral lesions may lessen in severity with treatment of systemic disease. Aggressive treatment is merited in the early stages to prevent fibrosis and permanent disfigurement. The same drugs as are used for bowel disease are required, together with steroid injections of swollen mucosa.
Dr. Iswarya V, BDS
REFERENCE: Cawson’s Essentials of Oral Pathology and Oral Medicine – E. W. Odell