Muhad Noorman P – Final year -Team Dentowesome
Most often we get frustrated by studying for days before exams, often we fail to recollect or forget while writing exams. It’s a quite natural process for a human body to forget.
However there are tricks to master our hippocampus and remember for long. Excelling in exams are only possible based on how much you remember topics.
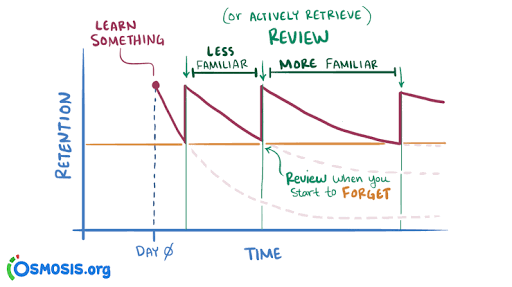
According to Ebbinghaus curve of forgetting information is lost from brain and we’re inable to recollect it.A typical graph of the forgetting curve purports to show that humans tend to halve their memory of newly learned knowledge in a matter of days or weeks unless they consciously review the learned material.

In oder to master long term memorization, we need to practice following methods
Revision : You still remember, A for apple and mitochondria is power house of cell. Constant and frequent revison makes your hippocampus to convert short term memory to long term memory.
Spaced repetition learning technique
Review Your Notes. Within 20-24 hours of the initial intake of information, make sure the information is written down in notes and that you have reviewed them.
Recall the Information for the First Time. Recall the Materials Again.
Study It All Over Again
Difficult topics are checked regularly while easy topics could be reviewed occasionally

Take a break method
Study for 20 minutes take a 5 minute break repeat pattern for 3 to 4 hours. It helps to gain more focus, At the end you’ll be happy for the productive hours. Without break in intervals your brains rejects input eventually your output becomes non productive. Mastering this techinque daily, your graph of productivity hits up.
Use body movements while learning,helps to Tigger muscle memory.
Make a story to memorize long topics. Pieces of information are always connected each other when a story link is given.
Organise your study table. Neat study table and fresh environment boost your intake . Bright light, fresh air, erect spine enhance brain functioning. Feel comfortable stay away from cluttered environment
Try to understand what you learn, things you understand and studied are memorised 9 times.
Learn opposite things .
Switch your topics frequently. Similiar memory get’s intermixed (interference theory).
Things learned at the beginning and end are most memorized. Plan your topics accordingly.
Dicatate your topics and record in dictaphone you can download in your phone. Hear audios before you sleep, going to a beach or restaurant… Brain makes short term memory to long term memory while relaxed.
Visualise your topics. You still remembers the colour of precipitate and titration from your 12th chemistry lab practicals. Visualized memory is far beyond your imaginations.
Read first from books, 2 or 3 days later watch related topics videos from Youtube or any informative apps. Audio+ video learning brushes your previous stored information
Always make use of Sticky notes of alternating colours (prefer light colours- eye rejects dark colour for long time. Use sticky notes apps In your phone screen ( numericals, years etc.could be written in it).
Last days before your exams should be used for rough reading or revison not for studying. Brain rejects things learned in stressed or a state of anxiety .( Your neurotransmitters makes it mess. Respect them 🤣)
Credits : 1) Forgetting curve definition:Wikipedia. Image : Internet. 2) Spaced repetition technique images from Internet and Osmosis.org website . Spaced repetition method content from Google.